
These posters have been presented at meetings in Children's Mercy and around the world. They represent research that was done at the time they were created, and may not represent medical knowledge or practice as it exists at the time viewers access these posters.
-

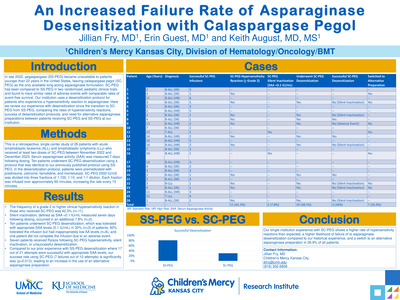
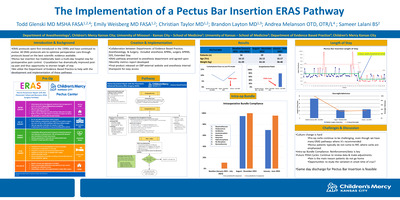
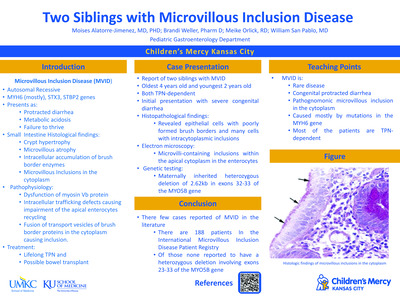
An Increased Failure Rate of Asparaginase Desensitization with Calaspargase Pegol
Jillian Fry, Erin M. Guest, and Keith J. August
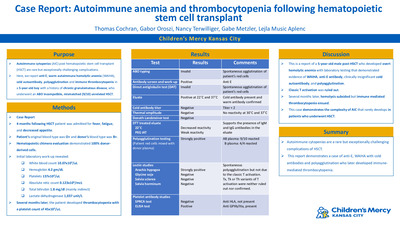
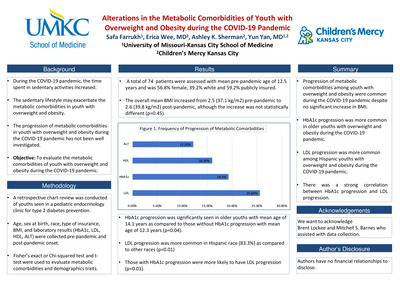
Background: In late 2022, pegaspargase (SS-PEG) became unavailable to patients younger than 22 years in the United States, leaving calaspargase pegol (SC-PEG) as the only available long-acting asparaginase formulation. SC-PEG has been compared to SS-PEG in two randomized, pediatric clinical trials and found to have similar rates of adverse events with comparable rates of event-free survival. Our institution uses a desensitization protocol for patients who experience a hypersensitivity reaction to asparaginase. Here we review our experience with desensitization since the transition to SC-PEG from SS-PEG. Objectives: To compare the rate of hypersensitivity reactions, success of desensitization protocols, and need for alternative asparaginase preparations between patients receiving SC-PEG and SS-PEG at our institution. Design/Method: This is a retrospective, single center study of pediatric patients who received at least 2 doses of SC-PEG between November 2022 and December 2023. Results: We report on 26 patients with acute lymphoblastic leukemia and lymphoblastic lymphoma who received at least two doses of SC-PEG. The frequency of a grade 2 or higher clinical hypersensitivity reaction in those who received SC-PEG was 42.3% (n=11). Silent inactivation, defined as serum asparaginase activity (SAA) <0.1 IU/mL measured seven days following dosing, occurred in an additional 7.8% (n=2). Ten patients underwent SC-PEG desensitization using a protocol that was identical to our previously published protocol using SS-PEG (August, et al., Ped Blood Cancer, 2020). In the desensitization protocol, patients were premedicated with prednisone, cetirizine, famotidine, and montelukast. SC-PEG 2500 IU/m2 was divided into three fractions of 1:100, 1:10, and 1:1 dilution. Each fraction was infused over approximately 60 minutes, increasing the rate every 15 minutes. Desensitization was tolerated with appropriate SAA levels (0.1 IU/mL) in 30% (n=3) of patients, 60% tolerated the infusion but had inappropriately low AA levels (n=6), and one patient did not complete the infusion due to an adverse event. Six patients received Rylaze following SC-PEG hypersensitivity, silent inactivation, or unsuccessful desensitization. Compared to our prior experience with SS-PEG desensitization where 17 out of 21 attempts were successful with appropriate SAA levels (August, et al., ASH, 2022), our success rate using SC-PEG (7 failures out of 10 attempts) is significantly less (p=0.013), leading to an increase in the use of an alternative asparaginase preparation. Conclusion: Our single institution experience with SC-PEG shows a high rate of hypersensitivity reactions, a high likelihood of failure of asparaginase desensitization compared to our historical experience, and the frequent need to switch to an alternative asparaginase preparation.
-

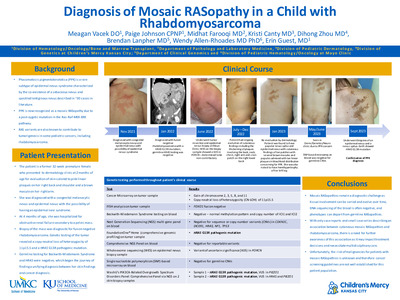
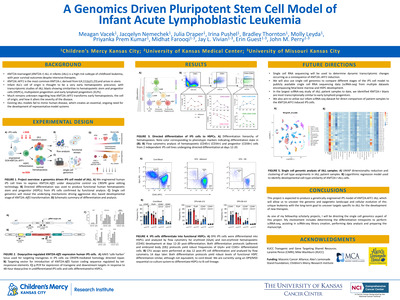
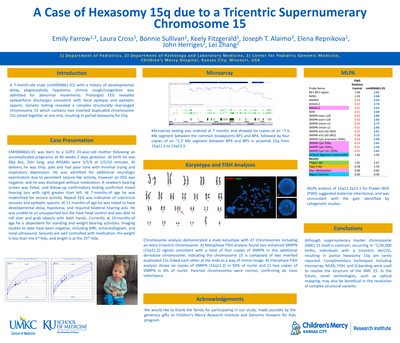
Diagnosis of Mosaic RASopathy in a Child with Rhabdomyosarcoma
Meagan Vacek, Paige Johnson, Midhat S. Farooqi, Kristi M. Canty, Dihong Zhou, Brendan Lanpher, Wendy Allen-Rhoades, and Erin M. Guest
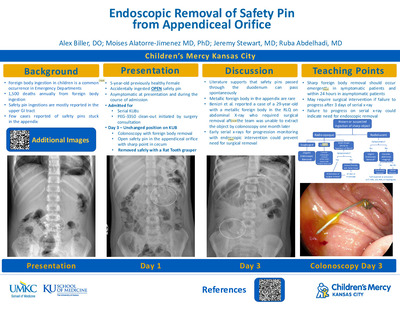
Background: Phacomatosis pigmentokeratotica (PPK) is a subtype of epidermal nevus syndrome characterized by the co-existence of a sebaceous nevus and a speckled lentiginous nevus and described in approximately 30 cases in literature. PPK is now recognized as a mosaic RASopathy due a postzygotic mutation in the Ras-Raf-MEK-ERK pathway. RAS variants are also known to contribute to tumorigenesis, in some pediatric cancers, including rhabdomyosarcoma. Objective: Describe the presentation and evaluation of a child with pelvic rhabdomyosarcoma and evolving skin lesions found to have a rare mosaic-RASopathy. Design/Method: Case Report Results: The patient is a former 32-week premature female who presented to dermatology clinic at 2 months of age for birthmarks on her back and right shoulder. She was diagnosed with epidermal nevi and congenital melanocytic nevi with the possibility of having an epidermal nevus syndrome. At 4 months of age, she was hospitalized for obstructive renal failure secondary to a pelvic mass. Biopsy of the mass was diagnostic for embryonal rhabdomyosarcoma with gain of chromosomes 2, 3, 5, 8 and 11, and copy-neutral loss of heterozygosity of 11p15.5. Molecular testing revealed HRAS G13R mutation in the tumor, but not in a blood sample. Five months after her cancer diagnosis she underwent tumor resection and skin biopsy. Whole exome sequencing of the skin biopsy showed a variant of uncertain significance in PORCN gene. While receiving chemotherapy and post-treatment, her skin lesions continued to evolve with increased size and number of nevi. A single nucleotide polymorphism-based microarray was performed on blood to assess for any germline copy number variants but was negative. Due to ongoing concerns for PPK, she underwent her second and third skin biopsies. The two lesions biopsied and showed the same HRAS G13R mutation as her tumor, confirming a diagnosis of a mosaic RASopathy almost 2 years after her first dermatology visit. Conclusion: Mosaic RASopathies remain a diagnostic challenge. Tissue involvement can be varied and subtle, DNA sequencing of the blood is often negative, and phenotypes can depart from germline RASopathies, even when caused by the same mutation. With only case reports and small case series describing an association between cutaneous mosaic RASopathies and rhabdomyosarcoma, there is a need for further awareness of this association as it may impact treatment decisions. Also, despite cancer screening guidelines for germline RASopathies being well established, they are not available for mosaic cases, leading providers to question future malignancy risks in this patient population.
-

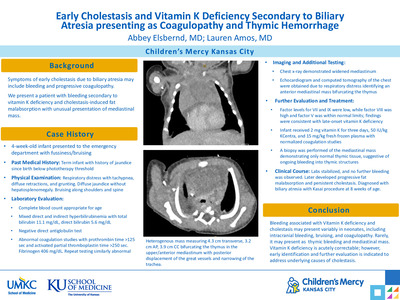
Early Cholestasis and Vitamin K Deficiency Secondary to Biliary Atresia presenting as Coagulopathy and Thymic Hemorrhage
Abbey Elsbernd and Lauren Amos MD
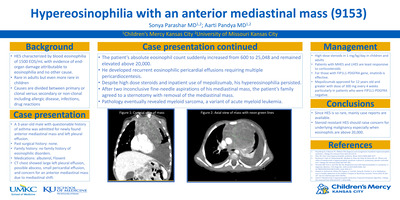
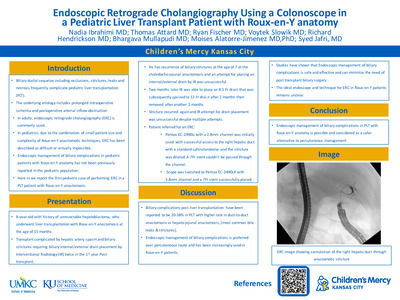
Background Bleeding and progressive coagulopathy are established symptoms of early cholestasis, including extrahepatic biliary atresia. We present a patient with bleeding secondary to vitamin K deficiency and cholestasis-induced fat malabsorption with unusual presentation of mediastinal mass. Objective Describe a case of late-onset vitamin K deficiency and cholestasis ¬¬presenting as jaundice and coagulopathy with associated bleeding into thymic structures Design/Method Case report Results A 4-week-old term male infant was brought to the ED with fussiness and bruising. Prior to presentation, he was afebrile and followed regularly with his primary care provider for jaundice below phototherapy thresholds. Infant received vitamin K at birth. In the ED, infant was tachypneic with retractions and grunting. Physical examination was notable for diffuse jaundice and two 1 cm bruises along shoulder and midline thoracic spine. No hepatosplenomegaly was noted. Chest x-ray was significant for mildly widened mediastinum. Labs demonstrated elevated WBC 19.68 x10(3)/mcL, Hgb 10.8 gm/dL, Platelet count 287 x10(3)/mcL. LFT notable for mixed direct/indirect hyperbilirubinemia with total bilirubin 11.1 mg/dL, direct bilirubin 5.6 mg/dL, indirect bilirubin 5.5 mg/dL. DAT was negative. Coagulation studies were significantly abnormal, with PT >125 sec and aPTT >250 sec; INR was unable to be completed. Fibrinogen was 406 mg/dL. A repeat set of coagulation studies were similarly abnormal. Infant received 2 mg vitamin K for three days, 50 IU/kg KCentra, and 15 mg/kg fresh frozen plasma. Factors VII and IX were low, factor VIII was high, and factor V was normal consistent with late-onset vitamin K deficiency bleeding. Coagulation studies normalized after these interventions. An echocardiogram and computed tomography scan of the chest were obtained due to respiratory distress identifying an anterior mediastinal mass bifurcating the thymus. Due to concern for solid appearance of the mass, a biopsy was completed demonstrating only normal thymic tissue, suggestive of bleeding into his thymic structures as cause of mass. He was able to be discharged with ongoing stability in coagulation labs but with ongoing fat malabsorption and persistent cholestasis. He followed closely with hepatology outpatient and was ultimately diagnosed with biliary atresia with Kasai procedure completed at 8 weeks of age. Conclusion Bleeding associated with Vitamin K deficiency and cholestasis may present variably in neonates, including intracranial bleeding, bruising, and coagulopathy; in this case, our patient presented with thymic bleeding and mediastinal mass. Vitamin K deficiency is correctable in the acute setting, however, early identification and further evaluation is indicated to address underlying causes of cholestasis.
-

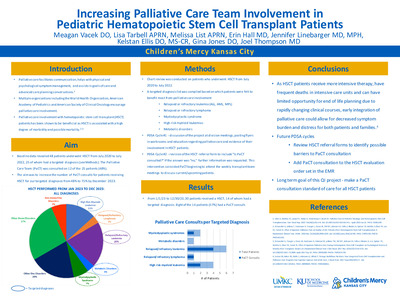
Increasing Palliative Care Team Involvement in Pediatric Hematopoietic Stem Cell Transplant Patients
Meagan Vacek, Lisa Tarbell, Melissa List, Erin Hall, Jennifer Linebarger, Kelstan Ellis, Gina Jones, and Joel Thompson
Background: Palliative care facilitates communication, helps with physical and psychological symptom management, and assists in goals of care and advance care planning discussions.1 Multiple organizations, including the American Academy of Pediatrics and American Society of Clinical Oncology encourage palliative care engagement and their involvement with hematopoietic stem cell transplant (HSCT) patients has been shown to be beneficial as HSCT is associated with a high degree of morbidity and possible mortality.2-3 Objective: To increase the number of PaCT consults for patients receiving HSCT for our targeted diagnoses from 48% to 75% by December 2023. Methods: Chart review was conducted for patients who underwent HSCT from July 2020 to July 2022. Demographics documented included reason for and date of HSCT, date of PaCT consult and living status. A targeted diagnosis list was compiled based on which patients were felt to benefit most from palliative care involvement: relapsed or refractory leukemias and lymphomas, myelodysplastic syndrome, high risk myeloid leukemias and metabolic disorders, such as Hurler syndrome. The first plan-do-study-act (PDSA) cycle included discussion of the project at division meetings and education regarding palliative care and evidence of its involvement in HSCT patients. The second PDSA cycle involved revision of the HSCT referral form to include the question “Is PaCT consulted.” During this time, PaCT also started attending the weekly transplant team meetings to discuss current and upcoming patients. Results: Baseline data from July 2020 to July 2022 revealed 48 patients underwent HSCT, 25 of whom had a targeted diagnosis. PaCT met 12 of the 25 patients (48%). From the initiation of the project on 1/1/23 to 11/30/23, 14 patients with a targeted diagnosis underwent HSCT. Eight of the 14 patients (57%) received a PaCT consult. Conclusions: Palliative care involvement in pediatric oncology is well established, but its role in HSCT patients continues to be explored. As HSCT patients receive more intense therapy, have frequent deaths in intensive care units and can have limited opportunity for end of life planning due to rapidly changing clinical courses, early integration of PaCT could allow for decreased symptom burden and distress for both patients and families.4 Future PDSA cycles to further increase involvement include adding PaCT consultation to the transplant evaluation order set in the electronic medical record and review of the comments on the completed HSCT referral forms to identify possible barriers in the PaCT consultation process.
-

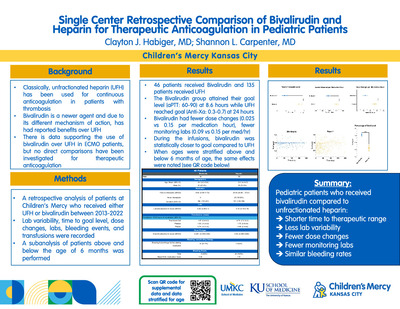
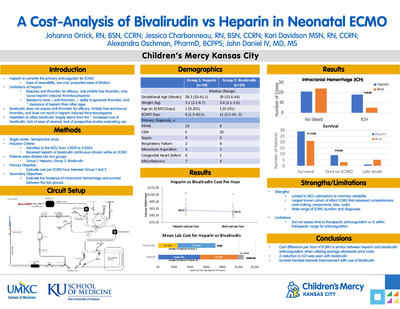
Single Center Retrospective Comparison of Bivalirudin and Heparin for Therapeutic Anticoagulation in Pediatric Patients
Clayton Habiger and Shannon L. Carpenter
Background: The pharmacological choice for continuous anticoagulation therapy in pediatric patients has classically been unfractionated heparin. However, with heparin there are risks of treatment resistance in pediatrics given differences in developmental hemostasis, and contemporary medications such as bivalirudin offer a valuable alternative. Bivalirudin binds to thrombin and has shown encouraging results compared to heparin in pediatric patients receiving ECMO, but no comparison has been made in patients receiving therapeutic anticoagulation. Three years ago, Children’s Mercy Pediatric Hematology department encouraged bivalirudin use over heparin use for therapeutic anticoagulation requiring a continuous infusion. Objectives: Compare clinical and laboratory outcomes in patients receiving bivalirudin and continuous heparin for therapeutic anticoagulation secondary to a thrombotic event. Methods: A retrospective chart review between 1/1/13 to 12/31/22 was performed and looked specifically at patients who had a pediatric hematology consult for therapeutic anticoagulation who were not on ECMO or CRRT. Patients who were on prophylactic dosing or were using the medication for prophylaxis at therapeutic ranges were excluded. Results: 46 patients received bivalirudin during this time while 135 patients received heparin. The time to therapeutic range was significantly shorter in the bivalirudin group compared to the heparin group (3.7 hours vs 18.6, respectively). Additionally, the bivalirudin group had fewer monitoring labs (0.09 vs 0.15), RBC transfusions (0.0019 vs 0.0097), plasma transfusions (0.00074 vs 0.0048), and dose changes (0.025, 0.54) per medication hour (all p<0.05). Both groups had similar rates of bleeding events (6.5% vs 16.3%; p=0.52) despite bivalirudin having more patients who had concurrent bleeding at the time of anticoagulation induction (21.7% vs 5.2%; p<0.05). None of the bivalirudin patients failed to achieve a therapeutic level while 18.6% of heparin patients required a change in anticoagulation due to failure to achieve therapeutic goal. Finally, when monitoring labs (heparinased PTT and Anti-Xa) were standardized to a percentage of goal there was significantly less variation in the bivalirudin group (p<0.001). The average age was older in the bivalirudin group (9.9 vs 1.1) so to account for this, patients were subdivided into under and over 6 months of age. There were 13 bivalirudin and 64 heparin patients who were under the age of 6 months and 33 bivalirudin and 71 heparin subjects older than 6 months of age. The same differences were noted in both subgroups (shorter time to therapeutic range, fewer monitoring labs, RBC transfusions, and dose changes, and more lab monitoring variability). There was no difference in bleeding events in both subgroups when compared with their age cohort. The bivalirudin group had fewer patients with congenital heart conditions (11% vs 47%) and this difference was still noted after subdividing the age groups. Conclusions: Pediatric patients who received bivalirudin had shorter time to a therapeutic range, less lab variability, fewer dose changes, fewer monitoring labs and fewer transfusions with similar bleeding rates compared to patients who received unfractionated heparin.
-

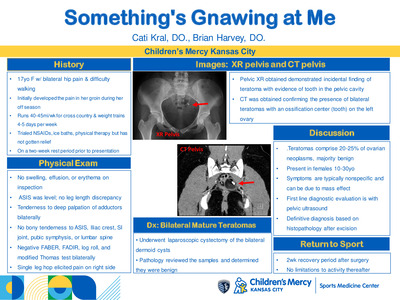
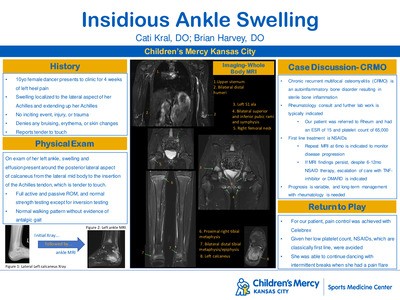
Something's Gnawing at Me
Catharine Kral and Brian Harvey
17-year-old female presented to Sports Medicine clinic with a chief complaint of bilateral hip pain and difficulty walking who was found to have bilateral ovarian teratoma.
-

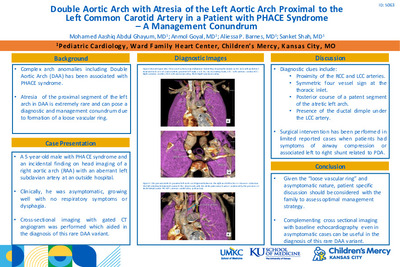
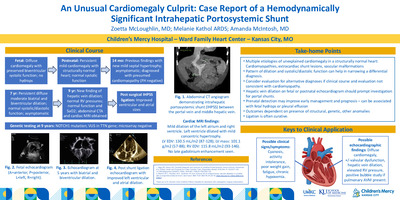
Double Aortic Arch with Atresia of the Left Aortic Arch Proximal to the Left Common Carotid Artery in a Patient with PHACE Syndrome – A Management Conundrum
Mohamed Aashiq Abdul Ghayum, Anmol Goyal, Aliessa P. Barnes, and Sanket Shah
Background Cardiac anomalies in PHACE syndrome (P: posterior fossa anomalies, H: hemangiomas, A: arterial lesions, C: cardiac abnormalities, E: abnormalities of the eye) often consists of complex aortic arch anomalies with double aortic arch (DAA) being an uncommon association. Atresia of the proximal segment of the left arch in DAA is extremely rare and can pose a diagnostic and management conundrum due to formation of a loose vascular ring and asymptomatic nature as seen in our case. Case Description A 5-year-old male, diagnosed with PHACE syndrome, at a different center was noted to have an incidental finding on head imaging of a right aortic arch (RAA) with an aberrant left subclavian artery. He was seen in our center for his follow up after relocation. Clinically, he was asymptomatic, growing well with no respiratory symptoms or dysphagia. His echocardiogram showed RAA with aberrant origin of the left subclavian artery along with the left common carotid from a distal trunk suspicious of a DAA. On cross sectional imaging, a DAA was appreciated with each arch giving rise to a common carotid artery and a subclavian artery with a vertebral artery (Figure 1A and 1B). The presumed portion of the left arch proximal to the common carotid artery did not have any discrete contrast enhancement but the proximity of the left and right carotid arteries suggested ligamentous continuity between the two arches completing the double arch and forming a vascular ring (Figure 2). A ductal dimple was appreciated on the undersurface of the left common carotid suggestive of a left sided ductus (Figure 2). There was no significant tracheal or left mainstem bronchus compression between the pulmonary trunk and distal left arch. Based on the asymptomatic presentation and discussion with family, our consensus was to not intervene surgically. Discussion: The diagnosis of this rare type of DAA with PHACE syndrome has not been previously described to our knowledge. An echocardiogram can assess common arch anomalies associated with this syndrome, however, cross-sectional imaging with CT angiography or MRI can help differentiate this rare diagnosis from its close mimics. Proximity of the right and left carotid arteries, symmetric four vessel sign at the thoracic inlet, posterior course of a patent segment of the atretic left arch and presence of the ductal dimple under the left common carotid are important diagnostic clues that can help differentiate this rare variant of DAA. Although surgical intervention has been performed in limited reported cases, diagnostic accuracy is paramount as patient may remain symptomatic if only the ductal ligament or atretic arch ligament is divided and the other left intact. Given the “loose vascular ring” and asymptomatic nature, patient specific discussion should be considered with the family to assess optimal management strategy. Conclusion: Aortic arch anomalies are common in PHACE syndrome, however, rare variants of DAA can be seen. Keeping a high index of suspicion and complementing cross sectional imaging with baseline echocardiography even in asymptomatic cases can be useful for diagnostic and management considerations as seen in our case.
-

Transposition of the great arteries with intramural left main coronary artery: Salient imaging findings and description of two operative techniques
Joshua Holbert, Manasa Gadiraju, Sanket Shah, and Edo Bedzra
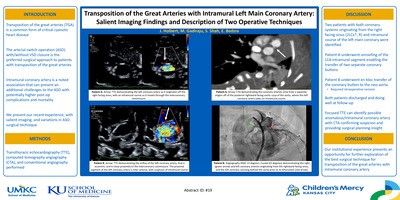
Background: Transposition of the great arteries (TGA) is a common cyanotic critical congenital heart disease, with a feasible prenatal diagnosis. Arterial switch operation (ASO) with/without VSD closure is the preferred surgical approach with added challenge when an intramural coronary artery (IMC) is present. ASO is technically quite demanding with IMC, and incidence of post-operative complications and mortality are potentially higher. We present our recent TGA-IMC experience focusing on salient features identified on echocardiography, CT and invasive angiograms, as well as variations in ASO surgical techniques for repair. Methods: Our echo imaging acquisition required high frequency transducers and shallow image depth in the para-sternal short axis plane, with focus on the aortic root; color Flow Doppler optimization with narrow color box, CF Color Setting and low Nyquist limit was also used. CT angiograms were performed with retrospective gating and breath-hold, after contrast bolus of an Omnipaque-240 contrast/saline mixture (70%-30%). Images were obtained at normal neonatal heart rate of 140s/min with appropriate dose reduction technique. Invasive angiograms were performed in the cardiac Cath lab, with balloon occlusion aortograms using a 5Fr Berman catheter and a combination of camera angulations. Results/Discussion: Two consecutive patients with TGA/intact ventricular septum and intramural left main coronary artery were identified. Both coronary artery systems originated from the right facing sinus in TGA (2 R, AD, Cx Leiden classification). The left main coronary artery had an intramural course, coursing through the pulmonary/septal/posterior commissure and then normally bifurcated to left anterior descending and circumflex arteries. Echocardiographic hallmark for the intramural course was the side-by-side origins of the two coronary arteries from the same sinus and the LCA course between the commissure and the aortic wall. On CT angiogram, key findings were an acute angle origin and subtle caliber change at the extramural coronary exit. Two different surgical approaches were undertaken. In one, the coronary button to be taken en bloc for transfer to the neo-aorta. Ischemia due to inadvertent left coronary artery injury, necessitated patch augmentation of the left main coronary artery. In the other, unroofing of the LCA intramural segment into sinus 1 enabled the transfer of two separate coronary buttons. Both patients had an uneventful subsequent post-operative course. Conclusion: Transposition of the great arteries with intramural left or right coronary artery presents a surgical challenge during ASO repair. By focused trans-thoracic echocardiography, anomalous/intramural coronary artery in TGA can be suspected. The intramural course can be confirmed by ECG gated CT angiograms, with measurement of intramural length, which can assist in operative planning. A recent report from a single center series suggest coronary unroofing with separate 2-button coronary transfer may be associated with lower risk of coronary and ischemic complications. Our limited experience suggests advance imaging with CT angiograms can help determine length of intramural segment, and feasibility of coronary artery unroofing, and 2-button transfer technique. Our institutional experience presents an opportunity for further exploration of the best surgical technique for TGA-IMC with a multi-center approach and longer term follow-up.
-

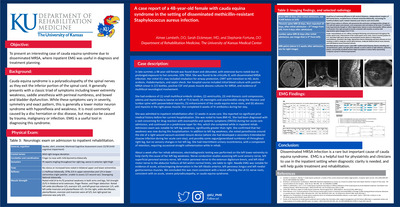
A case report of a 48-year-old female with cauda equina syndrome in the setting of disseminated MRSA infection
Aimee Lambeth, Sarah Eickmeyer, and Stephanie Fortune
To present an interesting case of cauda equina syndrome due to disseminated MRSA, where inpatient EMG was useful in diagnosis and treatment planning.
-

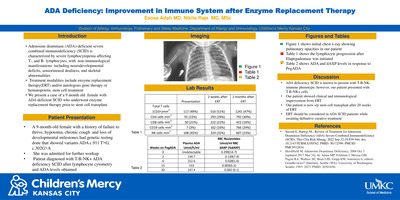
ADA Deficiency: Improvement in Immune Function after Enzyme Replacement Therapy
Esosa Adah and Nikita Raje
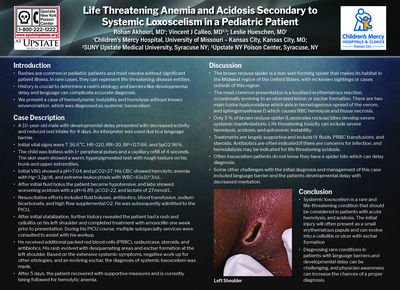
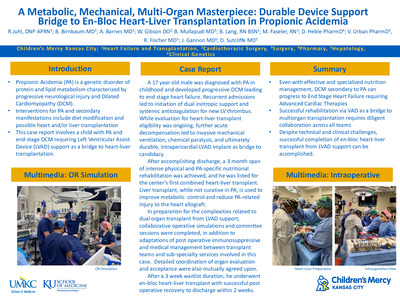
Introduction: Adenosine deaminase (ADA)-deficient severe combined immunodeficiency (SCID) is characterized by severe lymphocytopenia affecting T-, and B-,lymphocytes, with non-immunological manifestations including neurodevelopmental deficits, sensorineural deafness, and skeletal abnormalities. Treatment modalities include enzyme replacement therapy(ERT) and/or autologous gene therapy or hematopoietic stem cell treatment. We report a 9-month-old female with ADA deficient T-B-NK+ SCID treated with ERT while awaiting stem cell treatment. Case Description: A 9-month-old female with a history of failure to thrive, hypotonia and loss of developmental milestones had genetic testing done that showed variants ADA c.911 T>G, c.302G>A. She was admitted for further work up. Lymphocyte subsets showed CD3 117 mm ^3, CD4 55 mm^3, CD8 50 mm ^3, CD19 7 mm^3, and CD 16/56 cells 108 mm^3. Patient was diagnosed with T-B-NK+ SCID. ADA level noted to be
-

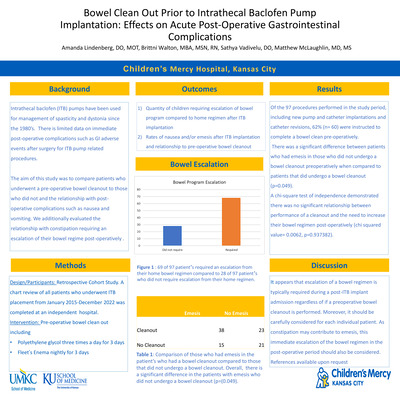
Bowel Cleanout Prior to Intrathecal Baclofen Pump Implantation: Effects on Acute Post- Operative Gastrointestinal Complications
Amanda Lindenberg, Brittni Walton, Sathya Vadivelu, and Matthew J. McLaughlin
Background: Intrathecal baclofen (ITB) pumps have been used for management of spasticity and dystonia There is limited data on immediate post-operative complications such as GI adverse events after surgery for ITB pump related procedures. This study aimed to compare patients who underwent a pre-operative bowel cleanout to those who did not and the relationship with post-operative nausea, vomiting and constipation requiring an escalation of their bowel regimen. Design: Retrospective cohort study. Setting: Pediatric acute care hospital. Participants: All patients who underwent new ITB pump and/or catheter placement from January 2015-December 2022. Interventions: Preoperative bowel clean out. Main Outcome Measure: Quantity of children requiring escalation of bowel program compared to home regimen after ITB implantation and rates of nausea and/or emesis after ITB implantation. Results: Of the 97 procedures performed in the study period, including new pump and catheter implantations and catheter revisions, 62% (n= 60) were instructed to complete a bowel clean pre-operatively. There was a significant difference between patients who had emesis in those who did not undergo a bowel cleanout preoperatively when compared to patients that did undergo a bowel cleanout (p=0.018). A chi-square test of independence demonstrated there was no significant relationship between performance of a cleanout and the need to increase their bowel regimen post-operatively (chi squared value= 0.0062, p=0.937382). Conclusions: Overall, it appears that escalation of a bowel regimen is typically required during a post-ITB implant admission regardless of if a preoperative bowel cleanout is performed. Therefore, it should be carefully considered for each individual patient. As constipation may contribute to emesis, an immediate escalation of the bowel regimen in the post-operative period should be considered.
-

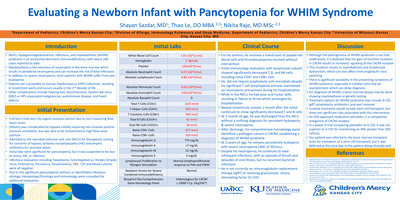
Evaluating a Newborn Infant with Pancytopenia for WHIM Syndrome
Shayan Sazdar, Thao Le, and Nikita Raje
Introduction Warts, hypogammaglobulinemia, infections, and myelokathexis (WHIM) syndrome is a rare immunodeficiency caused by a gain-of-function mutation in CXCR4. A complication of WHIM syndrome is severe neutropenia, which can result in fatal bacterial infections. Given the rarity of the disease and variability of clinical presentations, WHIM syndrome can be difficult to diagnose and manage. Case Description A full term male infant was hospitalized for hypoxic ischemic encephalopathy after delivery. Physical exam was unremarkable. During his hospitalization, he was found to have progressive pancytopenia. Initial lymphocyte subsets showed a significant T cell lymphopenia of 1325 mm3 CD3+, 920 mm3 CD4+, 390 mm3 CD8+, 42 mm3 CD19+, and natural killer (NK) cell count of 28 mm3. Naive CD4+ and CD8+ counts were also low. Immunoglobulin levels, lymphocyte to proliferation for mitogen, newborn screen, Epstein-Barr virus, and parvovirus were normal. Repeat lymphocyte subsets showed persistently low T, B, and NK cells without improvement. A comprehensive bone marrow panel showed a pathogenic variant in CXCR4. At two-years-of-age, he continues to have severe neutropenia. He has not had severe infections and has not required granulocyte-colony stimulating factor (G-CSF) therapy. Discussion WHIM syndrome may not present with all features. Treatment may include G-CSF, immunoglobulin replacement, prophylactic antibiotics, wart destruction, and stem cell transplant. A potential new treatment is plerixafor, which is a competitive antagonist of CXCR4. Its effectiveness and safety compared to G-CSF has not been established. Despite multiple treatment options, there is no standardized treatment. Early diagnosis and standardized therapy may help with preventing disease progression.
-

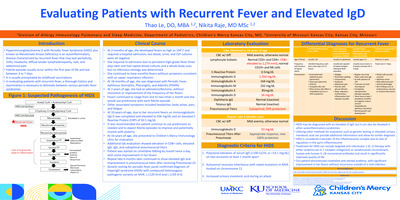
Evaluating Patients With Recurrent Fever and Elevated IgD
Thao Le and Nikita Raje
Introduction: Hyperimmunoglobulinemia D with periodic fever syndrome (HIDS) often presents within the first year of life. Symptoms include fevers, chills, headache, lymphadenopathy, and abdominal pain. Patients may be misdiagnosed as other autoinflammatory syndromes, resulting in delay of treatment. Case: A 16-year-old female presented for evaluation of recurrent fever. Her fevers started at two months of age, occurred one to two times a month, and were associated with headache, abdominal pain, and fatigue . At 18-months, she was diagnosed with periodic fever, aphthous stomatitis, pharyngitis, adenitis (PFAPA). She was treated with prednisone and an adenotonsillectomy but her fevers persisted. . At 10-years of age, she had an immunoglobulin (Ig) D level of 936 mg/dL, normal lymphocyte subsets, tetanus, and diphtheria titers. Repeat IgD was 56 mg/dL, but other immunoglobulins were normal. Pneumococcal titers were suboptimal but showed an adequate response after administration of pneumococcal booster vaccine. She was started on cimetidine 600mg twice a day, with reduced frequency in her fevers. A repeat IgD was 52mg/dL. Genetic testing showed two pathogenic variants of mevalonate kinase (MVK), confirming the diagnosis of HIDS. She was prescribed interleukin-1 (IL-1) inhibitor therapy. Discussion: HIDS is diagnosed by an elevated IgD greater than 100 IU/mL or 14.1mg/dL on two occasions at least a month apart. However, IgD can be elevated in other autoinflammatory syndromes. Genetic testing for mutations in MVK or an elevated urinary mevalonic acid can further confirm diagnosis. This may allow for earlier diagnosis and initiation of treatment with IL-1 inhibitors.
-

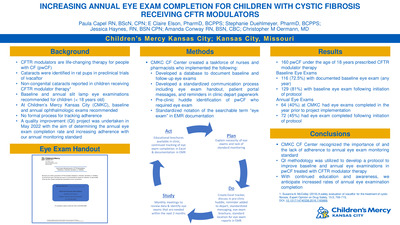
Increasing annual eye exam completion for children with cystic fibrosis receiving CFTR modulators
Paula Capel, Claire Elson, Stephanie Duehlmeyer, Jessica Haynes, Amanda Conway, and Christopher M. Oermann
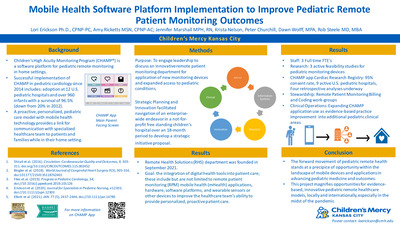
Background: CFTR modulators are life-changing therapy for people with CF. During preclinical studies of ivacaftor, cataracts were identified in juvenile rat pups. Subsequently, noncongenital cataracts have been reported in children receiving CFTR modulator therapy [1], so baseline and annual slit lamp eye examinations for cataract development are recommended for children with CF (aged <18). At Children’s Mercy Kansas City (CMKC), our standard practice is to conduct baseline and annual ophthalmologic examinations to assess for cataracts in children with CF prescribed CFTR modulator therapy, but there was no formal process for tracking adherence to this standard and ensuring that examinations were completed. A quality improvement project was undertaken in May 2022 to determine the rate of completion of annual eye exams and increase adherence to our annual monitoring standard.
Methods: To improve adherence to annual monitoring standards, a quality improvement taskforce including CF care team nurses and pharmacists was developed. A database was used to document baseline and follow-up eye examinations. A standardized communication process was developed and deployed that included an eye exam brochure (Figure 1), messaging to caregivers and patients through the electronic medical record (EMR), and reminders on clinic departure or discharge paperwork. Additionally, children with CF who required eye examinations were identified during preclinic huddles, and that information was communicated to the CF care team. To improve tracking of completed eye exam reports, standardized notation of the searchable term “eye exam” was included in EMR documentation.
Results: At CMKC, at least one eye examination was documented for 116 (72.5%) of 160 children with CF prescribed CFTR modulator therapy before implementation of the quality improvement project; after implementation, eye examinations were documented for 129 (81%). 64 (40%) children with CF at CMKC had eye exams completed in the year before project implementation. After project implementation, 72 (45%) PwCF had an eye exam completed per monitoring recommendations.
Conclusions: Using quality improvement methodology, the CMKC CF care team developed a tracking tool and standardized process for communicating annual eye examination education in children with CF prescribed CFTR modulators. An increase in the rate of annual eye exam completion of 5% was observed after implementation of the process. With continued education and awareness, we anticipate higher rates of annual eye examination completion.
-

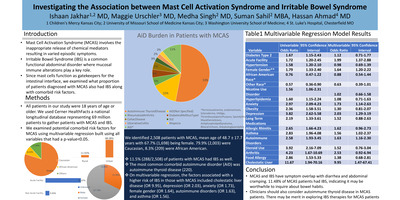
Investigating the Association between Mast Cell Activation Syndrome and Irritable Bowel Syndrome
Ishaan Jakhar, Maggie Urschler, Medha Singh, Suman Sahil, and Hassan Ahmad
Investigating the Association between Mast Cell Activation Syndrome and Irritable Bowel Syndrome Introduction Mast Cell Activation Syndrome (MCAS) involves the inappropriate release of chemical mediators resulting in varied episodic symptoms. Irritable Bowel Syndrome (IBS) is a common functional abdominal disorder where mucosal immune alterations play a key role. Since mast cells function as gatekeepers for the intestinal interface, we examined what proportion of patients diagnosed with MCAS also had IBS along with comorbid risk factors. Methods All patients in our study were 18 years of age or older. We used Cerner Healthfacts to gather our cohorts of patients with MCAS, IBS. We examined potential comorbid risk factors for MCAS using multivariable regression. Results We identified 2,508 patients with MCAS, mean age of48.7 ± 17.7 years with 67.7% (1,698) being female. 79.9% (2,003) were Caucasian, 8.3% (209) were African American. 11.5% (288/2,508) of patients with MCAS had IBS as well. The most common comorbid autoimmune disorder (AiD) was autoimmune thyroid disease (220). On multivariable regression, the factors associated with a higher risk of IBS in those with MCAS included cholestatic liver disease (OR 9.95), depression (OR 2.03), anxiety (OR 1.73), female gender (OR 1.64), autoimmune disorders (OR 1.63), and asthma (OR 1.56). Conclusions MCAS and IBS have symptom overlap with diarrhea and abdominal cramping. 11.48% of MCAS patients had IBS, indicating it may be worthwhile to inquire about bowel habits. Clinicians should also consider autoimmune thyroid disease in MCAS patients. There may be merit in exploring IBS therapies for MCAS patients.
-

Privacy preserving self-service DeGAUSS Based Geomarker Portal
Harpreet Gill, Kushal Vallambhatla, Mark A. Hoffman, Kevin Power, and Catherine Jackson
DeGAUSS offers a privacy-preserving capability to annotate a list of addresses with geomarker information that is useful for social determinants and other research. The standard delivery of DeGAUSS requires command line proficiency, potentially limiting the group of users. We provide a self-service portal that enables researchers to load a file and receive a downloadable annotated output file. In our pilot phase, the system has processed 481 calls for more than 45,000 addresses at Children’s Mercy.
-

Candida Chorioretinitis in Immunocompromised Patient with Candida Tropicalis Fungemia Secondary to Chemotherapy
Jourdan Valkner Krause
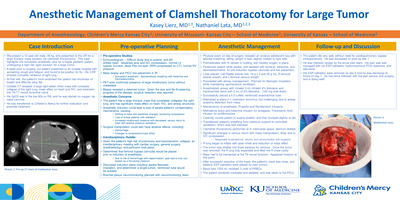
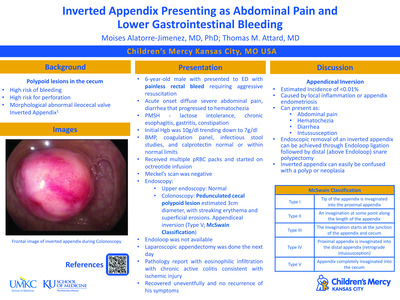
Summary: An immunocompromised patient with candida tropicalis fungemia secondary to chemotherapy presented for follow up of candida chorioretinitis. This infection puts the patient at high risk for CNVM formation and must be followed closely. Case History: • 3-year-old Hispanic female • CC: Candida chorioretinitis follow up • POH: Bilateral orbital chloromas and optic nerve atrophy • PMH: Acute myeloid leukemia, Candida tropicalis fungemia • Meds: o Amphotericin B liposomal 85 mg 42.5 mL, IV, q24hr o Flucytosine 500 mg Capsule *NF* 1,000 mg 2 capsule, PO/NG, q6hr o Micafungin 100 mg 100 mL, IV, q24hr *Plus numerous chemotherapy, pain and other systemic medications. Pertinent Findings: •Clinical: o DFE: One small, <1/2 disc diameter, white lesion inferior to macula OD. Slightly elevated with pigmented borders • Physical: o Immunocompromised • Laboratory testing: o Culture confirmation of Candida tropicalis fungemia o MRI: innumerable foci of nodular and ringlike contrast enhancement involving the brain, brainstem, and cerebellum most compatible with CNS dissemination of fungal disease. There is additional dissemination of fungal disease with involvement of the orbits and scalp. The presence of restricted diffusion within the rim-enhancing collection of the right orbit as described on the CT examination is most compatible with an abscess. Differential Diagnosis: • Toxoplasmosis • White dot syndrome • Cotton wool spot • Retinal tuft Diagnosis Discussion: Immunocompromised patients are susceptible to life threatening infections that are otherwise rare in the immunonormal. With any concern for infection, a thorough work up is needed to initiate proper treatment quickly. In this patient, cultures were positive for Candida tropicalis fungemia. Amphotericin B, micafungin and flucytosine were started. A baseline eye exam was performed and bilateral candida chorioretinitis was diagnosed. Two lesions near the macula OD and one lesion in the periphery OS were observed. After continuous antifungal treatment, only one lesion with pigmented edges remained near the macula OD and no lesions OS at 1 month follow up. With no additional signs to suggest active infection, pigmentation around the remaining lesion led to diagnosis of inactive candida chorioretinitis. Treatment/Management Discussion: Although the infection appears to be inactive, it is crucial to follow this patient every 6 weeks while the patient remains immunocompromised due to high risk of reactivation. There is also risk of CNVM formation. With the lesion’s close proximity to the macula, this must be carefully monitored with DFE and fundus imaging at every 6 week exam. In addition, it is anticipated the reflex seen during retinoscopy will be altered if changes to the macula occur. Alteration in the reflex would be an additional sign leading to the assumption the disease has progressed. The patient should continue taking systemic antifungals as prescribed by infectious disease team until instructed otherwise. Due to this patient’s young age, and still being within the visual development period, it is important to monitor for amblyopia since the lesion resides within the macula. With the patient having equal 20/50 acuity OD and OS, no amblyopia treatment is indicated at this time, but will be closely watched. Conclusion: Immunocompromised patients are predisposed to life threatening infections. In individuals with a history of infection, it is imperative to follow them closely, no matter if the infection is active or inactive. This group is at a higher risk of reactivation, thus should be monitored until the immune system recovers. In patient’s with any form of chorioretinitis, there is a risk of CNVM formation, even once immunonormal. Careful DFE and imaging should be performed at every follow up.
-

Dexamethasone for BPD while on Non-invasive positive pressure ventilation
Priya Tiwari, Jansynn Radford, Michael Norberg, and Alain Cuna
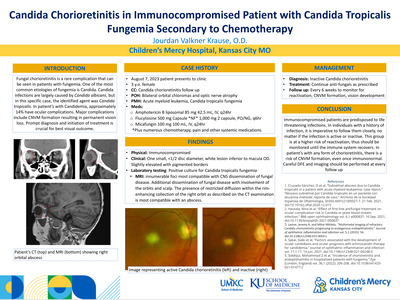
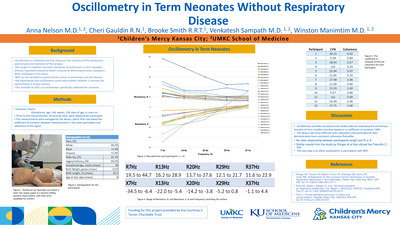
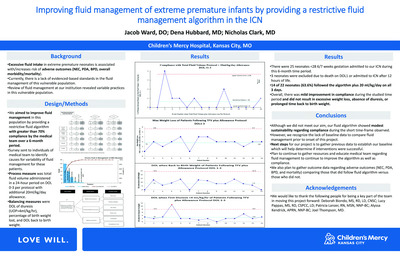
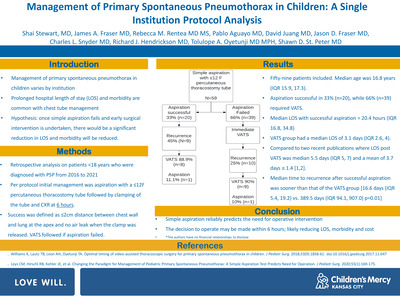
Background: Postnatal dexamethasone (DEX) has traditionally been reserved for preterm infants on prolonged mechanical ventilation, with reported rates of successful extubation at 47% to 76%. Recent emphasis on avoiding mechanical ventilation has resulted in preterm infants being increasingly supported with chronic non-invasive ventilation (NIV). The use of DEX for weaning preterm infants on chronic NIV remains largely unexplored. Objective: To determine efficacy of postnatal DEX in weaning infants on chronic NIV, and to identify factors and outcomes associated with successful weaning. Methods: Single-center retrospective study (2010-2022) of preterm infants ≤32 weeks gestation treated with postnatal DEX while on chronic NIV. Data on baseline demographics, respiratory characteristics at start and end of treatment, and clinical outcomes were collected. Primary outcome was rate of successful weaning from NIV to high-flow nasal cannula (HFNC). Other outcomes included factors and outcomes associated with successful weaning. Results: A total of 56 infants (mean gestational age 26 weeks, mean birth weight 890 grams) received postnatal DEX while on NIV. The average postnatal day and postmenstrual age at time of treatment were 78 days and 37 weeks, respectively. DEX treatment resulted in a significant decrease in oxygen and ventilation support from baseline to end of treatment (Fig 1). Overall, the rate of successful weaning to HFNC was 46% (26/56). Infants treated with postnatal DEX for the first time had similar rates of successful weaning compared to infants who had received prior DEX treatment (43% vs 39%, P =0.79). Factors associated with successful weaning to HFNC were earlier age and lower NIV and oxygen support at time of DEX treatment (Table 1). Infants with successful weaning were more likely to be discharged earlier with less bronchopulmonary dysplasia and less retinopathy of prematurity compared to infants with unsuccessful weaning (Table 2). Other complications of prematurity were similar between the two groups (Table 2). Conclusion: In our level IV NICU, efficacy of postnatal DEX to wean infants on chronic NIV was 46%. Our results suggest that DEX may also be useful in infants on chronic NIV, but further studies are needed to fully determine efficacy and safety.
-

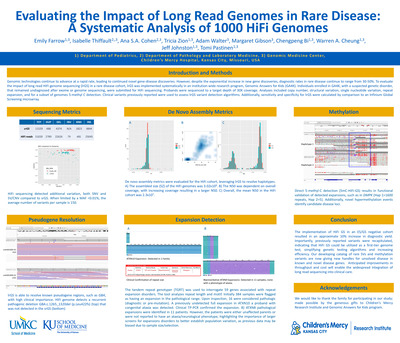
Factors associated with respiratory pathogen panel utilization in children hospitalized with acute respiratory illness — New Vaccine Surveillance Network, Kansas City, 2017–2021
Edward Lyon, Brian R. Lee, Benjamin Clopper, Heidi L. Moline, Rangaraj Selvarangan, and Jennifer Schuster
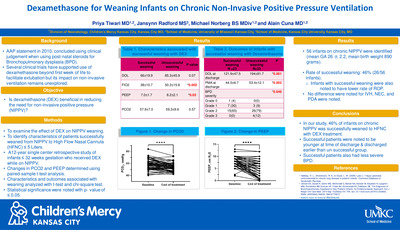
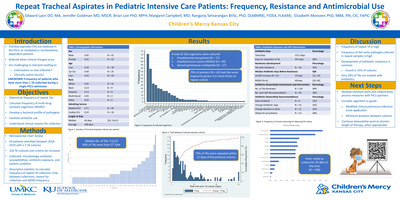
Background: Respiratory pathogen panels (RPP) are multiplex PCR platforms that detect several respiratory viruses from one specimen. For most children hospitalized with acute respiratory illness (ARI), management is supportive, and detection of a specific virus from RPP does not impact clinical care. Therefore, clinical RPP use is not standardized, and ordering is at the discretion of the clinician. We sought to understand factors associated with RPP utilization among pediatric patients hospitalized with ARI. Methods: From October 2017 to September 2021, participants < 18 years hospitalized with ARI were enrolled at a single site in the New Vaccine Surveillance Network (NVSN). Eligible patients were residents of Jackson County, MO, had one or more ARI symptoms (e.g., cough, fever, nasal congestion) lasting < 14 days, and were enrolled within 48 hours of admission. Parent interviews and medical chart reviews were conducted. All participants had a research RPP, but results were not available to the clinical providers. Clinical providers were able to order a clinical RPP (cRPP), for which they received test results. Characteristics of NVSN enrollees hospitalized with ARI with and without a cRPP are described. Lastly, medical complexity was assessed via the pediatric complex chronic conditions classification system (CCC) then analyzed via chi- square test between groups. Findings: During the study period, 1,038 participants were enrolled, and 555 (53.4%) received a cRPP. Most, 299 (53%), cRPPs were ordered in the emergency department or urgent care before admission. Age was a significant factor associated with cRPP use (Table 1). cRPP participants were more likely to have complex chronic conditions, and/or technology dependence. No difference in cRPP use was observed by race/ethnicity, payer status, or sex. More participants were enrolled in 2020-2021, but the overall usage of cRPP is similar between years (Table 2). Conclusions: In this large cohort of children hospitalized with ARI, medical complexity, technological dependence, and age < 2 months were associated with increased utilization of cRPPs. Understanding the impact of cRPP on clinical care requires further investigation to better understand the utility of these tests.
-

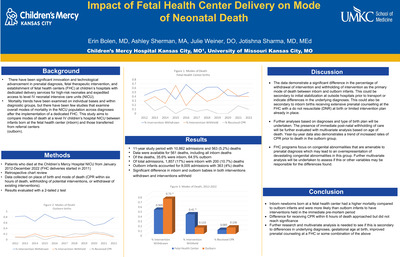
Impact of Fetal Health Center on Mode of Neonatal Death
Erin Bolen, Ashley Sherman, Julie Weiner, and Jotishna Sharma
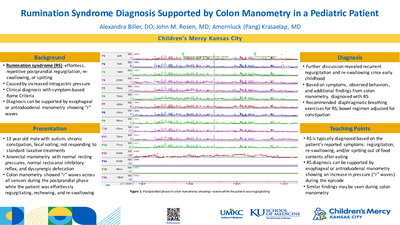
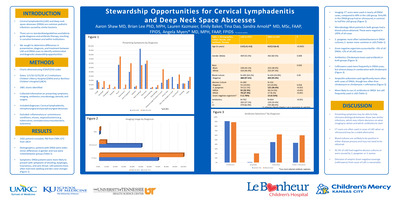
Introduction There has been significant innovation and technological advancement in prenatal diagnosis, fetal therapeutic intervention, and establishment of fetal health centers (FHC) at children’s hospitals with dedicated delivery services for high-risk neonates and expedited access to level IV neonatal intensive care units (NICU). Morality trends have been examined on individual bases and within diagnostic groups, but there have been few studies that examine overall modes of mortality in the NICU population across diagnoses after the implementation of a dedicated FHC. This study aims to compare modes of death at a level IV children’s hospital NICU between infants born at the fetal health center (inborn) and those transferred from referral centers (outborn). Study Design/Methods Patients who died at the Children’s Mercy Hospital NICU from January 2012-December 2022 were identified. FHC deliveries started in 2011. Via retrospective chart review, data were collected on place of birth and mode of death (CPR within six hours of death, withholding of potential interventions, or withdrawal of existing interventions). Results were evaluated with a 2-tailed z test. Further analysis will be undertaken. Results Over the 10-year study period, there were 10,862 admissions and 563 (5.2%) deaths. Of the deaths, 35.6% were inborn and 64.5% outborn. Of total admissions, 1,857 (17%) were inborn with 200 (10.7%) deaths. Outborn infants accounted for 9,005 admissions with 363 (4%) deaths. Data were available for 561 deaths, including all inborn deaths. Figures 1 (inborn) and 2 (outborn) show modes of death by year as a percentage. Modes of death were compared based on place of birth in Figure 3. Differences for withdrawal and withholding of interventions between outborn and inborn infants were significant with p=<0.00001 while the difference for receiving CPR approached but did not reach significance with p=0.073. Discussion The data demonstrate a significant difference in the percentage of withdrawal of intervention and withholding of intervention as the primary mode of death between inborn and outborn infants. This could be secondary to initial stabilization at outside hospitals prior to transport or indicate differences in the underlying diagnoses. This could also be secondary to inborn births receiving extensive prenatal counselling at the FHC with a do not resuscitate (DNR) at birth or limited intervention plan already in place. Further analyses based on diagnoses and type of birth plan will be undertaken. The presence of immediate post-natal withholding of care will be further evaluated with multivariate analysis based on age of death. Year-by-year data also demonstrates a trend of increased rates of CPR prior to death in the outborn group. FHC programs focus on congenital abnormalities that are amenable to prenatal diagnosis which may lead to an overrepresentation of devastating congenital abnormalities in this group. Further multivariate analysis will be undertaken to assess if this or other variables may be responsible for the differences in modes of death between populations. Conclusion Inborn newborns born at a fetal health center had a higher mortality compared to outborn infants and were more likely than outborn infants to have interventions held.
-

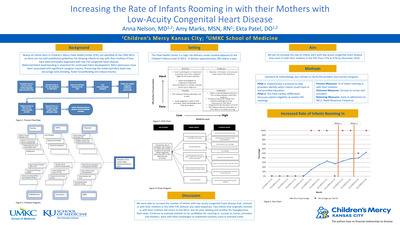
Increasing the Rate of Infants Rooming In with their Mothers with Low Acuity Congenital Heart Disease
Anna Nelson, Amy Marks, and Ekta Patel
Background The Children’s Mercy Fetal Health Center (FHC) was created to be able to deliver infants with complex fetal diagnoses including congenital heart disease. Mothers are referred from all over the Midwest region for their babies to have access to specialized care immediately after birth. Nearly all babies born in the FHC are admitted to our neonatal intensive care unit (NICU), as there are not well-established guidelines for keeping babies with their mothers if they have low-risk congenital heart disease that do not need intensive care continuous monitoring. Maternal infant bonding starts before an infant is born and becomes stronger in those first few moments after birth. Maternal infant bonding is important to help establish breastfeeding if desired and for early childhood development. Previously, only 27% of the patients with these diagnoses that would have been safe to room in with their mothers did. We aim to increase the rate of neonates born with low acuity congenital heart disease that room-in with their mothers in the FHC from 27% to 47% by October 2023. Methods We targeted infants with prenatal diagnoses of likely asymptomatic vascular rings, balanced AV canal, low risk intermittent fetal supraventricular tachycardia, tetralogy of Fallot without concern for pulmonary obstruction or low risk coarctation of the aorta. The first PDSA cycle implemented a protocol that was developed in collaboration with Pediatric Cardiologists to help providers assess the appropriateness of allowing a patient to room in with the mother with intermittent monitoring of vital signs. This protocol also dictates how frequently vital signs should be assessed by nursing once a baby is rooming-in with its mother. Education was provided to the physicians, NNPs and nurses about implementing the protocol. The second PDSA cycle included Fetal Cardiology APRNs discussing the appropriateness of patients rooming in with their mothers at weekly Fetal Health Center meetings. The quantitative data is collected monthly based upon FHC weekly patient e-mails and review of the medical records. Results The rate of infants rooming-in increased to 38% following implementation of the first PDSA cycle and up to 52% following implementation of the second PDSA cycle. Discussion We were able to increase the number of infants with low acuity congenital heart disease that roomed-in with their mothers in the FHC without any rapid responses. The next step is to survey families to better understand their experience of having their infant room-in with them in the FHC.
-

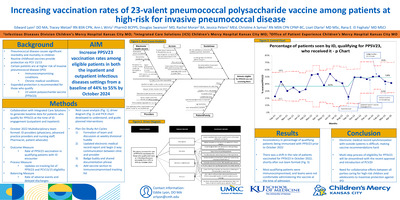
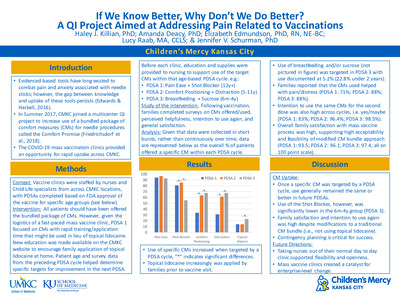
Increasing vaccination rates of 23-valent pneumococcal polysaccharide vaccine among patients at high-risk for invasive pneumococcal disease.
Edward Lyon, Tracey Wetzel, Ann L. Wirtz, Douglas Swanson, Rachel Moran, Jessica Peters, Christine Symes, Liset Olarte, and Rana El Feghaly
Introduction: Pneumococcal disease causes significant morbidity and mortality in children. Routine childhood immunizations protect for 13 or 15 pneumococcal serotypes via two pneumococcal conjugated vaccines. Patients with immunocompromising and chronic medical conditions are at high risk of invasive pneumococcal disease. A 23-valent pneumococcal polysaccharide vaccine (PPSV23) is recommended in these patients to protect against more pneumococcal serotypes, but many patients have not received it. Our AIM is to increase PPSV23 vaccination rates among eligible patients in both the inpatient and outpatient infectious diseases (ID) settings from a baseline of 44% to 55% by October 2024. Methods: In collaboration with Children’s Mercy integrated care solutions, we created a report of eligible patients evaluated by ID in the inpatient and outpatient settings. This report captures pneumococcal immunization history of patients eligible for PPSV23. In October 2022, we formed a multi-disciplinary team of ID nurses, a pharmacist, providers, and a patient advocate. We identified several potential causes of low PPSV23 vaccination rate and developed countermeasures (figure 1). Since October 2022, we have discussed the project weekly during our divisional huddle. In January 2023, we matched outpatient and inpatient reports to include maximal information and created a 2-way communication strategy where outpatient nursing staff notifies ID providers of patients who qualify for PPSV23. In February 2023, we created an EMR shared phrase to include in ID provider notes and a badge buddy with qualifying conditions for PPSV23 vaccination. Results: Following the initiation of the project we have seen an increase in qualifying patients who have received PPSV23 that has so far been sustained for 6 months (48-56%); we also see narrowing of the control limits implying improved process (figure 2). Discussion: We were able to increase PPSV23 vaccination of eligible high-risk patients in both the outpatient and inpatient settings. If this trend is sustained, we will be able to move our center line in 2 months. We have multiple additional plan-do-study-act cycles planned over the next several months to include electronic medical record changes, collaboration with different specialties and family education.
-

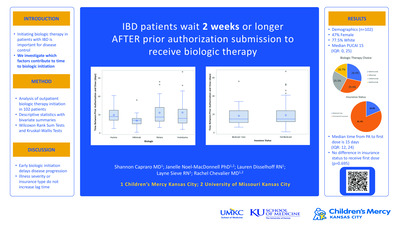
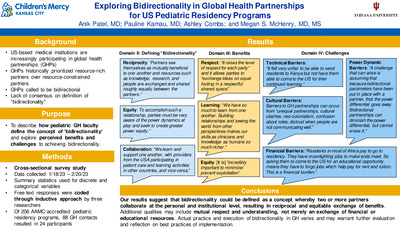
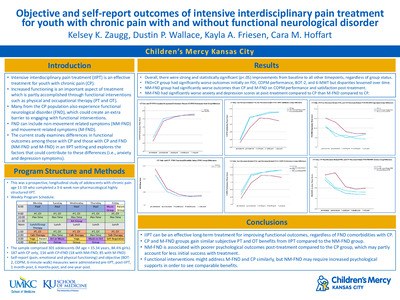
Latency Time From Prior Authorization Submission To Initiation Of Biologic Therapy In Inflammatory Bowel Disease
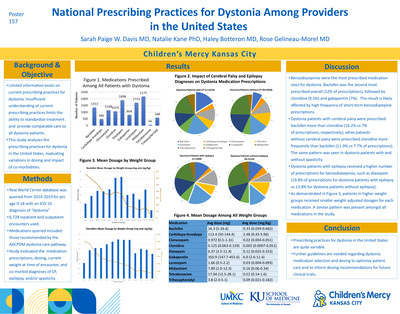
Shannon Capraro, Janelle R. Noel-Macdonnell PhD, Lauren Disselhoff, Layne Sieve, and Rachel Chevalier
Background For pediatric patients with a diagnosis of inflammatory bowel disease (IBD), initiation of biologic therapy can be essential to attain disease control. Unfortunately, patients often experience delays in receiving the first dose of these medications due to the need for insurance companies to approve medication prior authorizations (PA). Physicians and support staff spend many working hours collating and transferring information regarding urgency to payors. To our knowledge, no studies exist to evaluate the factors that contribute to how quickly a medication is approved in pediatric patients. We set out here to evaluate which demographic and disease factors contribute to the lag time between submission of medication prior authorization for IBD biologic therapy and administration of that therapy. Methods Our pilot cohort consists of 102 patients with IBD who initiated biologics as an outpatient at our tertiary care hospital between the years of 2018-2023. Clinical information regarding disease status, previous therapies, surgical history, laboratory information, and medication administration information was obtained from the chart. Descriptive statistics were performed and followed by bivariate summaries for insurance status (Medicaid users vs. not), initial denial of biologic, and type of biologic. Wilcoxon Rank Sum Tests and Kruskal-Wallis Test were used to compare time from PA to first dose depending on variable of interest. Results Demographics are included in Table 1. Patients were median age of 14.7 years (interquartile range [IQR] 11.5-17.0) and were 52.9% male. Most patients (80/102; 78.4%) have Crohn’s disease. In this cohort, the median time from submission of prior authorization to administration of medication (lag time) was 15.0 days (IQR 12.0-24.0) with maximum times up to 53 days. When evaluating between medications, infliximab had a significantly lower median lag time (median 14d; IQR 10-16d) compared to ustekinumab (17.5d; IQR 13-28) or adalimumab (18d; IQR 14-25d) but not vedolizumadb (16d; IQR 11-26) (Figure 1). No other pairings showed a significant difference. Pediatric Ulcerative Colitis Activity Index (PUCAI) decreased the lag time 1.5 days for every 10-point increase in PUCAI. Hemoglobin, albumin, ESR, and CRP contributions to lag time varied between medications. Lag time does not vary significantly between state insurance (Medicaid) and private insurance (Figure 2). Additionally, an initial denial of the prior authorization requiring appeal does not prolong lag time. Conclusion Early initiation of biologic therapy can delay the progression of disease to stricturing or penetrating disease 2 . However, providers experience significant challenges administering these medications in a timely manner. Notably, pediatric patients with IBD often wait at least two weeks to receive their first dose of biologic therapy. Our preliminary analysis does not indicate that severity of illness or type of insurance make clinically significant differences. It is important to remark that our population was limited in the number of Medicaid patients, so more data will be essential to corroborate this analysis. Infliximab shows the quickest availability perhaps due to its long history on the market, availability of biosimilars, or widespread use. Further analysis of our collected cohort of approximately 400 patients is pending including analysis of outcomes.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}