
-

Save the Pharmacy Piggy Bank: Managing Mega High-Cost Drugs
Richard K. Ogden Jr., Jerame Hill, and Sam Abdelghany
-

A NINJA Initiative at Children's Mercy
Richard Ogden, Bradley A. Warady, Vimal Chadha, and Wendy Hoebing
-

Facilitating the everyday steward: Impact of mandatory antimicrobial indication/duration and a 48 hour time out
Ann L. Wirtz, Alaina N. Burns, Brian R. Lee, Tammy Frank, Laura Fitzmaurice, Richard Ogden, Brian O'Neal, and Jennifer Goldman
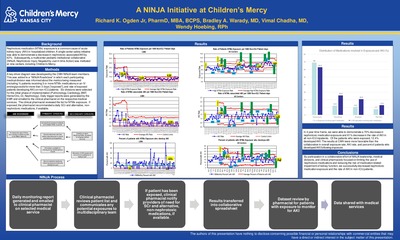
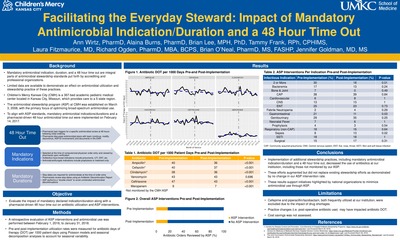
Introduction: Required indication, duration, and a 48-hour antimicrobial timeout are an integral part of antimicrobial stewardship standards; however, limited data are available to demonstrate an effect on antimicrobial utilization and antimicrobial stewardship practice. Therefore, we evaluated the impact of mandatory declared indication/duration along with a pharmacy-driven 48-hour timeout on antimicrobial utilization and antimicrobial stewardship interventions.
Methods: We performed a retrospective evaluation of ASP interventions and antimicrobial use following implementation of mandatory antimicrobial indication/duration at the point of computerized physician order entry (CPOE). A pharmacist-driven 48-hour antimicrobial timeout was introduced on the same date. This study was conducted at Children’s Mercy Kansas City, a 367-bed freestanding pediatric hospital servicing the Kansas City Metro Area and beyond. Data were collected from February 1, 2016 to January 31, 2018. A pre and post comparison was performed; interventions were implemented hospital-wide on February 14, 2017. ASP intervention rates were measured. Days of therapy (DOT) per 1000 patient days of antibiotics were also evaluated. Poisson models were utilized to compare DOT rates pre- and post-implementation, and seasonal decomposition analyses were performed to account for seasonal variability.
Results: A significant decrease in DOT rates was observed in non-ASP monitored antibiotics post-implementation, including cefazolin (39.7 to 36.9; p
Conclusions: Implementation of additional stewardship practices, including mandatory antimicrobial indication/ duration and a pharmacist-driven 48-hour timeout, resulted in a decrease in the use of antimicrobials, including those not monitored by our ASP. These efforts augmented, but did not replace existing stewardship efforts. These results support initiatives highlighted by national organizations to minimize unnecessary antimicrobial use through ASP.
-

Integration of a Pharmacist in a Pediatric Medical Home for Children with Medical Complexity
Alannah K. Yoder, Richard K. Ogden Jr., Ingrid A. Larson, and Emily J. Goodwin
Background/Objectives
Children with medical complexity require unique care, specialized attention, and a dedicated team to meet the needs of the patient & caregivers. Drug-therapy related problems in complex, chronic conditions influence financial, institutional, and patient outcomes. The addition of a pharmacist allows for collaboration and delivery of comprehensive medication management in order to provide value-added medication services to optimize complex therapeutic regimens and patient outcomes through evidence-based practice, medication adherence, medication use coordination, and medication safety processes.
Description
Our program provides a pediatric medical home for hundreds of children with medical complexity. Families are cared for by a comprehensive medical team, including a clinical pharmacist. The pharmacist is available for all appointments and meets with patients and caregivers at the beginning of clinic visits. The pharmacist’s initiative to improve patient care is provided through multiple services which include: (1) comprehensive medication reconciliation through history provided by caregiver, outpatient pharmacy review, and chart review of specialty teams; (2) adverse drug assessment; (3) systemic drug-utilization review of each medication (drug-disease contraindication, drug-drug interaction, drug-patient precaution, dosing, duration of drug treatment, over and/or underutilization, drug dosage for modification, adherence concerns, and determination if additional monitoring is warranted); (4) patient education and development of personal, family-friendly medication lists; and (5) coordination of care between inpatient admissions, specialty/consulting services, home healthcare, and prior authorization needs.
Significance
The integration of a pharmacist in a pediatric medical home for children with medical complexity and childhood-onset disabilities allows for innovation and interdisciplinary collaboration to provide comprehensive medication management. Incorporation of family education and tangible medication plans promotes safe and consistent medication practices. Further studies describing the qualitative and quantitative impact on patient outcomes will be conducted at our institution.
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.



{kind=link}
{kind=link}
{kind=link}
{kind=link}