
These posters have been presented at meetings in Children's Mercy and around the world. They represent research that was done at the time they were created, and may not represent medical knowledge or practice as it exists at the time viewers access these posters.
-

BYOS: Build Your Own Simulator - Creation of Specialized Surgical Simulations Using AI Segmentation and 3D Printing
Jieun Lee MD
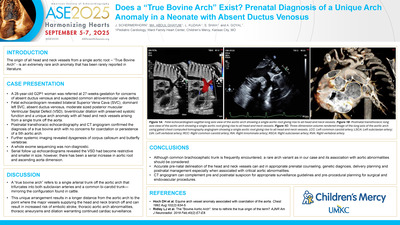
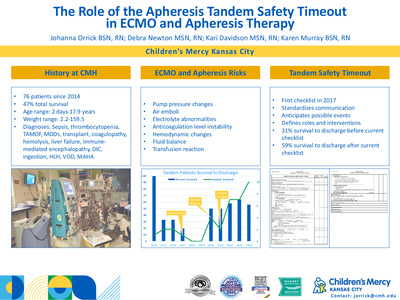
Aim: Minimally invasive surgery in children frequently involves performing complex tasks within a confined space. Skills obtained in general surgery training are not always transferable to specialized technical aspects of pediatric procedures. We describe an expedited workflow for designing and creating tailored simulations for pediatric procedures.. Methods: An anonymized infant thoracoabdominal CT scan was imported into 3D Slicer (Slicer.org). An AI segmentation algorithm was then applied to the images (TotalSegmentator) for rapid modeling of anatomic structures. After post-processing, relevant models were exported as .STL files and uploaded into slicer software for further modification and printing using fused deposition modeling (FDM) or stereolithography (SLA). Materials were selected based on the desired properties of the simulated tissue. For structures not printable with thermoplastics or resin, (skin and subcutaneous tissue), the models were used to generate negative silicone molds. Incorporation of mechanical elements (magnets, hinges) was done using Autodesk Fusion 360. Results: AI modeling of all structures was performed in approximately 67 seconds. Printing time for individual components was approximately 8-16 hours depending on materials used. A non-linear cut was placed through the thoracic model to allow for fixation of simulated or animal tissue between magnetic and mechanical attachment points. Conclusions: Conversion of CT and MRI data to printable 3D models can be accomplished rapidly using AI segmentation algorithms integrated into open-source imaging software. Low-cost commercial 3D printers are now able to manufacture detailed objects using diverse materials. This enables pediatric surgeons to create simulators tailored to complex procedural tasks.
-

Dental Findings Associated with Dandy Walker and Orofacial Digital Syndrome
Cailey C. Schell, Robin Onikul, Neena Patel, Jenna Sparks, and Amy Burleson
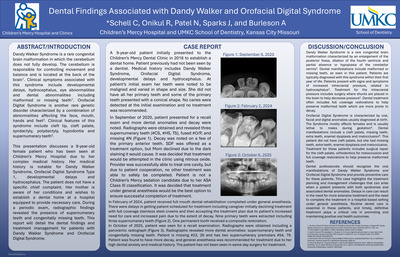
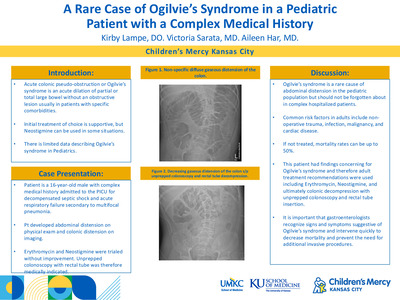
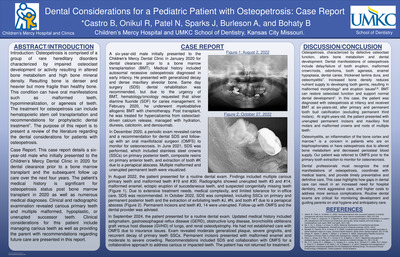
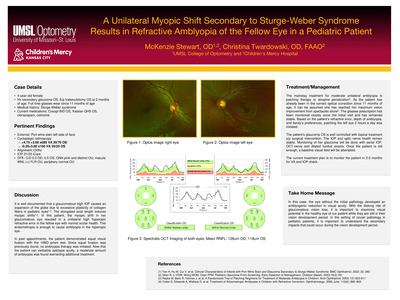
Dandy Walker Syndrome is a rare congenital brain malformation in which the cerebellum does not fully develop. The cerebellum is responsible for controlling movement and balance and is located at the back of the brain1. Clinical symptoms associated with this syndrome include developmental delays, hydrocephalus, eye abnormalities and dental abnormalities including malformed or missing teeth1. Orofacial Digital Syndrome is another rare genetic disorder characterized by a combination of abnormalities affecting the face, mouth, hands and feet2. Clinical features of this syndrome include cleft lip, cleft palate, syndactyly, polydactyly, hypodontia and supernumerary teeth2. This presentation discusses a 9-year-old female patient who has been seen at Children’s Mercy Hospital due to her complex medical history. Her medical history is notable for Dandy Walker Syndrome, Orofacial Digital Syndrome Type 1, developmental delays and hydrocephalus. The patient does not have a specific chief complaint. Her mother is aware of her conditions and wishes to establish a dental home at a hospital equipped to provide necessary care. During a periodic exam, radiographic findings revealed the presence of supernumerary teeth and congenitally missing teeth. This report will detail the dental findings and treatment management for patients with Dandy Walker Syndrome and Orofacial Digital Syndrome.
-

Dental Rehabilitation of Pediatric Patient with Ellis-van Creveld Syndrome: Case Report
Emma Kojima DDS, Robin Onikul, Neena Patel, Jenna Sparks, and Amy Burleson
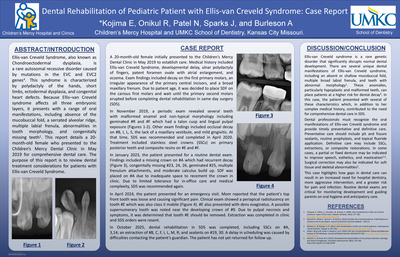
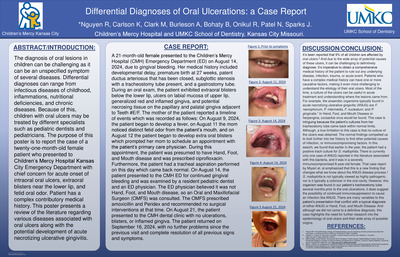
Ellis-van Creveld Syndrome, also known as Chondroectodermal dysplasia, is a rare autosomal recessive disorder caused by mutations in the EVC and EVC2 genes4. This syndrome is characterized by polydactyly of the hands, short limbs, ectodermal dysplasia, and congenital heart defects. Because Ellis–van Creveld syndrome affects all three embryonic layers, it presents with a range of oral manifestations, including absence of the mucobuccal fold, a serrated alveolar ridge, multiple labial frenula, abnormalities in tooth morphology, and congenitally missing teeth1. This report details a 20-month-old female who presented to the Children’s Mercy Dental Clinic in May 2019 for comprehensive dental care. The purpose of this report is to review dental treatment considerations for patients with Ellis-van Creveld Syndrome.
-

Dental Rehabilitation with General Anesthesia and Analysis of Waiting Time Periods
Hannah Shelton, Bethany Castro, Neena Patel, Robin Onikul, Amy Burleson, and Jenna Sparks
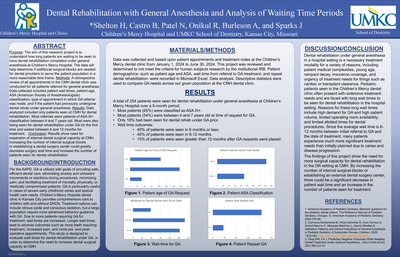
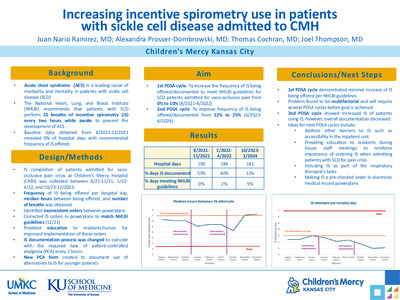
Purpose: The aim of this research project is to understand how long patients are waiting to be seen to have dental rehabilitation completed under general anesthesia at Children’s Mercy Hospital. The data will help determine if additional surgical blocks are needed for dental providers to serve the patient population in a more reasonable time frame. Methods: A retrospective review of all appointments in the CMH dental clinic was conducted for all patients referred for general anesthesia. Data collected included patient wait times, patient age, ASA (American Society of Anesthesiologists) classification, type of appointment in which GA referral was made, and if the patient had previously undergone dental rehab under general anesthesia. Results: Data analyzed included only patients seen at CMH for dental rehabilitation. Most referrals were patients of ASA III+ classification between 4 and 7 years old. Most were also being seen for dental rehabilitation under GA for the first time and waited between 6 and 12 months for treatment. Conclusion: Results show need for expansion of internal dental surgical capacity at CMH. Increasing the number of internal surgical blocks or establishing a dental surgery center could greatly decrease surgery wait time and increase the number of patients seen for dental rehabilitation.
-

Evaluation and Treatment of Pediatric Pre-eruptive Intracoronal Resorption
Sophia Rosen, Robin Onikul, Neena Patel, Jenna Sparks, and Amy Burleson
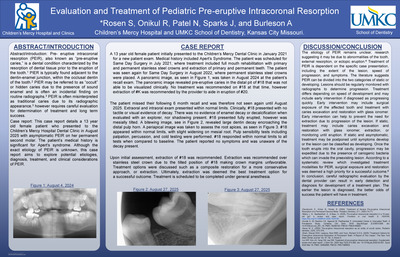
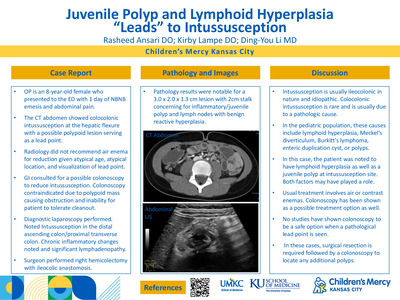
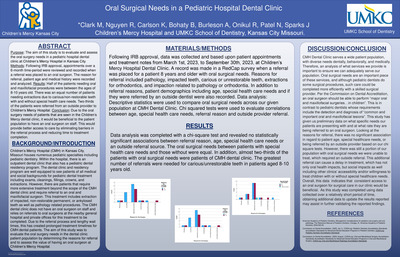
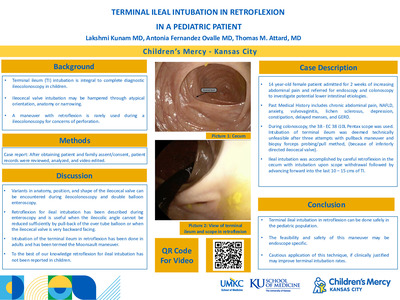
Pre- eruptive intracoronal resorption (PEIR), also known as “pre-eruptive caries,” is a dental condition characterized by the resorption of dental tissue prior to the eruption of the tooth.1PIER is typically found adjacent to the dentin-enamel junction, within the occlusal dentin of the tooth.2PIER may be referred to as “occult” or hidden caries due to the presence of sound enamel and is often an incidental finding on routine radiographs.3PEIR is often misinterpreted as traditional caries due to its radiographic appearance,3however requires careful evaluation for determination of treatment and long term success. Case report: This case report details a 13 year old female patient who presented to the Children’s Mercy Hospital Dental Clinic in August 2025 with asymptomatic PEIR on her permanent second molar. The patient’s medical history is significant for Apert’s syndrome. Although the exact etiology of PEIR is unknown, this case report aims to explore potential etiologies, diagnosis, treatment, and clinical considerations of PEIR
-
 by Caitlyn Maye, Robert C. Gibler, Kristen E. Jastrowski, Dustin Wallace PhD, Cara M. Hoffart, and Jenny Scheurich PhD")
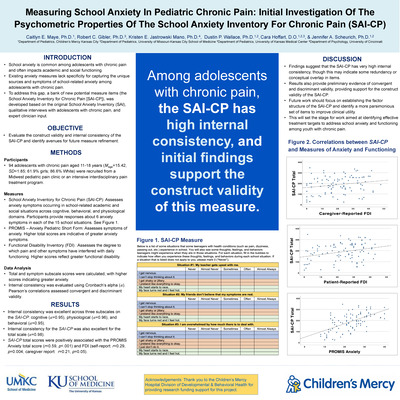
Measuring school anxiety in pediatric chronic pain: Initial investigation of the psychometric properties of the School Anxiety Inventory for Chronic Pain (SAI-CP)
Caitlyn Maye, Robert C. Gibler, Kristen E. Jastrowski, Dustin Wallace PhD, Cara M. Hoffart, and Jenny Scheurich PhD
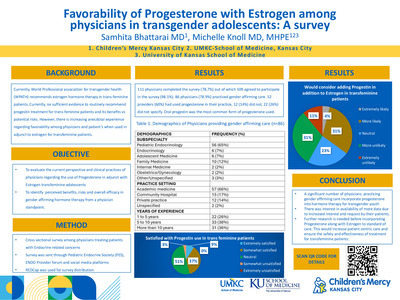
Introduction: School anxiety is common among adolescents with chronic pain and often impacts academic and social functioning. Existing anxiety measures lack specificity for capturing the unique sources and symptoms of school-related anxiety in this population. To address this gap, a bank of new potential measure items (the School Anxiety Inventory for Chronic Pain [SAI-CP]), was developed based on the original School Anxiety Inventory (SAI), qualitative interviews with adolescents with chronic pain, and expert clinician input. The objective of this study was to evaluate the construct validity and internal consistency of the SAI-CP and identify avenues for future measure refinement. Method: Participants were 97 adolescents aged 11-18 (87% White, 62% female, 13.3% minoritized gender identity) seeking treatment in a Midwest pediatric pain clinic or an intensive interdisciplinary pain treatment program. Adolescents completed demographics, PROMIS Anxiety-Short Form, Functional Disability Inventory (FDI), and SAI-CP. The SAI-CP consists of 15 potentially anxiety-provoking school situations, and respondents rate how frequently they experience cognitive, physiological, and behavioral symptoms in these situations from 0 (“never”) to 4 (“always”). Total and symptom subscale scores were calculated, with higher scores indicating greater anxiety. Internal consistency was evaluated using Cronbach’s alpha (α). Pearson’s correlations assessed construct validity. Results: Internal consistency was excellent across three subscales: cognitive (α=0.96), physiological (α=0.96), and behavioral (α=0.96), and total scale (α=0.98). SAI-CP total scores were positively associated with the PROMIS Anxiety total score (r=0.58, p< .001) and FDI (self-report: r=0.34, p< 0.001; parent report: r=0.23, p=0.03). Discussion: Findings suggest that the SAI-CP has very high internal consistency, though this may indicate some redundancy or conceptual overlap in items. Preliminary evidence also supports the construct validity of the SAI-CP. Future work should establish the factor structure of the SAI-CP to improve clinical utility and inform treatment targets for school anxiety in youth with chronic pain.
-
 Prevention Rounds by Lacey Bergerhofer, Christian Anthony Schneider, and Emily Evans")
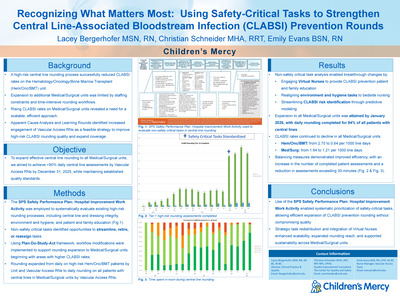
Recognizing What Matters Most: Using Safety-Critical Tasks to Strengthen Central Line-Associated Bloodstream Infection (CLABSI) Prevention Rounds
Lacey Bergerhofer, Christian Anthony Schneider, and Emily Evans
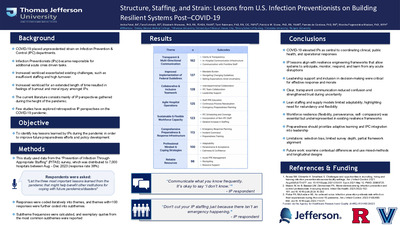
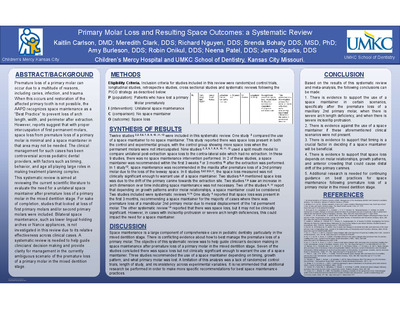
Background: Our CLABSI improvement team developed high-risk rounding processes on the Hematology/Oncology unit. Expanding this model to additional Med/Surg units was challenging due to limited staffing and time-intensive tasks required during rounds. Concurrently, CLABSI rates across other Med/Surg units increased, necessitating a scalable approach. Objectives: Apparent Cause Analysis (ACA) review in Med/Surg units identified an opportunity to strengthen surveillance by engaging Vascular Access subject-matter experts. Our proactive high-risk rounds pilot led to CLABSI rate reduction. The objective was to expand service coverage without compromising established high-risk rounding quality standards. Our goal is to assess > 90% of central lines in Med/Surg through daily high-risk rounding. Methods: We applied the SPS Safety Performance Plan: Hospital Improvement Work Activity to systematically evaluate existing high‑risk rounding processes. Non–safety‑critical tasks were identified, and an improvement team assessed opportunities to streamline, retire, or reassign. This analysis enabled breakthrough changes, including engaging virtual nurses to deliver CLABSI education. Utilizing Plan‑Do‑Study‑Act framework, we tested process modifications and refined workflow to support expansion beyond the Hematology/Oncology/BMT unit. Rounding extended first to Med/Surg areas with higher CLABSI rates, allowing resource prioritization and validating scalability of the revised model. Results: Hem/Onc CLABSI rates decreased from 2.70 to 0.64 per 1,000 line days (July–October 2025 vs. November 2025–January 2026). Med/Surg CLABSI rates declined from 1.64 to 1.21 per 1,000 line days, concurrent with expanding CLABSI rounding to all Med/Surg units by January 2026. On average, 88% of central‑line patients received high-risk rounds. The proportion of in-room assessment times under 15 minutes increased from 33.5% to 54.8%. Conclusions/Implications: Prioritizing safety-critical tasks strengthened continuous monitoring and enabled earlier risk mitigation through subject‑matter expert support. By reallocating non-critical tasks to existing hospital rounds and shifting education to virtual nursing, rounding across all Med/Surg units expanded. Frequent rounding supports adherence to interventions and lowers CLABSI risk.
-

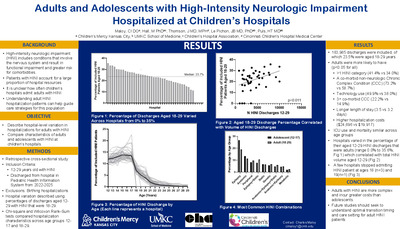
Adults and Adolescents with High-Intensity Neurologic Impairment Hospitalized at Children’s Hospitals
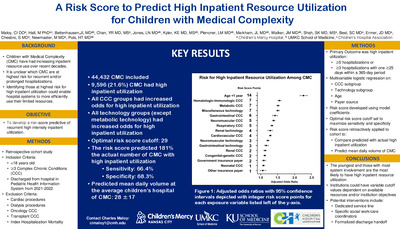
Charles Maloy, Matt Hall, Joanna Thomson, Jean-Baptist LePichon, and Henry T. Puls
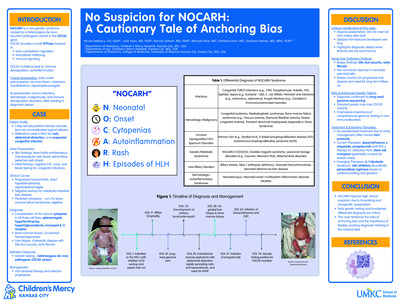
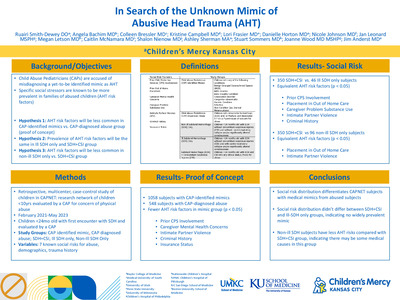
Introduction: Children with high-intensity neurologic impairment (HINI) account for a sizeable proportion of inpatient resources. As survival into adulthood for children with medical complexity increases, children’s hospitals will likely admit adults with HINI. Understanding adult HINI hospitalization patterns is necessary to develop effective care strategies for this population. Objective: Compare characteristics of adults and adolescents with HINI hospitalized at children’s hospitals and describe hospital-level variation in hospitalizations for adults with HINI. Methods: This retrospective cross-sectional study included discharges of patients with HINI aged 12-29 years from 41 children’s hospitals in the Pediatric Health Information System between 2022-24. Hospitals were excluded if birthing encounters were identified. Discharges were categorized by age: adolescents (12-17 years) and adults (18-29 years). Chi-square and Wilcoxon Rank-Sum tests compared hospitalization level characteristics (i.e., intensive care use, hospital length of stay, in-hospital mortality, and costs) across the two age groups. Hospital-level variation was described using the percentage of included HINI discharges that were adults and correlated with hospital volume of included HINI discharges using Pearson’s coefficient. Results: There were 136,290 discharges included; 23.6% were adults. Compared to adolescents, adults were more likely to have >1 HINI category (41.1% vs 33.9%), a co-morbid non-neurologic chronic complex condition (72.5% vs 58.5%), and technology use (49.2% vs 37.8%) (Table). Adults had slightly longer length-of-stay, similar ICU use, similar mortality, and higher hospitalization costs (Table). There was substantial hospital-level variation in the percentage of HINI hospitalizations that were adults (range 0.0% to 35.7%), which was correlated with hospital volume of all HINI discharges aged 12-29 years (p< 0.01). Conclusion: Adults with HINI were more complex and incurred longer hospitalizations and greater costs than their adolescent counterparts. Hospital-level variation in adults with HINI hospitalized at children’s hospitals was correlated with hospital volume of HINI discharges and may result from differences in the transition processes between institutions. Future studies should seek to understand optimal transition timing and care setting for adult HINI patients.
-

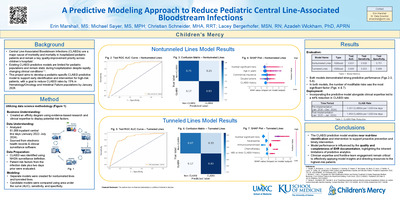
A Predictive Modeling Approach to Reduce Pediatric Central Line-Associated
Erin Marshall, Michael Sayer, Christian Anthony Schneider, Lacey Bergerhofer, and Azadeh Wickham
-

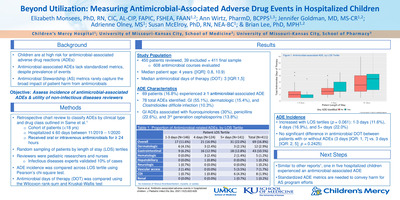
Beyond Utilization: Measuring Antimicrobial-Associated Adverse Drug Events in Hospitalized Children
Elizabeth Monsees, Ann L. Wirtz, Jennifer Goldman, Adrienne Olney, Susan F. McElroy, and Brian Lee
-

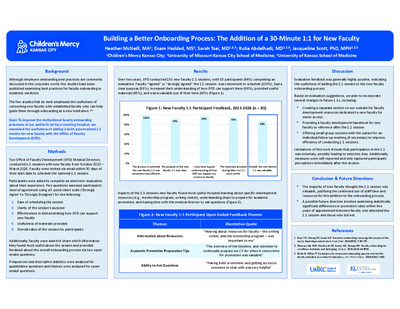
Building a Better Onboarding Process: The Addition of a 30-Minute 1:1 for New Faculty
Heather McNeill, Enam Haddad, Sarah Tsai, Ruba A. Abdelhadi, and Jacqueline Hill
Our faculty development office examined the addition of a 30-minute personalized 1:1 session to the broader faculty onboarding strategy at our pediatric teaching hospital. We surveyed 106 new faculty who participated in a session from 2023-2025 to assess its usefulness. Of the 69 (65.7%) respondents, a large majority (92%) “agreed” or “strongly agreed” that the session was a valuable use of their time. Several faculty commented that the most useful information was learning about career development resources (e.g., mentorship program, writing center), understanding how to prepare for academic promotion, and having time to ask questions. Most new faculty thought the 1:1 was valuable, justifying the use of time and staff resources to sustain this addition to the onboarding process.
-

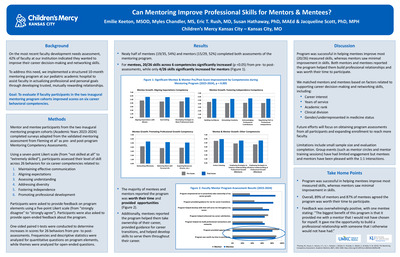
Can Mentoring Improve Professional Skills for Mentors and Mentees?
Emilie Keeton, MSOD; Myles Chandler; Eric T. Rush; Susan B. Hathaway; and Jacqueline Hill
Introduction/Background: We implemented a structured 10-month mentoring program at our pediatric academic hospital designed to assist faculty in actualizing professional and personal goals through developing trusted, mutually rewarding relationships. Goals/Hypothesis: To evaluate if faculty participants in the 2 inaugural mentoring program cohorts improve scores on 6 behavioral competencies related to maintaining effective communication, aligning expectations, assessing understanding, addressing diversity, fostering independence, and promoting professional development. Methods/Approach We used pre- and post-program Mentoring Competency Assessments to assess changes in 26 skills across 6 competencies and gather feedback on program elements from participants. Results/Outcomes: 19/35 (54%) mentees and 15/29 (52%) mentors completed both assessments. 20/26 rated skills across 6 competencies significantly increased for mentees (p < 0.05), while 4/26 rated skills across 6 competencies significantly improved for mentors. Overall, 89% of mentors and 87% of mentees agreed the program was worth their time to participate. Conclusion/Impact: Program was successful in helping mentees improve most skills across all 6 competencies, whereas mentors saw minimal improvement in skills. Both mentors and mentees reported the program helped them build professional relationships and was worth their time to participate. Future efforts will focus on obtaining assessments and enrolling more participants.
-

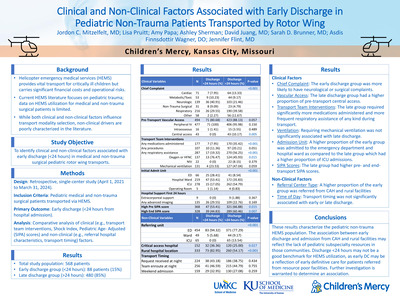
Clinical and Non-Clinical Factors Associated with Early Discharge in Pediatric Non-Trauma Patients Transported by Rotor Wing
Jordon Mitzelfelt, Lisa Pruitt, Amy Papa, Ashley K. Sherman, David Juang, Sarah Brunner, Asdis Finnsdottir Wagner, and Jennifer Flint
Objective: Helicopter emergency medical services (HEMS) are crucial for transporting critically ill children to definitive care, however, rising costs and relative risks of this type of transportation necessitate careful evaluation of potential over-utilization. Current literature primarily focuses on pediatric trauma patients, leaving a significant gap in data regarding non-trauma pediatric HEMS transports and the influence of non-clinical factors such as referral hospital distance, resources, and capabilities on transport decisions. This study aims to address these gaps by examining non-trauma pediatric HEMS patients and identifying associated clinical and non-clinical factors related to early hospital discharge (< 24 hours). Methods: This retrospective, single-center study includes pediatric patients with medical and non-trauma surgical diagnoses transported by HEMS between April 1, 2021 and March 31, 2024. Clinical data were extracted from transport team records and the hospital’s electronic health records. Analyses were performed to identify factors associated with discharge within 24 hours of admission. To identify predictors of early discharge, we analyzed clinical factors including chief complaint, pre-transport vascular access, transport crew interventions (medication administration and procedures), respiratory assistance, and Pediatric Age-Adjusted Shock Index (SIPA) scores. Additionally, we examined the impact of the initial admit unit, and medical support required within the first 24 hours of hospitalization. Non-clinical predictors included the referring hospital’s status (critical access and/or rural designation) and the time of transport. Results: A total of 568 patients were transported by HEMS, of whom 88 (15%) were discharged within 24 hours. Patients in the early discharge group were more likely to present with neurologic chief complaints (40%), whereas those remaining hospitalized beyond 24 hours more frequently presented with respiratory complaints (40%). Normal SIPA scores both prior to and at the conclusion of transport were significantly associated with early discharge (p=0.012 and p=0.011, respectively). Furthermore, patients requiring no medications or respiratory assistance during transport, or no respiratory support within the first 24 hours of admission, were significantly more likely to be discharged early (p< 0.001). Notably, all patients with central access prior to transport remained admitted for more than 24 hours (p=0.004). Regarding non-clinical factors, patients transported from designated rural hospitals were more likely to experience early discharge (p< 0.001). Conclusion: These results characterize the pediatric non-trauma HEMS population and identify key predictors of early hospital discharge. This data is essential for developing standardized dispatch criteria to mitigate over-utilization and ensure high-acuity transport is reserved for the most appropriate patients.
-

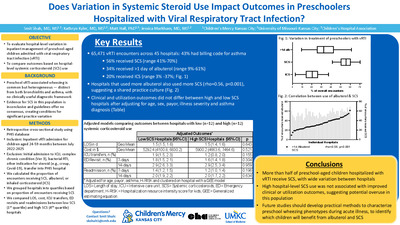
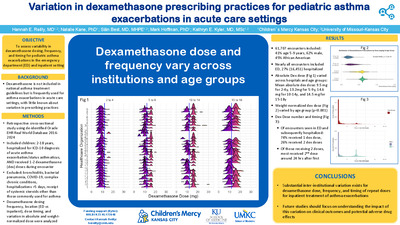
Does Variation in Systemic Steroid Use Impact Outcomes in Preschoolers Hospitalized with Viral Respiratory Tract Infection?
Smit Shah, Kathryn Kyler, Matt Hall, and Jessica Markham
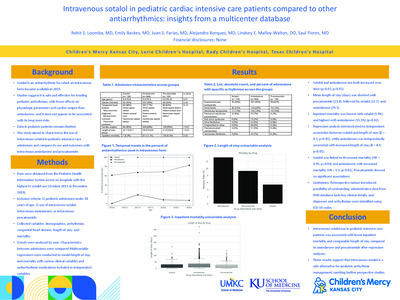
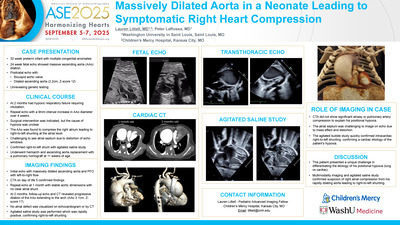
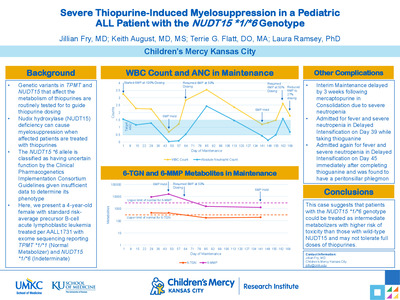
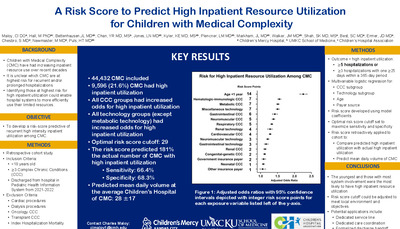
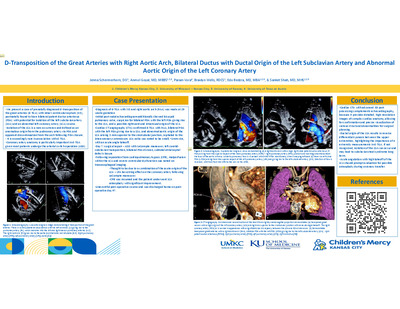
Background: Systemic corticosteroids (SCS) are a cornerstone of treatment for acute asthma exacerbation. However, the role of SCS in preschool-aged children hospitalized with viral respiratory tract infection (vRTI), including viral induced wheezing, remains uncertain. Clinical trials have reported conflicting results about the benefits of SCS in this population. Objectives: To evaluate hospital-level variation in inpatient management of preschool-aged children admitted with vRTI and to compare clinical and utilization outcomes based on hospital-level SCS use. Methods: We conducted a retrospective cohort study of children aged 24-59 months admitted to US children’s hospitals with vRTI from July 2022-July 2024 using the Pediatric Health Information System. We excluded encounters with complex chronic conditions, intensive care unit stays, bacterial RTIs (e.g., pneumonia, pertussis) and vRTI treated with SCS (e.g., croup, COVID-19). We calculated hospital-level proportion of encounters receiving SCS (including methylprednisolone, prednisone, prednisolone, dexamethasone), albuterol on ≥1 day, and inhaled corticosteroids (ICS). We grouped hospitals into quartiles based on the proportion of encounters receiving SCS. Generalized estimating equations were used to compare length of stay (LOS), ED revisits, readmissions, and costs between low SCS (1st quartile) and high SCS (4th quartile) hospitals, adjusting for age, sex, payor, illness severity, and asthma diagnosis. Results: We identified 44,848 vRTI encounters across 46 hospitals; 42.4% had an asthma diagnosis. On average, 55% of encounters received SCS (range: 39%-60%), 32.2% received ≥1 day of albuterol (range: 7%-56%), and 19.3% received ICS (range: 3%-37%) (Fig. 1). A positive correlation existed between hospital-level proportion of encounters receiving ≥1 day albuterol and hospital-level SCS use (Pearson’s r =0.52, p< 0.001) (Fig. 2). In unadjusted analyses, only 7-day revisit rates differed between low SCS hospitals (revisit rate=2.0%) and high SCS hospitals (revisit rate 1.6; p=0.014). In adjusted analyses, hospitals with low and high SCS use had similar LOS, ED revisits, readmissions, and costs (Table 1). Conclusions: Substantial hospital-level variation exists in use of SCS and albuterol among preschool-aged children hospitalized for vRTI. Hospitals with higher SCS use had similar outcomes compared to those with lower use. Our findings suggest potential overuse of SCS and highlight the need for more evidence to guide appropriate SCS use in preschool aged vRTI.
-

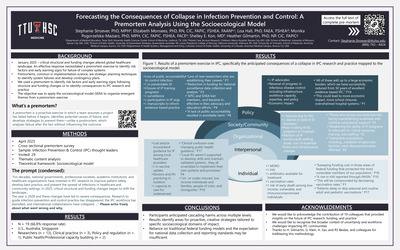
Forecasting the Consequences of Collapse in Infection Prevention and Control: A Premortem Analysis Using the Socioecological Model
Stephanie Stroever, Elizabeth Monsees, Lisa Hall, Monika Pogorzelska-Maziarz, Shelley E. Kon, and Heather Gilmartin
-

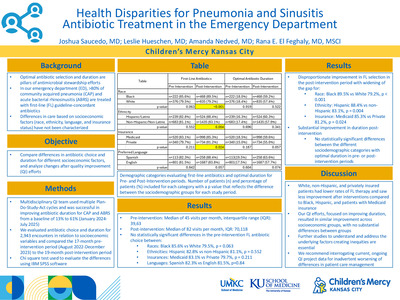
Health Disparities for Pneumonia and Sinusitis Antibiotic Treatment in the Emergency Department
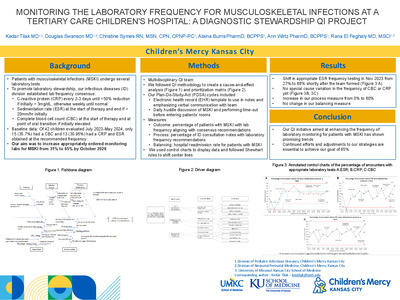
Joshua Saucedo, Leslie Hueschen, Amanda Nedved, and Rana El Feghaly MD
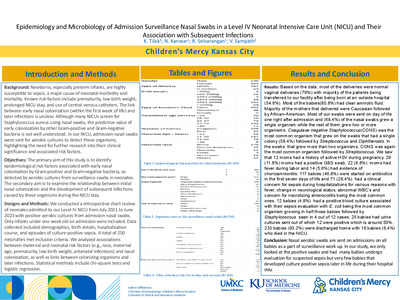
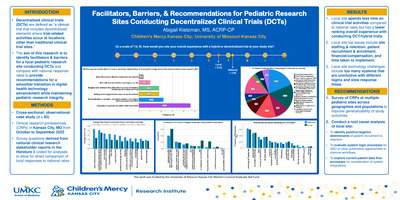
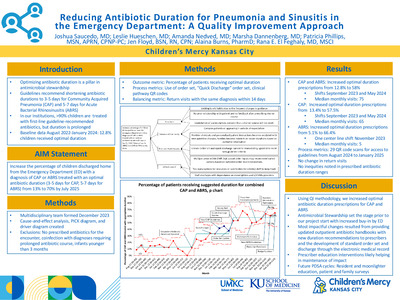
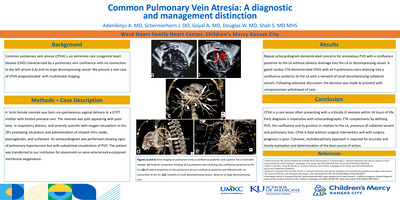
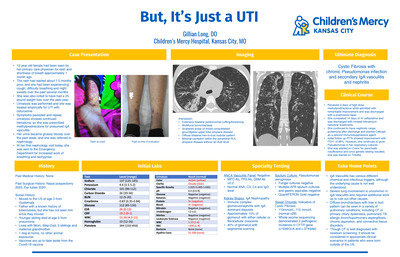
Optimal antibiotic selection and duration are pillars of antimicrobial stewardship efforts. In our emergency department (ED), >80% of community acquired pneumonia (CAP) and acute bacterial rhinosinusitis (ABRS) are treated with first-line (FL) guideline-concordant antibiotics. Differences in care based on socioeconomic factors (race, ethnicity, language, and insurance status) have not been characterized. We sought to compare differences in antibiotic choice and duration for different socioeconomic factors, and analyze changes after quality improvement (QI) efforts. Multidisciplinary QI team used multiple Plan- Do-Study-Act cycles and was successful in improving antibiotic duration for CAP and ABRS from a baseline of 13% to 61% (January 2024- July 2025). We evaluated antibiotic choice and duration for 2,943 encounters in relation to socioeconomic variables and compared the 17-month pre-intervention period (August 2022-December 2023) to the 19-month post-intervention period. Chi square test used to evaluate the differences using IBM SPSS software. Pre-intervention: Median of 45 visits per month, interquartile range (IQR): 39,63, Post-intervention: Median of 82 visits per month, IQR: 70,118. No statistically significant differences in the pre-intervention FL antibiotic choice between: Races: Black 85.6% vs White 79.5%, p = 0.063, Ethnicities: Hispanic 82.8% vs non-Hispanic 81.1%, p = 0.552, Insurances: Medicaid 83.1% vs Private 79.7%, p = 0.211, Languages: Spanish 82.3% vs English 81.5%, p=0.84.Disproportionate improvement in FL selection in the post-intervention period with widening of the gap for: Race: Black 89.5% vs White 79.2%, p < 0.001, Ethnicity: Hispanic 88.4% vs non- Hispanic 83.1%, p = 0.004, Insurance: Medicaid 85.3% vs Private 81.2%, p = 0.024. Substantial improvement in duration post- intervention. No statistically significant differences between the different sociodemographic categories with optimal duration in pre- or post-intervention periods. White, non-Hispanic, and privately insured patients had lower rates of FL therapy and saw less improvement after interventions compared to Black, Hispanic, and patients with Medicaid insurance. Our QI efforts, focused on improving duration, resulted in similar improvement across socioeconomic groups, with no substantial differences between groups. Further studies to understand and address the underlying factors creating inequities are essential. We recommend interrogating current, ongoing QI project data for inadvertent worsening of differences in patient care management
-

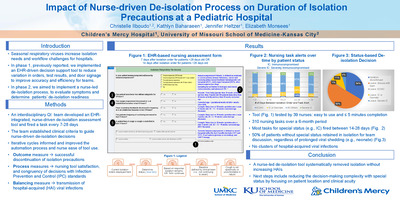
Impact of nurse-driven de-isolation process on isolation precautions duration at a Pediatric Hospital
Christelle Ilboudo, Kathlyn Baharaeen, Jenny Heltzer, and Elizabeth Monsees
-

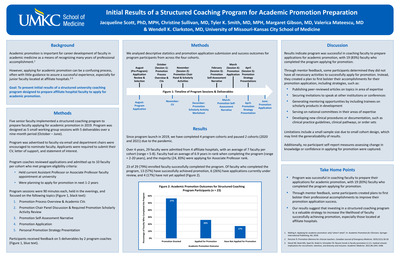
Initial Results of a Structured Coaching Program for Academic Promotion Preparation
Jacqueline Hill, Christine Sullivan, Tyler Smith, Margaret Gibson, Valerica Mateescu, and Wendell K. Clarkston
Introduction: Applying for academic promotion can be a confusing and arduous process, often with little guidance to assure a successful experience, especially for junior faculty located at affiliate hospitals. Goals: We present initial results of a structured university mentorship program to prepare faculty to apply for academic promotion. Methods: Program was designed as a small working group of 5 structured sessions over a 9-month period where participants were coached by senior faculty from 3 university affiliate hospitals. Program culminated in the completion of an academic promotion application. Results: Since launch in 2019, we have completed 4 program cohorts and paused 2 cohorts due to the pandemic. 23 of 29 (79%) enrolled faculty successfully completed the program. Majority (24, 83%) were applying for Associate Professor. Of faculty who completed the program, 13 (57%) have successfully achieved promotion, 6 (26%) have applications currently under review, and 4 (17%) have not yet applied. Conclusion: Program was successful in coaching faculty to prepare applications for academic promotion. Through mentor feedback, some participants determined they did not yet have all necessary activities to successfully apply for promotion and instead created a plan to first bolster scholarly accomplishments. Our results suggest that investing in structured coaching sessions is a valuable strategy to increase the likelihood of faculty successfully achieving promotion.
-

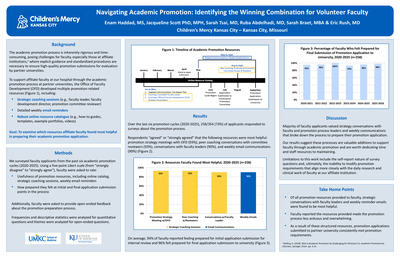
Navigating Academic Promotion: Identifying the Winning Combination for Volunteer Faculty
Enam Haddad, Jacqueline Hill, Sarah Tsai, Ruba A. Abdelhadi, Sarah Braet, and Eric T. Rush
Introduction/Background: Academic promotion is an arduous and time-consuming process. Implementation of support resources is essential for faculty success. Supporting faculty through the process, we developed multiple promotion resources, including a robust online resource catalogue, peer coaching sessions, and detailed weekly email reminders. Goals/Hypothesis: To examine which resources faculty find most helpful in preparing their academic promotion application. Methods/Approach: We surveyed promotion applicants from 6 cycles (2020-2025). Faculty rated the usefulness of promotion resources, how prepared they felt at different points in the promotion timeline, and provided feedback about the overall promotion preparation process. Results/Outcomes: 258/354 (73%) applicants responded to the survey. Respondents agreed or strongly agreed that the following resources were most helpful: promotion strategy meetings with faculty development director (93%), conversations with promotion committee reviewer (93%), conversations with faculty leaders (90%), and weekly promotion communications (90%). 94% of respondents reported feeling prepared for initial application submission for promotion committee review and 96% felt prepared for the final submission to university. Conclusion/Impact: Majority of faculty applicants value promotion conversations with multiple faculty and promotion process leaders and weekly outlined communications as they navigate the academic promotion process.
-

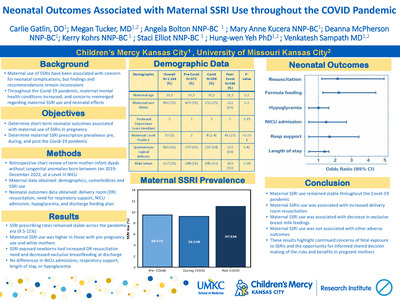
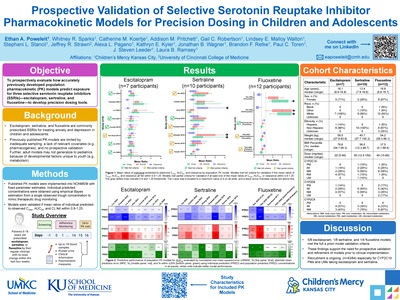
Neonatal Outcomes Associated with Maternal SSRI Use throughout the COVID Pandemic
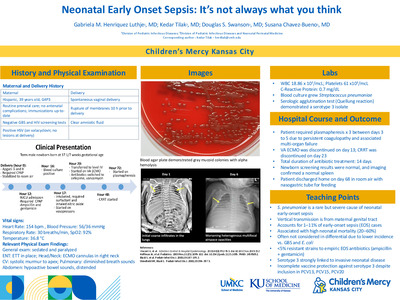
Carlie G. Gatlin, Megan Tucker, Angela Bolton, Mary Anne Kucera, Deanna McPherson, Kerry Kohrs, Staci S. Elliott, Hung-Wen Yeh, and Venkatesh Sampath
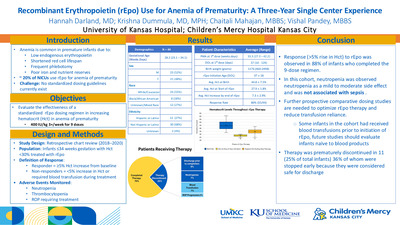
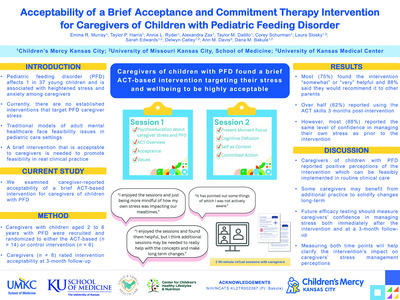
Background: Maternal antenatal selective serotonin reuptake inhibitor (SSRI) use has been suggested as a risk factor for neonatal complications, though evidence remains inconclusive. Mental health conditions increased during the COVID-19 pandemic, raising questions about SSRI prescription trends. This study examines associations between maternal SSRI use and neonatal outcomes across three time periods: before, during, and after the pandemic. Objectives: Primary: Determine if SSRI use in pregnancy is associated with NICU admission, respiratory support, hospital stay length, hypoglycemia, formula feeding, and/or delivery room resuscitation. Secondary: Assess SSRI prescription prevalence across pandemic phases. Methods: Retrospective chart review of term maternal-infant dyads born in Jan/June during each of the years of 2019–2022 in a level III NICU. Data included maternal demographics, SSRI use, comorbidities, and neonatal outcomes. Exclusions: congenital anomalies, multiple gestations, and preterm birth < 37 weeks. N=1,246. Categorical variables were compared using Chi-squared or Fisher’s exact test; continuous variables via Wilcoxon or Kruskal-Wallis tests. Regression models adjusted for COVID phase and covariates. Missing data (>5%) were imputed using MICE and random forest, with pooled results via Rubin’s rule. Results: Maternal SSRI use rates did not differ significantly across the 3 time periods (pre-Covid 54/572 9.5% vs. during Covid 31/338 9.3% vs. post-Covid 36/336 11%) (Table 1). SSRI use was highest among those with pre-pregnancy use (p=< 0.001), and white mothers (White 108/890 12% vs. Non-white 13/354 3.7 %, p= < 0.001) (Table 2). Infants exposed to SSRIs were more likely to require delivery room resuscitation (OR 2.51, 95% CI 1.19-5.26, p= 0.015) (Table 3B). Mothers using SSRIs were more likely to formula or combo feed rather than exclusively breastfeed (OR 2.86, 95% 1.68-4.85, p=0.000) (OR 1.91, 95% 1.05-3.47, p= 0.034) (Table 3F). No significant associations were found between maternal SSRI use and neonatal hypoglycemia, NICU admission, respiratory support, or length of stay (Table 3A,C,D,E). Conclusion: In our study, we did not find an increase in maternal SSRI use during the COVID pandemic. Maternal SSRI use was associated with increased delivery room resuscitation and non-exclusive breastfeeding, but not other adverse neonatal outcomes. These findings highlight the continued concerns of maternal SSRI use on neonatal outcomes, and advocate for careful consideration and discussion of its benefits vs. risks in pregnant mothers as expressed by recent FDA and ACOG statements.
-

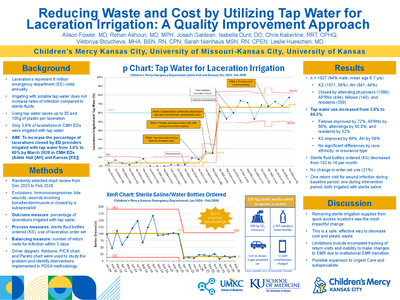
Reducing Waste and Cost by Utilizing Tap Water for Laceration Irrigation in the Emergency Department: A Quality Improvement Approach
Alison L. Fowler; Rohan Akhouri; Josaih Galdean; Isabella Dunt; Christopher Kaberline; Viktoriya Stoycheva MHA, RN, CPN; Sarah Nienhaus; and Leslie Hueschen
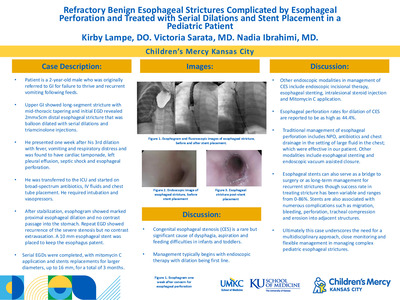
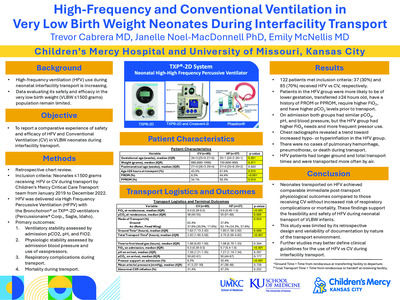
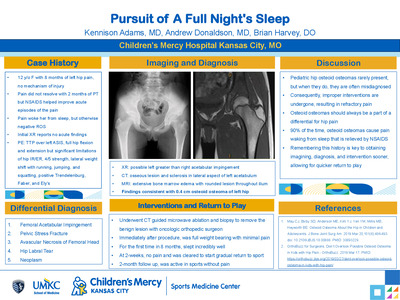
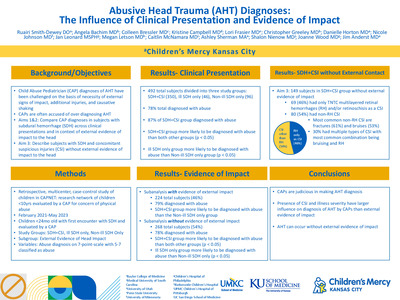
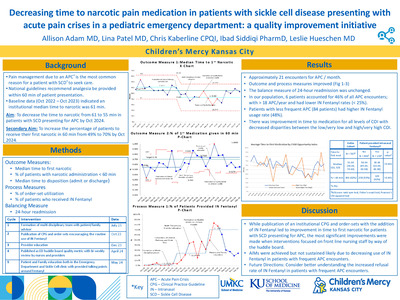
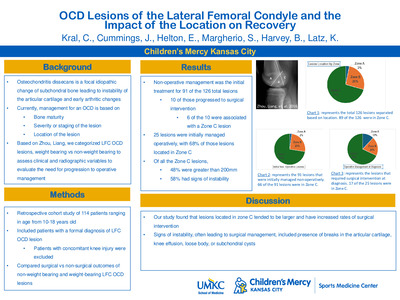
Purpose/Objective: Lacerations requiring closure make up 8 million emergency department (ED) visits annually. Irrigating prior to closure with potable tap water decreases cost and waste without increasing rates of infection compared to sterile fluids. Currently, only 3.5% of lacerations closed in our ED are irrigated with tap water. This project aims to increase the percent age of lacerations closed by ED providers irrigated with tap water from 3.5% to 60% by March 2026 in a freestanding pediatric emergency department across two sites (ED 1, ED 2). Design/Methods: A multidisciplinary team (physicians, nurses, QI consultant, parent advisors) formed in November 2024. Using driver diagram, fishbone, and PICK charts, interventions were identified and implemented in Plan-Do-Study-Act (PDSA) cycles (Table 1). The outcome measure was percentage of lacerations irrigated with tap water. Process measures were the number of sterile fluid bottles ordered for ED 2, order set usage, and rate of irrigation by nurses. The balancing measure was the rate of return visits for infection within 3 days. Fifty randomized charts were reviewed monthly. IRB deemed this study QI, not human subjects research. Results: Of 3,288 eligible encounters, 985 were randomized and included. Tap water irrigation increased from 3.5% to 64.6% (Fig 1). The average number of sterile bottles ordered monthly for ED 2 decreased from 102 to 16, representing a monthly savings of at least $430 and a reduction in plastic waste by at least 9 kg per month, reducing carbon emissions equivalent to 26 miles driven in a gas-powered car. There were no differences in irrigation by nurses or order set usage. There were no return visits for infection. Conclusion/Discussion: Altering the environment by removing sterile irrigation supplies from quick access locations was the most impactful intervention, allowing the team to meet their goal of increased tap water irrigation and decreased cost and waste. Future interventions include patient/family education and a new clinical pathway for lacerations. Limitations include inability to update order sets and limited monitoring of return visits. With the success of this project, the team plans to expand tap water irrigation to urgent care and subspecialist laceration repairs.
-

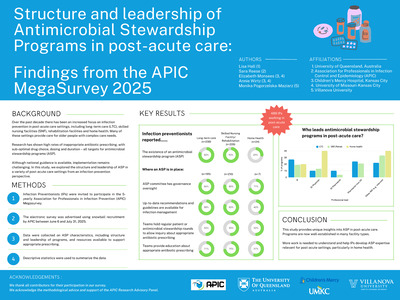
Structure and Leadership of Antibiotic Stewardship Programs in post-acute care: Findings from the APIC MegaSurvey 2025
Lisa Hall, Sara Reese, Elizabeth Monsees, Ann L. Wirtz, and Monika Pogorzelska-Maziarz
-

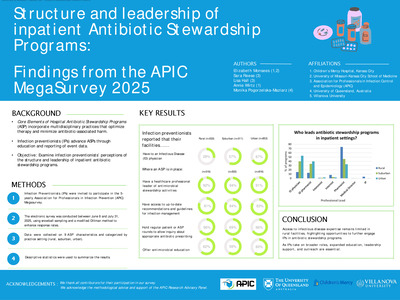
Structure and Leadership of Inpatient Antibiotic Stewardship Programs: Findings from the APIC MegaSurvey 2025
Elizabeth Monsees, Sara Reese, Lisa Hall, Ann L. Wirtz, and Monika Pogorzelska-Maziarz
-

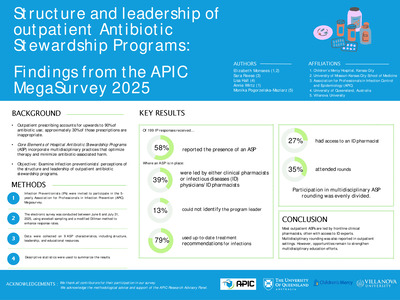
Structure and Leadership of Outpatient Antibiotic Stewardship Programs: Findings from the APIC MegaSurvey 2025
Elizabeth Monsees, Sara Reese, Lisa Hall, Ann L. Wirtz, and Monika Pogorzelska-Maziarz




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}