
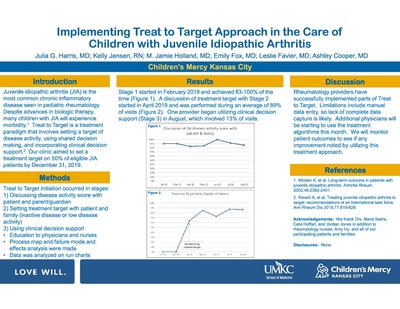
-

An Innovation for Skin Integrity Risk Assessment SIRA Quality Metrics
Kristina Foster, Michele Fix, and Lacey Bergerhofer
Metrics for hospital acquired pressure ulcers over time, by stage, by device, and compared to other pediatric hospitals.
-

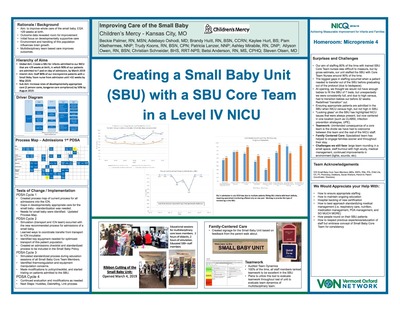
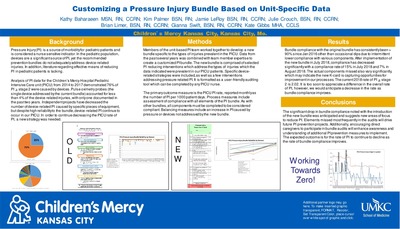
Customizing a Pressure Injury Bundle Based on Unit-Specific Data
Kathlyn Baharaeen, Kimberly Palmer, Jamie Leroy, Julia Crouch, Bryan Limer, Gianna Swift, and Kate Gibbs
-

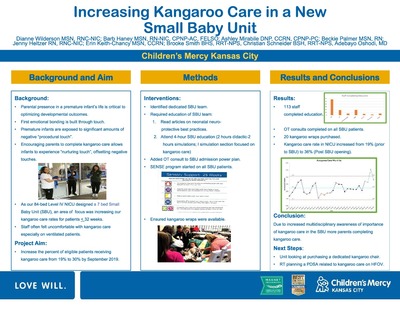
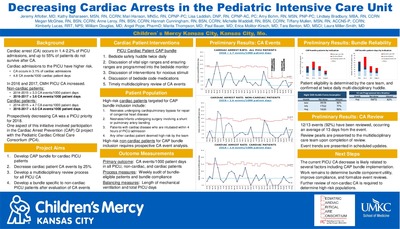
Decreasing Cardiac Arrests in the Pediatric Intensive Care Unit
Jeremy Affolter, Kathlyn Baharaeen, Mari Hanson, Lisa Laddish, Amy Bohm, Lindsey Bradbury, Megan McGhee, Anne Leroy, Hannah Cunningham, Michelle Waddell, Tiffany Mullen, Kimberly Lucas, William Douglas, Angel Pope, Marita Thompson, Paul N. Bauer, Erica Molitor-Kirsch, Tara Benton, and Laura Miller-Smith
-

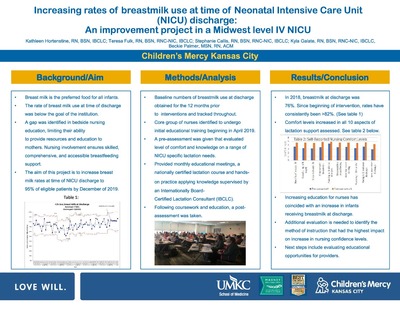
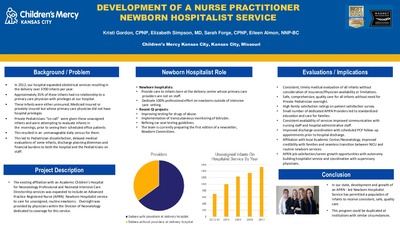
Development of a Nurse Practitioner Newborn Hospitalist Service
Kristi Gordon, Elizabeth Simpson, Sarah Forge, and Eileen Almon
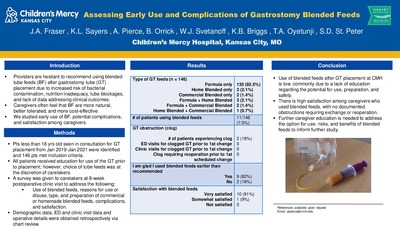
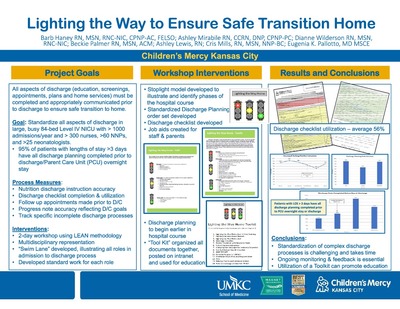
Background/Problem
•In 2012, our hospital expanded obstetrical services resulting in the delivery over 3700 infants per year.
•Approximately 35% of these infants had no relationship to a primary care physician with privileges at our hospital.
•These infants were either uninsured, Medicaid insured or privately insured but whose primary care physician did not have hospital privileges.
•Private Pediatricians “on call” were given these unassigned infants and were attempting to evaluate infants in the mornings, prior to seeing their scheduled office patients
•This resulted in an unmanageable daily census for them.
•This led to Pediatrician dissatisfaction, delayed medical evaluations of some infants, discharge planning dilemmas and financial burdens to both the hospital and the Pediatricians on staff.Project Description
•The existing affiliation with an Academic Children’s Hospital for Neonatology Professional and Neonatal Intensive Care Directorship services was expanded to include an Advanced Practice Registered Nurse (APRN) Newborn Hospitalist service to care for unassigned, routine newborns. Oversight was provided by physicians within the Division of Neonatology dedicated to coverage for this service.
Newborn Hospitalist Role
•Newborn hospitalists:
•Provide care to infants born at the delivery center whose primary care providers are not on staff.
•Dedicate 100% professional effort on newborns outside of intensive care setting. •Recent QI projects:
•Improving testing for drugs of abuse.
•Implementation of transcutaneous monitoring of bilirubin.
•Refining car seat testing guidelines.
•The team is currently preparing the first edition of a newsletter, Newborn Connections.Evaluations/Implications
•Consistent, timely medical evaluation of all infants without consideration of insurance/Physician availability or limitations.
•Safe, comprehensive, quality care for all infants without need for Private Pediatrician oversight.
•High family satisfaction ratings on patient satisfaction survey. •Small number of dedicated APRN Providers led to standardized education and care for families. •Consistent availability of services improved communication with nursing staff and hospital administrative staff.
•Improved discharge coordination with scheduled PCP follow-up appointments prior to hospital discharge.
•Affiliation with local Academic Center/Neonatology, improved credibility with families and seamless transition between NICU and routine newborn services. •APRN job satisfaction/career growth opportunities with autonomy building hospitalist service and coordination with supervisory physiciansConclusion
•In our state, development and growth of an APRN -led Newborn Hospitalist Service has permitted a population of infants to receive consistent, safe, quality care.
•This program could be duplicated at institutions with similar circumstances -

Early Identification of Depression in Patients with Pediatric Epilepsy
Erin Fecske, Paul Glasier, Lines Vargas Collado, and Elizabeth Rende
Describes the use of the Neurological Disorders Depression Inventory-Epilepsy-Youth (NDDI-E-Y) in adolescent patients in a comprehensive epilepsy center to identify patients who need referral for mental health care.
-

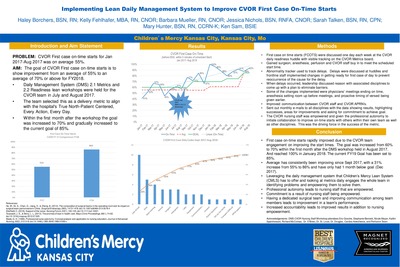
Implementing Lean Daily Management System to Improve CVOR First Case On-Time Starts
Haley Borchers, Kelly Fehlhafer, Barbara Mueller, Jessica Nichols, Sarah Talken, Mary Hunter, and Kenneth Sam
-

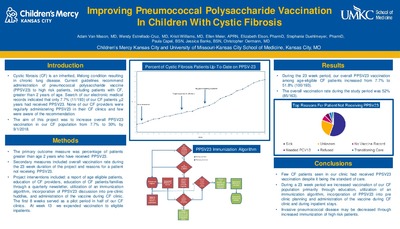
Improving Pneumococcal Polysaccharide Vaccination in Children With Cystic Fibrosis
Adam Van Mason, Wendy Estrellado-Cruz, Kristi Williams, Ellen Meier, Elizabeth Elson, Stephanie Duehlmeyer, Paula Capel, Jessica Banks, and Christopher M. Oermann
-

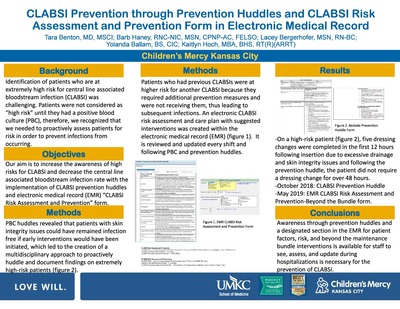
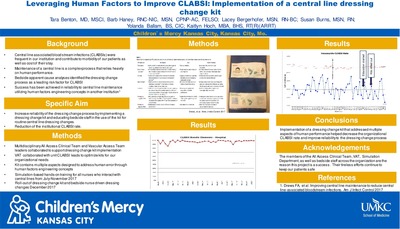
Leveraging Human Factors to Improve CLABSI: Implementation of a Central Line Dressing Change Kit
Tara Benton, Barb Haney, Lacey Bergerhofer, Susan Burns, Yolanda Ballam, and Kaitlyn Hoch
-

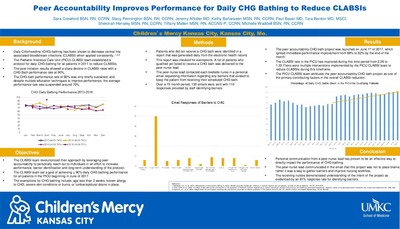
Peer Accountability Improves Performance for Daily CHG Bathing to Reduce CLABSIs
Sara Crawford, Stacy Pennington, Jeremy Affolter, Kathlyn Baharaeen, Paul N. Bauer, Tara Benton, Shekinah Hensley, Tiffany Mullen, and Michelle Waddell
-

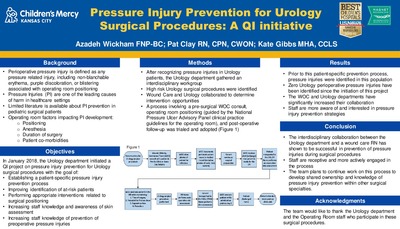
Pressure Injury Prevention for Urology Surgical Procedures: A QI Initiative
Azadeh Wickham, Pat Clay, and Kate Gibbs
-

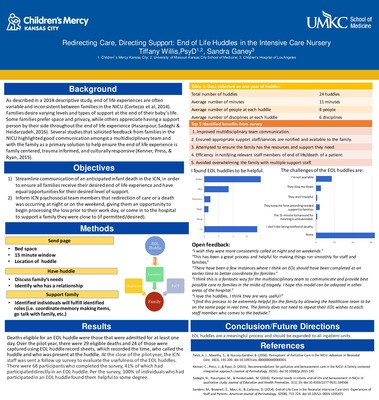
Redirecting Care, Directing Support: End of Life Huddles in the Intensive Care Nursery
Tiffany Willis and Sandra Ganey
-

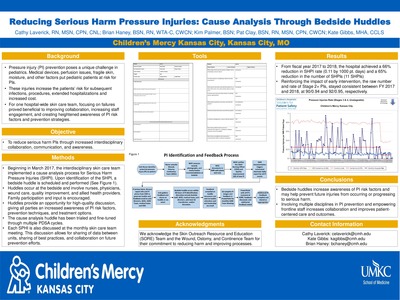
Reducing Serious Harm Pressure Injuries: Cause Analysis Through Bedside Huddles
Cathy Bandelier Laverick, Brian Haney, Kimberly Palmer, Pat Clay, and Kate Gibbs
-

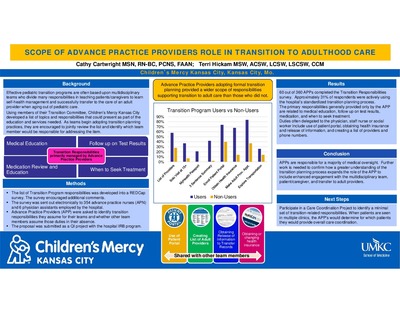
Scope of Advance Practice Providers' Role in Transition to Adulthood Care
Cathy Cartwright and Teresa Hickam
Advance Practice Providers adopting formal transition planning provided a wider scope of responsibilities supporting transition to adult care than those who did not.
-

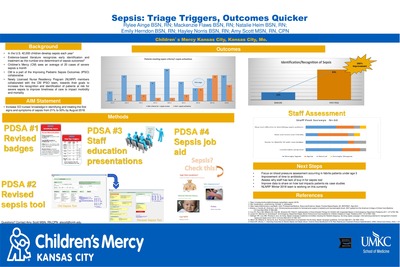
Sepsis: Triage Triggers, Outcomes Quicker
Rylee Ainge, Mackenzie Flaws, Natalie Heim, Emily Herndon, Hayley Norris, and Amy Scott
-

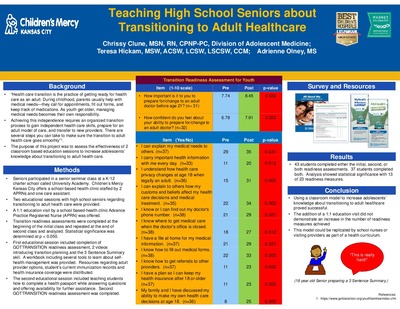
Teaching High School Seniors about Transitioning to Adult Healthcare
Christine Clune, Teresa Hickam, and Adrienne Olney
This poster describes an educational intervention consisting of two classroom sessions to teach high school seniors how to successfully transition to adult care. Topics covered included the ability to fill out medical forms, when to contact one's doctor and where to get medical care when the doctor's office is closed, how health care privacy changes at age 18, the need for health insurance, the need to keep medical records, etc.
-

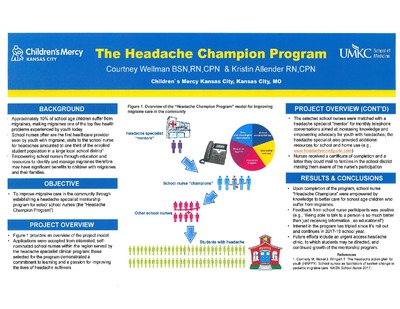
The Headache Champion Program
Courtney Wellman and Kristin Allender
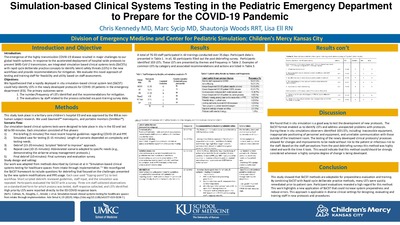
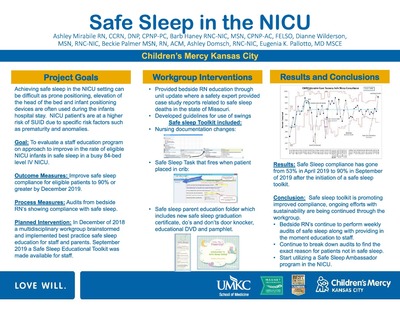
BACKGROUND
Approximately 10% of school age children suffer from migraines, making migraines one of the top five health problems experienced by youth today
School nurses often are the first healthcare provider seen by youth with migraine; visits to the school nurse for headaches amounted to one-third of the enrolled student population in a large local school district. (see reference)
Empowering school nurses through education and resources to identify and manage migraines therefore may have significant benefits to children with migraines and their families.
OBJECTIVE
To improve migraine care in the community through establishing a headache specialist mentorship program for select school nurses (the "Headache Champion Program")
PROJECT OVERVIEW
Figure 1 provides an overview of the project model
Applications were accepted from interested, self-nominated school nurses within the region served by the headache specialist clinical program; those selected for the program demonstrated a commitment to learning and a passion for improving the lives of headache sufferers
The selected school nurses were matched with a headache specialist "mentor" for monthly telephone conversations aimed at increasing knowledge and empowering advocacy for youth with headaches; the headache specialist also provided additional resources for school and home use (e.g., www.headachereliefguide.com)
Nurses received a certificate of completion and a letter they could mail to families in the school district making them aware of the nurse's participation
RESULTS & CONCLUSIONS
Upon completion of the program, school nurse "Headache Champions" were empowered by knowledge to better care for school age children who suffer from migraines.
Feedback from school nurse participants was positive (e.g., "Being able to talk to a person is so much better than just receiving information. . . so educational")
Interest in the program has triipled since its roll out and continues in 2017-18 school year
Future efforts include an urgent access headache clinic, to which students may be directed, and continued growth of the mentorship program.
-

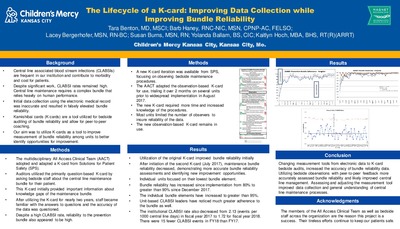
The Lifecycle of a K-card: Improving Data Collection While Improving Bundle Reliability
Tara Benton, Barb Haney, Lacey Bergerhofer, Susan Burns, Yolanda Ballam, and Kaitlyn Hoch
-

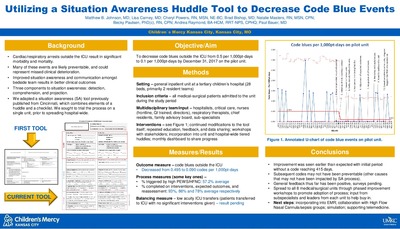
Utilizing a Situation Awareness Huddle Tool to Decrease Code Blue Events
Matthew B. Johnson, Lisa Carney, Cheryl Powers, Bradley Bishop, Natalie Masters, Becky Paulsen, Andrea Raymond, and Paul N. Bauer
-

An Expanded Role for Nurses in Laboratory Utilization
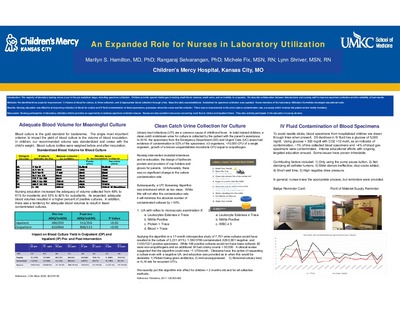
Marilyn S. Hamilton, Rangaraj Selvarangan, Michele Fix, and Lynn E. Shriver
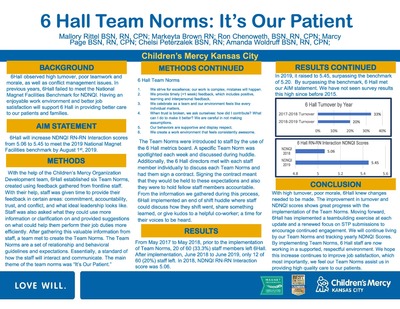
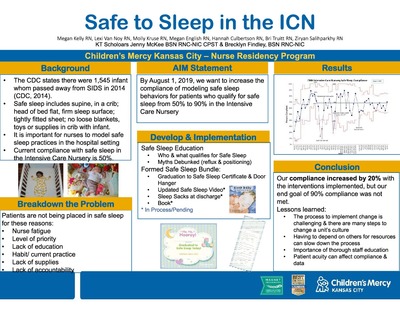
Introduction: The majority of laboratory testing errors occur in the pre-analytical stage, including specimen collection. Children provide special challenges including small blood volumes, small veins, and an inability to cooperate. We describe collaboration between laboratorians and nursing staff to improve specimen collection and the reliability of test results.
Methods: We identified three areas for improvement: 1) Volume of blood for culture, 2) Urine collection, and 3) Appropriate blood collection through a line. Base line data was established. Guidelines for specimen collection were updated. Nurse members of the Laboratory Utilization Committee developed educational tools.
Results: Nursing education was effective at improving collection of blood for culture and IV fluid contamination of blood specimens, processes where the nurse was the collector. There was no improvement in the urine culture contamination rate, a process which involves the patient and/or family members.
Discussion: Nursing participation in laboratory utilization efforts provides an opportunity to address specimen collection issues. Nurses are also excellent resources concerning work flow in clinics and inpatient floors. They also actively participate in the education of young doctors.
-

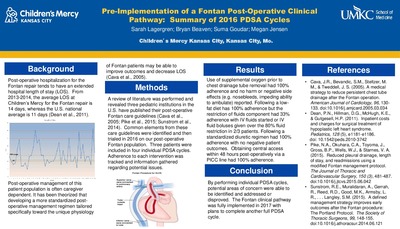
Pre-Implementation of a Fontan Post-Operative Clinical Pathway: Summary of 2016 PDSA Cycles
Sarah M. Lagergren, Bryan Beaven, Suma Goudar, and Megan Jensen
Background/Introduction: Post-operative hospitalization for the Fontan procedure tends to have an extended hospital length of stay (LOS). From 2013-2014, the average LOS at Children’s Mercy for the Fontan procedure is 14 days, whereas the U.S. national reported average is 11 days. Post-operative management of this patient population is often caregiver dependent. It has been theorized that developing a more standardized post-operative management regimen tailored specifically toward the unique physiology of Fontan patients may be able to improve outcomes and decrease LOS.
Methods: A review of literature was performed and revealed three pediatric institutions have published their post-operative Fontan care guidelines. Common elements from these care guidelines were identified and then trialed in 2016 on our post-operative Fontan population. Three patients were included in four individual PDSA cycles. Adherence to each intervention was tracked and information gathered regarding potential issues.
Results: Use of supplemental oxygen prior to chest drainage tube removal had 100% adherence and no harm or negative side effects (such as nosebleeds, or impeding ability to ambulate) reported. Restriction of fluids had a 33% adherence rate with IV fluids started or IV fluid boluses administered over the 80% restriction in 2/3 patients. Following a standardized diuretic regimen had 100% adherence with no negative patient outcomes. Obtaining central access within 48 hours post-operatively via a PICC line had 100% adherence.
Conclusion: By performing individual PDSA cycles prior to full implementation of a post-operative clinical pathway, potential areas of concern were able to be identified and addressed or disproved. The Fontan clinical pathway was fully implemented for 2017 with plans to complete another full PDSA cycle.
-
 Performed in Tandem with CRRT and/or ECMO: Experience of One Pediatric Center by Lejla Music Aplenc, Cindy George, and Kimberly Marriott")
Therapeutic Plasma Exchange (TPE) Performed in Tandem with CRRT and/or ECMO: Experience of One Pediatric Center
Lejla Music Aplenc, Cindy George, and Kimberly Marriott
SUMMARY
The most common indications for starting tandem procedures were ASFA Category III indications, followed by un-categorized indications.
Similar to other reports in literature, hypocalcemia and hypotension were the most common complications. Transfusion reactions were rare, despite the use of large volumes of plasma.
Tandem procedures in critically ill pediatric patients require close monitoring and excellent communication between staff members.
-

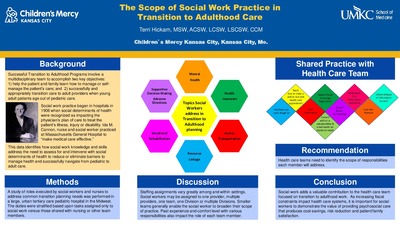
The Scope of Social Work Practice in Transition to Adulthood Care
Teresa Hickam
This is a study of roles executed by social workers and nurses to address common transition planning needs in a pediatric hospital. Duties were stratified based upon tasks assigned only to social work versus those shared with nursing or other team members.
-

Use of Personalized Patient Heart Diagrams at the Bedside to Improve Quality of Care
Melissa D. Elliott
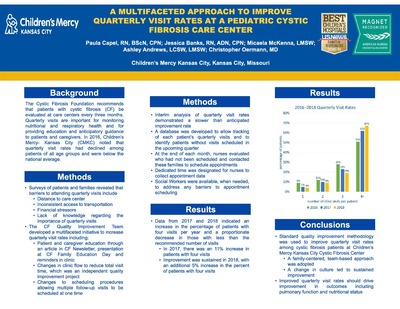
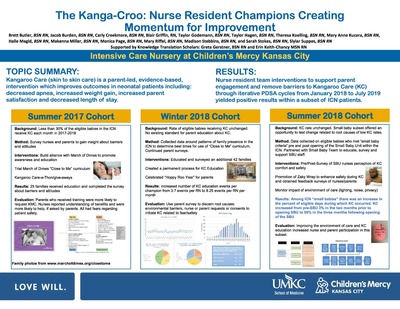
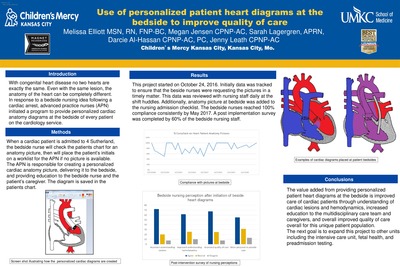
Title: Use of personalized patient heart diagrams at the bedside to improve quality of care
Background/Introduction: With congenital heart disease no two hearts are exactly the same. Even with the same lesion, the anatomy of the heart can be completely different. In response to a bedside nursing idea following a cardiac arrest, advanced practice nurses (APN) initiated a program to provide personalized cardiac anatomy diagrams at the bedside of every patient on the cardiology service.
Methods: When a cardiac patient is admitted to cardiology floor, the nurse will check the patients chart for an anatomy picture, then will place the patient’s initials on a worklist for the APN if no picture is available. The APN is responsible for creating a personalized cardiac anatomy picture, delivering it to the bedside, and providing education to the nurse and the patient’s caregiver. The diagram is saved in the patients chart.
Results: This project started on October 24, 2016. Initially data was tracked to ensure that nurses were requesting the pictures in a timely matter. This data was reviewed with nursing staff daily at the shift huddles. Additionally, anatomy picture at bedside was added to the nursing admission checklist. The team reached 100% compliance consistently by May 2017. A post implementation survey was completed by 60% of the nursing staff.
Conclusion: The value added from providing personalized patient heart diagrams at the bedside is improved care of cardiac patients through understanding of cardiac lesions and hemodynamics, increased education to the multidisciplinary care team and caregivers, and overall improved quality of care overall for this unique patient population.
The next goal is to expand this project to other units including the intensive care unit, fetal health, and preadmission testing.
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}