
Publication Date
5-2021
Files
Download Full Text (500 KB)
Abstract
Background: A study using administrative data reported urgent care providers as having the highest rates of inappropriate antibiotic use for upper respiratory illnesses. In a national survey, pediatric urgent care providers reported family expectations as a primary driver for prescribing inappropriate antibiotics. Standardized scripting has been effective at reducing unnecessary antibiotics while increasing family satisfaction.
Objective: To reduce inappropriate prescribing for upper respiratory infections (acute otitis media (AOM), otitis media with effusion (OME), and pharyngitis) in pediatric urgent cares by 20% by December 1, 2020 through use of standardized scripting in Year 2 of a national pediatric urgent care quality improvement collaborative.
Design/Methods: Participants were recruited via email, newsletters, and webinars from pediatric urgent care national societies. Each site committed at least 3 providers who each submitted data from 10 encounters per month. Antibiotic prescribing was defined as appropriate based on consensus guidelines. Previously published antibiotic stewardship scripting for viral upper respiratory infections was adapted for use with the three target diagnoses. Patient and family advisors reviewed all scripting and their feedback was incorporated into the revised standardized scripting. Clinical examples for each diagnosis using the standardized scripting were provided to the collaborative by use of digital cartoon videos, written framework, and templated discharge instructions. Data from clinical encounters were submitted via a REDCap form, analyzed for inappropriateness, and reported back to participating sites via run charts during monthly webinars.
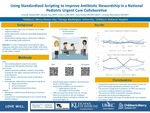
Results: The 104 participants from 10 institutions submitted 1,150 encounters for analysis in the intervention cycles (May-December 2020). Overall inappropriate antibiotics decreased from 26.4% to 16.6% (p=0.13). Inappropriate antibiotic use decreased in AOM (38.6% to 26.5%; p=0.12) and pharyngitis (14.5% to 8.8%; p=0.26). OME increased from 30.8% to 46.7% (p=0.18) (Figure 1). During the study immediate antibiotic prescriptions for OME decreased; however, delayed prescribing increased (Figure 2).
Conclusion(s): In its second year, this national collaborative developed standardized scripting to overcome the barrier of perceived family expectations to decreases inappropriate antibiotic prescriptions in pediatric urgent care for AOM and pharyngitis. Future interventions will target the inappropriate use of delayed prescribing in OME.
Presented at the 2021 PAS Virtual Conference
Disciplines
Emergency Medicine | Pediatrics
Recommended Citation
Nedved, Amanda; Fung, Melody; Liu, Cindy; Hamdy, Rana; and Montalbano, Amanda, "Using Standardized Scripting to Improve Antibiotic Stewardship in a National Pediatric Urgent Care Collaborative" (2021). Posters. 166.
https://scholarlyexchange.childrensmercy.org/posters/166


