
These posters have been presented at meetings in Children's Mercy and around the world. They represent research that was done at the time they were created, and may not represent medical knowledge or practice as it exists at the time viewers access these posters.
-
 by Abby Kietzman")
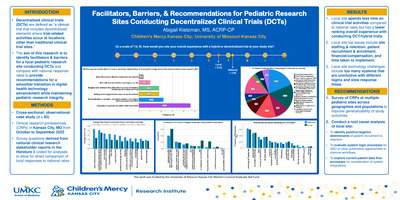
Facilitators, Barriers, & Recommendations for Pediatric Research Sites Conducting Decentralized Clinical Trials (DCTs)
Abby Kietzman
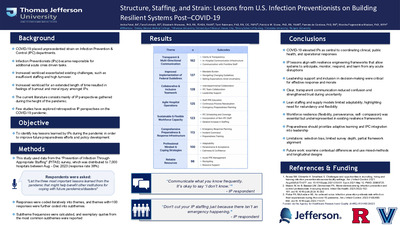
The COVID-19 pandemic drastically altered the way clinical research is conducted through a widespread adoption of telemedicine practices to continue clinical trial procedures during peak periods of global COVID-19 spread. Using telehealth/telemedicine services allows researchers to conduct “decentralized clinical trials”, or DCTs, for all or portions of study protocol procedures while maintaining safety measures implemented for pandemic control. However, research sites are hesitant to adopt DCT policies due to concerns around digital health technology, data safety and quality, and limited information in the literature specifically assessing telemedicine use for pediatric clinical research via DCTs or how equipped pediatric research sites are for the transition away from the site. A cross-sectional, observational casestudy surveying clinical research professionals (CRPs) at a local pediatric institution in Kansas City, MO, was conducted to better understand pediatric site facilitators and barriers to implementation and utilization of DCTs from a site perspective.
-
 by Ruairi Smith-Dewey, Angela Bachim, Colleen Bressler, Kristine Campbell, Lori Frasier, Danielle Horton, Nicole Johnson, Jan Leonard, Megan Letson, Caitlin McNamara, Shalon Nienow, Ashley K. Sherman, Stuart Sommers, Joanne Wood, and James Anderst")
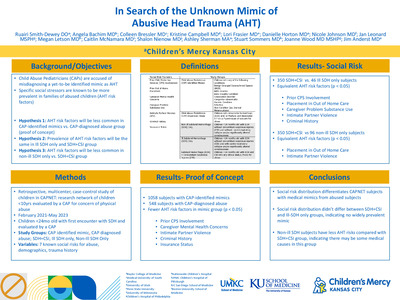
In Search of the Unknown Mimic of Abusive Head Trauma (AHT)
Ruairi Smith-Dewey, Angela Bachim, Colleen Bressler, Kristine Campbell, Lori Frasier, Danielle Horton, Nicole Johnson, Jan Leonard, Megan Letson, Caitlin McNamara, Shalon Nienow, Ashley K. Sherman, Stuart Sommers, Joanne Wood, and James Anderst
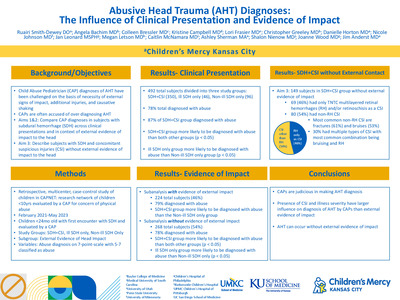
Background Child Abuse Pediatricians (CAPs) are accused of misdiagnosing a yet-to-be-identified mimic as abusive head trauma (AHT), particularly in ill children with an isolated subdural hemorrhage (SDH). Though not diagnostic criteria, specific social stressors are identified as AHT risk factors. The existence of a mimic can be assessed by comparing the prevalence of AHT risk factors across study groups (See Table 1). Objective We hypothesize that the distribution of AHT risk factors will be: fewer in the CAP-identified mimic group versus the CAP-diagnosed abuse group, no difference between ill SDH only and SDH+CSI groups as these are likely the same condition, and fewer in the non-ill SDH only versus SDH+CSI groups as there are likely undocumented known mimics in the non-ill SDH only group. Design/Methods Retrospective case-control study using Child Abuse Pediatrics Research Network (CAPNET) data from 10 sites over 27 months. As proof of concept, the prevalence of AHT risk factors was compared between CAP identified mimics and CAP-diagnosed abuse groups. Social risks were compared using unadjusted odds ratios with 95% confidence intervals. For social risk comparison across SDH groups, subjects were < 24 months old and evaluated by a CAP. Ill subjects had cardio-respiratory collapse and/or significantly altered consciousness. CSIs were injuries that are highly associated with abuse in the skin, bones, eyes, and abdomen. CAP diagnosis was not considered for SDH group determination. Prevalence of social risk, demographics, and trauma history were compared between groups using two one-sided equivalence tests with a 20% equivalence margin. Results In proof of concept, 1058 subjects with known medical mimics had statistically significantly fewer AHT social risk factors than 548 abused subjects with ICH/fracture in 5/7 domains. In the main study, when comparing the 350 SDH+CSI subjects and 46 Ill SDH subjects, the two groups were statistically equivalent in 5/7 social risks. When comparing the 350 SDH+CSI and 96 Non-Ill SDH subjects, they were statistically equivalent in 2/7 social risks. Provision of trauma history was equivalent across all three groups (RD –0.01-0.10). Conclusion(s) Social risk distribution differentiates CAPNET subjects with medical mimics from those without. Social risk distribution largely did not differ between SDH+CSI and Ill-SDH groups, indicating that a yet-to-be-identified mimic is not widely prevalent in the Ill-SDH group. Non-ill appearing subjects with SDH appear to have fewer AHT risks compared to SDH+CSI, supporting possible medical causes in some of these children.
-

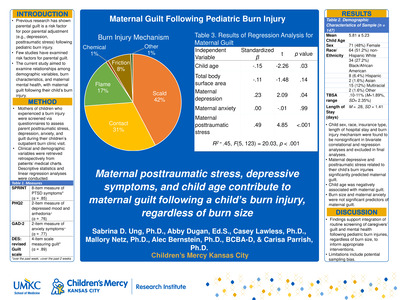
Maternal Guilt Following Pediatric Burn Injury
Sabrina Ung, Abby Dugan, Casey Lawless, Mallory Netz, Alec Bernstein, and Carisa Parrish
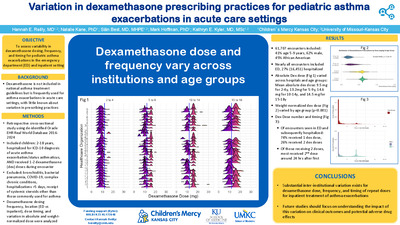
Background: Previous research has shown that parental guilt is a risk factor for poor parental adjustment (e.g., depression, posttraumatic stress) following a pediatric burn injury (Hawkins et al., 2019). However, few studies have examined risk factors for parental guilt. Objectives/Goal: The current study aimed to examine relationships among demographic variables, burn characteristics, maternal mental health, with maternal guilt following their child’s burn injury. Methods/Design: Mothers of 147 children who experienced a burn injury (mean child age = 6.28 years, 46% female, 44.7% White, 19.2% Black or African American, 9.6% Hispanic, 1.3% Asian, 11.9% multiracial, total body surface area range .10 – 15%) were screened using questionnaires assessing parent posttraumatic stress, depression, anxiety, and guilt during their children’s outpatient burn clinic visit. Clinical and demographic variables were retrieved retrospectively from patients’ medical charts. Descriptive statistics and linear regression analyses were conducted. Several demographic factors (e.g., child’s sex, race, insurance type) and burn injury characteristics (e.g., length of hospital stay, burn injury mechanism) were found to be nonsignificant in bivariate correlational and regression analyses and therefore were excluded in final analyses. Results: Maternal depressive symptoms (β = .23, p = .04) and posttraumatic stress related to their child’s burn injuries (β = .49, p = < .001) significantly predicted maternal guilt. Mothers of younger children were observed to experience higher levels of guilt (β = -.15, p = .03). Lastly, burn size (β = -.11, p = .14) and maternal anxiety (β = .00, p = .99) were not significant predictors of maternal guilt. Conclusions: Following a burn injury, maternal posttraumatic stress, depressive symptoms, and child age contribute to maternal guilt related to the injury regardless of burn size. Findings support integration of routine screening of caregivers’ guilt and mental health following pediatric burn injuries, regardless of burn size, to inform appropriate interventions.
-

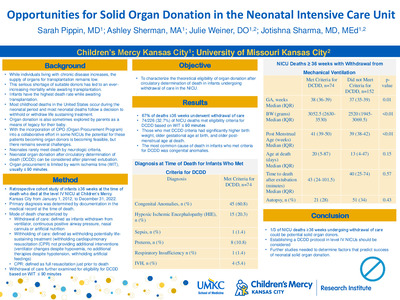
Opportunities for Solid Organ Donation in the Neonatal Intensive Care Unit
Sarah Pippin, Ashley Sherman, Julie Weiner, and Jotishna Sharma
Background: Pediatric patients are at an increased risk of mortality when waiting for an organ transplant. Approximately 50% of pediatric patients wait for> a year for a solid organ transplant and infants < 1 year of age have the highest death rate while awaiting transplantation. There are two pathways for organ donation (OD), donation after death by neurologic criteria (DDNC) or donation after circulatory determination of death (DCDD). Neonates rarely meet brain death criteria, and since most deaths in the NICU occur aftera planned extubation, DCDD with organ procurement after a planned extubation from mechanical ventilation can be a consideration especially with kidney and liver donations. Organ procurement may be limited by warm ischernic time (WI1); usually :'.S 90 minutes. The question remains which neonates would meet criteria for DCDD.
Purpose: The aim of this study is to characterize theoretical eligibility of DCDD in infants undergoing withdrawal of care in the NICU based on WIT :'.S 90 minutes
Method: Retrospective study of a cohort of infants 2:36 weeks at the time of death who died at a level IV NICU from January 1, 2012, to December 31, 2022. Demographic information was obtained. Mode of death was categorized as withdrawal of care, withholding of care, or CPR. The withdrawal of care was further examined for eligibility for DCDD based on WIT :'.S 90 minutes.
Results: During the study period, there were 337 infants 2': 36 weeks at the time of death and of those, 67% (226/337) infants had withdrawal of care. The most co=on cause of death was congenital anomalies. Those who met DCDD criteria were found to have significantly higher birth weight (p=< 0.01), older GA at birth (p=0.01), and older PMA at death (p=
Conclusion: One third ofNICU deaths 2::36 weeks undergoing withdrawal of mechanical ventilation could be potential solid organ donor after DCDD with WIT ::S 90 minutes. Increased organ donation opportunities in this age group could have an impact for pediatric patients waiting for an organ transplant. Establishing a DCDD protocol in level IV NICUs should be strongly considered. Further studies are needed to determine factors that predict success of neonatal solid organ donation through DCDD.
-

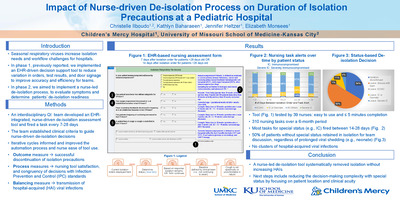
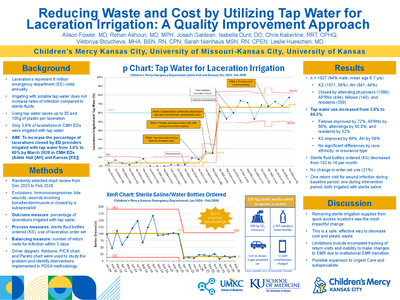
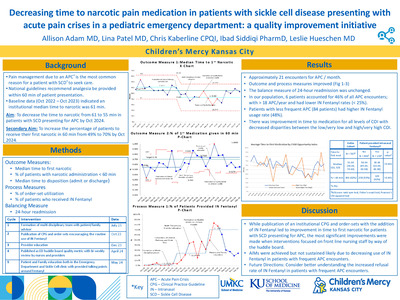
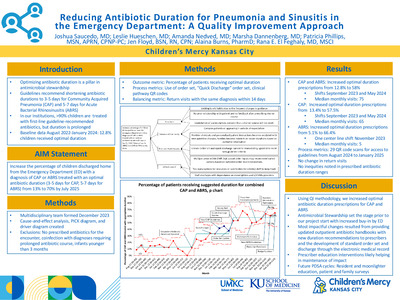
Reducing Antibiotic Duration for Pneumonia and Sinusitis in the Emergency Department: A Quality Improvement Approach
Joshua Saucedo, Leslie Hueschen, Amanda Nedved, Marsha Dannenberg, Patricia Phillips, Jennifer Floyd, Alaina N. Burns, and Rana El Feghaly
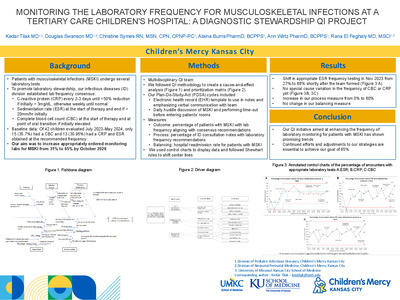
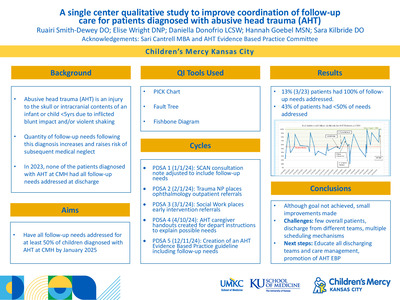
Background: Antibiotic duration is one of the pillars of antimicrobial stewardship programs (ASP) as it helps to limit unnecessary antibiotic exposure while continuing to provide appropriate care for infections. In our emergency department (ED), clinicians are using first-line guideline-recommended antibiotics as an appropriate choice for most patients (per our ASP report tracking), however, duration continues to be prolonged especially for community acquired pneumonia (CAP) and acute bacterial rhinosinusitis (ABRS). National guidelines recommend shortening antibiotic durations to 3-5 days for CAP and 5-7 days for ABRS, however currently only 22% of patients discharged from our ED receive the recommended duration. Objective: Our aim is to increase percentage of children discharged home from the ED with a diagnosis of CAP or ABRS treated with an optimal antibiotic duration (5 days or less for CAP, 7 days or less for ABRS) from 22% to 70% by July 2025, while assessing for differences in care based on demographic and socioeconomic factors. Design/Methods: A multidisciplinary team (infectious diseases physicians, ED and urgent care physicians, advanced practice providers, nurses, and pharmacy) formed in December 2023. Outcome metric is the percentage of patients receiving recommended antibiotic duration for CAP or ABRS; data trends analyzed monthly and process changes implemented according to the SPC Out of Control Process Western Electric rule set. Process metrics include use of order set, quick discharge order set, and QR code. Balancing metric is the number of return visits with the same discharge diagnosis within 14 days. Utilizing cause-and-effect diagram, driver diagram (Figure 1), and PICK chart (Figure 2), we identified possible interventions. Plan-Do-Study-Act cycles so far have included implementation of new internal CAP, updates to electronic medical record and quick discharge order sets. A survey of prescriber comfort with shorter duration identified barriers and provided education, which has led to posting evidence for lower duration treatment to prescribers in their workrooms and developing new ABRS CPG. Results: We have shifts in the central line of our overall outcome in August 2023, May and July 2024 to 65.4% with no change in balancing metric (Figures 3A-CQBS, annotated with PDSA cycles). Discussion: We have seen a reduction in the duration of antibiotics for CAP and ABRS with electronic medical record and prescriber education interventions. Future cycles will focus on barrier mitigation and increased data transparency, with huddle board reminders and positive encouragement to providers.
-

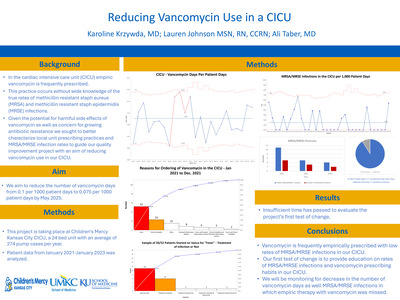
Reducing Vancomycin in a CICU
Karoline Krzywda, Lauren Johnson, and Allison Taber
Introduction: In the cardiac intensive care unit (CICU) empiric vancomycin is frequently prescribed. This practice occurs without wide knowledge of the true rates of methicillin resistant staph aureus (MRSA) and methicillin resistant staph epidermidis (MRSE) infections. Given the potential for harmful side effects of vancomycin as well as concern for growing antibiotic resistance we sought to better characterize local unit prescribing practices and MRSA/MRSE infection rates to guide our quality improvement project with an aim of reducing vancomycin use in our CICU. Methods: This project is taking place at Children’s Mercy Kansas City CICU, a 24 bed unit with an average of 274 pump cases per year. Patient data from January 2021-January 2023 was analyzed. There were approximately 20-60 vancomycin days per month with a center line of 0.1, indicating that over that time frame, 10% of the patient days were vancomycin days. In 2021 there were 111 orders for Vancomycin. Using a Pareto chart, we found that a majority (52) of Vancomycin orders were for fever alone. We analyzed all positive cultures in 2021 and of the 111 vancomycin orders there were only 11 positive MRSA/MRSE infections for which Vancomycin was prescribed as a full treatment course. We aim to reduce the number of vancomycin days from 0.1 per 1000 patient days to 0.075 per 1000 patient days by May 2025. Given the mismatch between prescribing habits and true infection rates, our first test of change will be to provide education regarding MRSA/MRSE infection rates in the CICU and current prescribing habits. Additionally, we will ask that providers not order vancomycin if a patient has a fever alone without hemodynamic instability, without high or increasing inflammatory markers, has not had a heart transplant, is not on extracorporeal membrane support or a ventricular assist device or is not immunocompromised. As a balancing measure we will track MRSA/MRSE positive cultures that did not receive vancomycin prior to culture results. Results: Insufficient time has passed to evaluate the project’s first test of change. Conclusions: Vancomycin is frequently empirically prescribed with low rates of MRSA/MRSE infections in our CICU. Our first test of change is to provide education on rates of MRSA/MRSE infections and vancomycin prescribing habits in our CICU. We will be monitoring for decrease in the number of vancomycin days as well MRSA/MRSE infections in which empiric therapy with vancomycin was missed.
-

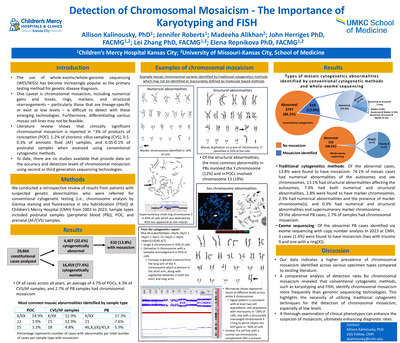
Detection of Chromosomal Mosaicism- the Importance of Karyotyping and FISH
Allison Kalinousky, Jennifer Roberts, Madeeha Alikhan, John Herriges, Lei Zhang, and Elena Repnikova
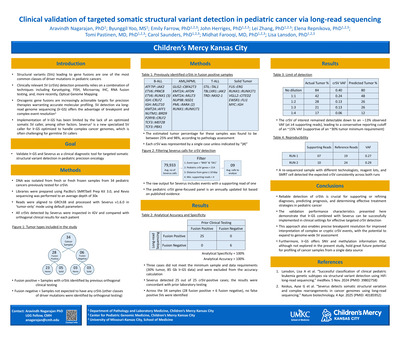
Introduction: The use of whole-exome/whole-genome sequencing for the detection of sequence-level variants and copy number variations (CNV) is increasingly being adopted as a primary testing method for genetic disease diagnosis by many institutions. Additionally, long-read sequencing is a promising technique to capture not only sequence level variants and CNVs but also structural chromosomal abnormalities. Significant progress has been achieved in this field; however, the detection of chromosomal mosaicism, including numerical gains and losses, rings, markers, and structural rearrangements – particularly those that are lineage-specific or exist at low levels – might still pose challenges with these emerging technologies. Furthermore, differentiating various mosaic cell lines may not be feasible. Literature review shows that chromosomal mosaicism is estimated to occur in up to 70% of human preimplantation embryos. Clinically significant chromosomal mosaicism is reported in ~3% of products of conceptions (POC), 1-2% of chorionic villus sampling (CVS), 0.1-0.3% of amniotic fluids (AF) samples, and 0.05-0.1% postnatal samples when assessed using conventional cytogenetic methods. To date, there are no studies available that provide data on the accuracy and detection levels of chromosomal mosaicism using third of fourth generation sequencing technologies. Methods: We conducted a retrospective review of patients who underwent conventional cytogenetic testing (chromosome analysis via Giemsa staining and fluorescence in situ hybridization (FISH)) for various clinical indications at Children’s Mercy Hospital from 2003 and 2023. Within this period, we received 20,866 constitutional cases of with 4,414 were cytogenetically abnormal. We also evaluated 762 cases submitted for exome sequencing with copy number analysis in 2023. We then examined all mosaic cases. Results: We found that the average number of mosaic cases each year was 29 (range: 9-39), accounting for ~3.1% of all clinical cases studied and ~14% of all abnormal cases per year. Levels of mosaicism were variable, ranging from 4 to 95%. Of all cases (both normal and abnormal) across all years, 4.7% of POCs, 4.3% of AF samples, and 2.7% of peripheral blood (PB) samples had chromosomal mosaicism. In comparison to the 762 PB exome cases, only three were mosaic (two with trisomy 9 and a ring(X)) totaling ~0.4% of postnatal cases. Numerical abnormalities are the most common form of mosaicism in our cohort, accounting for ~79% of mosaic cases. Of the numerical abnormalities, sex chromosomes are the most frequently implicated, with an average involvement of 44% in POCs, 40% in AF samples, and 79% in PB. The most common numerical abnormality of the autosomes in POCs were affecting chromosomes 22 (7%), 15 (6%), and 16 (5%); in AF samples affecting chromosomes 21 (20%), 18 (7.5%), and 22 (5%); and in PBs affecting chromosomes 21 (11%) and 18 (4%). Approximately 14% of mosaic cases harbored a structural abnormality of the autosomes. The most common abnormality in PBs involved the Y chromosome (12%), and in POCs involved chromosome 13 (19%). The structural abnormalities in AF samples affected chromosomes 3, 7, 9, 12, 14, 16, 18, and 22 at relatively equal prevalence. Discussion: Review of our data indicates a higher prevalence of chromosomal mosaicism identified through conventional cytogenetic methods across various specimen types compared to existing literature. Furthermore, our limited genomic sequencing data suggests that conventional cytogenetic technologies may detect chromosomal mosaicism more frequently than genomic technologies. These findings underscore the importance of employing karyotyping and FISH for the detection of chromosomal mosaicism, particularly at low levels, which may be missed by genomic sequencing. Additionally, a thorough examination of clinical phenotypes can enhance the suspicion of mosaicism, ultimately enhancing diagnostic rates.
-

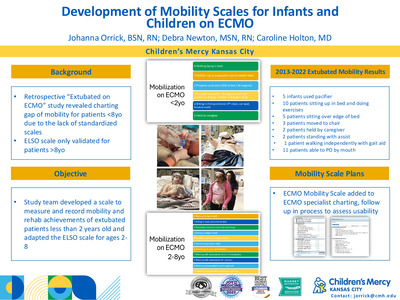
Development of Mobility Scales for Infants and Children on ECMO
Johanna I. Orrick, Debra E. Newton, and Caroline Holton
Extracorporeal Membrane Oxygenation (ECMO) is a life-saving intervention commonly used in pediatric and neonatal intensive care; however, it presents unique challenges for maintaining patient mobility. Early mobility contributes to better long-term outcomes. Existing mobility scales by the Extracorporeal Life Support Organization (ELSO) are limited to patients aged 8 years and older, leaving a gap for younger populations. This study aimed to develop and validate mobility scales specifically for infants (< 2 years) and children aged 2-8 years undergoing ECMO therapy. Through a collaborative effort involving pediatric ECMO specialists, physicians, and critical care nurses, we adapted ELSO’s mobility criteria to be developmentally appropriate for these younger age groups. For infants, mobility benchmarks include passive and active limb movements, head control, and supported sitting. The criteria for children aged 2-8 is expanded to include sitting, supported standing, and age-appropriate gross motor activities. This scale provides graded levels of mobility that accommodate ECMO-specific safety considerations, allowing practitioners to chart interventions according to each child’s developmental and physiological capacity. The resulting scales are being pilot-tested at our large ECMO center, with data showing preliminary effectiveness at capturing the degree of mobility achieved during ECMO runs. This mobility scale fills a critical need by providing structured charting guidelines for mobilizing infants and young children on ECMO, promoting functional recovery and potential improvements in long-term developmental outcomes. Further studies are recommended to establish consistency across institutions and confirm the scale's impact on mobility outcomes in pediatric ECMO patients.
-

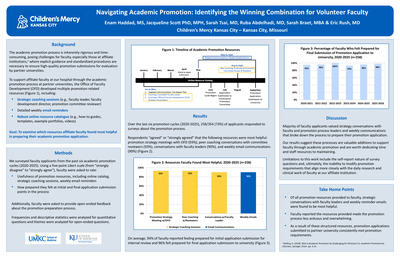
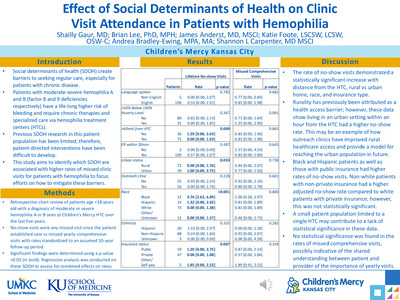
Effect of Social Determinants of Health on Clinic Visit Attendance in Patients with Hemophilia
Shailly Gaur; Brian Lee PhD, MPH; James Anderst MD, MSCI; Katie Foote LSCSW, LCSW, OSW-C; Andrea Bradley-Ewing MPA, MA; and Shannon L. Carpenter
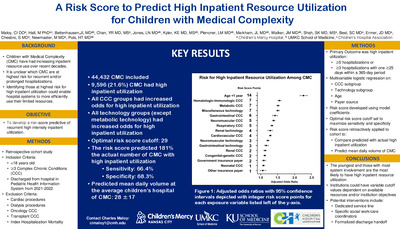
Background Social determinants of health (SDOH) create barriers to seeking care regularly, especially for patients with chronic disease. Patients with moderate-severe hemophilia A and B (factor 8 and 9 deficiencies respectively) have a life-long higher risk of bleeding and require chronic therapies. Specialized care is offered through hemophilia treatment centers (HTCs); however, these can be difficult to access for some individuals. Previous SDOH research in this patient population has been limited; therefore, it can be difficult to identify the barriers to care that exist. There is a need to examine SDOH more thoroughly to create patient-directed interventions to improve access to care. Objectives To identify common SDOH affecting patients with moderate-severe hemophilia and determine how each impacts clinical utilization within a single HTC. Methods A retrospective chart review of patients age < 18 years old with a diagnosis of moderate or severe hemophilia A or B seen at Children’s Mercy Hemophilia Treatment Center over the last five years. Dependent variables included no-show visits, which were any missed visit since the patient established care, and missed yearly comprehensive visits, of which non-parametric distributions were calculated. Rates were standardized to an assumed 10-year follow-up period and then compared across independent variables including race, ethnicity, language spoken, insurance type, rural vs urban home, food insecurity rate, poverty level, distance to an ER and to the HTC using the Kruskal-Wallis and Wilcoxon rank-sum tests, where appropriate. Significant findings were determined using a p-value < 0.05. Results Patients with the following SDOH had a statistically significant difference in rates of no-show visits: distance >60min from the HTC (p=0.009), urban vs rural home county (p=0.033), race of patient (p< 0.001), and insurance status (p=0.007). [Figure 1] Further demographic data and analysis included with confidence intervals provided in Fig 1. Conclusions The rate of no-show visits was most affected by patient race, insurance type, distance from HTC, and urban vs rural living conditions. No statistically significant correlations existed within the yearly comprehensive visits, which may be indicative of the shared importance of keeping regularly scheduled appointments between patient and provider when caring for a chronic disease. Interestingly, though previous data in this field has demonstrated rurality as a limitation to care, these findings suggest that an urban setting closer to the HTC presented more of an issue. These findings also help support the benefits of outreach clinics in providing specialized care directly in rural environments, likely reducing no-show rates in this population. This may inspire a similar approach to localized outreach within the urban neighborhoods affected by SDOH limitations to offer clinics where patients are most vulnerable.
-

Engineering A Novel Treg Population to Control Autoimmune Diabetes
Sofia Colon Guzman, Elly Puckett, Ryan T. Fischer, and Mary Markiewicz
Purpose Type 1 diabetes (T1D) in an autoimmune disorder where T cells attack islet cells, which are the pancreatic cells responsible for insulin production. T1D affects about 1 in 500 children in the United States and is one of the most common chronic diseases in pediatrics. Currently, insulin is the most effective treatment for T1D However, it does not change the underlying disease, and patients still experience many complications throughout their lifetimes. With a significant increase in the prevalence of T1D in children and adolescence in the past two decades, it’s important to explore therapies that alter the immune response as a possible way to reverse or even prevent the progression and development of this disease. One approach being investigated is to use regulatory T cells (Tregs), which can suppress the function of autoreactive T cells, as treatment for autoimmune disease. However, using a patient’s own naturally occurring Tregs (nTregs) as therapy poses several challenges. Therefore, we developed a novel way to generate human engineered Tregs (eTregs) from conventional T cells (Tconvs) by expressing both FOXP3 and HELIOS in both CD4+ and CD8+ Tconvs. We hypothesize that these novel eTregs will be as, or more, effective in their suppressive abilities against islet-specific effector T cells and be more stable under inflammatory conditions compared to naturally occurring Tregs. Methods We isolated CD8+ T cells from healthy human donors through negative selection using magnetic beads. From these cells we created cytotoxic T cells (Tconvs) through lentiviral transduction of a vector that expressed a TCR specific for an islet-specific antigen (IGRP) presented in HLA-A2:01 and mCherry as a fluorescent marker of transduction. The presence of IGRP-specific TCR was confirmed using dextramer staining. These Tconvs were co-cultured with BetaLox5 cells, an immortalized human cell line derived from islet cells. The response of the CD8+ Tconvs was determined by measuring effector cytokine release. We also created autologous natural Tregs (nTregs) and tested the ability of these cells to reduce the CD8+ Tconv response against BetaLox5Unpaired T test analysis was used to measure the statistical difference in cytokine production between co-culture conditions. Summary of Results IGRP-specific T cells responded to the human islet cell line BetaLox5 in vitro, demonstrated by elevated IFN-γ and TNF- production after co-culture. This response was decreased when nTregs were present in co-culture, as the amount of IFN-γ and TNF- in co-culture supernatant was significantly lower. Conclusions We were able to create a model to test the immunosuppressive capacity of Helios+FOXP3+ eTregs compared to nTregs against islet-specific autoreactive T cells. We also showed that nTregs decrease the response of these cytotoxic T cells when co-cultured with BetaLox5 cells. We are now comparing the immunosuppressive ability of our eTregs to nTregs in this assay, as well as comparing their stability under inflammation.
-

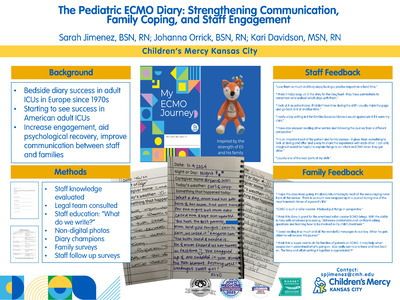
The Pediatric ECMO Diary: Strengthening Communication, Family Coping, and Staff Engagement
Sarah P. Jimenez, Johanna I. Orrick, and Kari L. Davidson
Bedside diaries have been used in Adult Intensive Care Units (ICUs) in Europe since the 1970s. These journals encourage clinicians to record a patient’s progress, illness narrative, and daily occurrences. Adult ICUs in America are beginning to implement and study the benefits of ICU journals. Bedside journals have been shown to increase staff engagement and aid in psychological recovery for patients and families following their illness. These diaries improve communication between the healthcare team and families, and help patients make sense of ICU stays by filling in memory gaps. Studies on ICU diaries have shown that a bedside diary kept throughout an ICU stay can decrease anxiety levels, decrease depression, decrease symptoms of post-traumatic stress disorder (PTSD), and improve an ICU survivor’s quality of life. This project examines the impact of bedside diaries on families with patients on Extracorporeal Membrane Oxygenation (ECMO) support and the staff that cares for them. The hospital legal team and Family Advisory Board were consulted in the diary development. A survey was sent to ECMO staff to evaluate existing knowledge of ICU diaries. Education was provided through department meetings. Diary champions were recruited to audit diaries. Diaries included non-digital photographs. Family members completed a survey after their loved one’s ECMO run and completion of the diary. Common themes from family surveys included: “loved,” “great,” “perspective,” “roller coaster,” “traumatic time,” “amazing,” “encouraging,” “awesome,” and “cute.” Families expressed that the diaries helped humanize the ECMO staff and care providers, fostering a more personal connection. A follow-up survey was conducted with ECMO staff to assess their perceptions. Common themes from the staff post survey included: “enjoyment,” “coping," “useful,” and “value.” Patient diaries have a positive psychological effect on family members, serving as a powerful rapport-building tool. Families and staff provided positive feedback, noting increased engagement and improved communication.
-

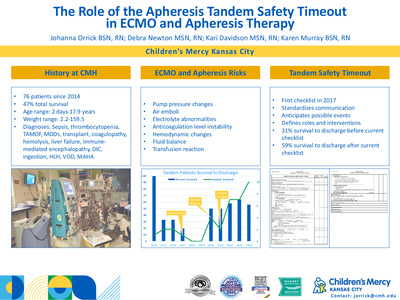
The Role of the Apheresis Tandem Safety Timeout in ECMO and Apheresis Therapy
Johanna I. Orrick, Debra E. Newton, Kari L. Davidson, and Karen Murray
The Apheresis Tandem Safety Timeout was implemented in 2017 at Children’s Mercy Hospital (CMH) to ensure safe, coordinated care when performing therapeutic plasma exchange (TPE) alongside Extracorporeal Membrane Oxygenation (ECMO). The first tandem procedure at CMH was performed in 2013, introducing a valuable tool for treating the sickest patients in the region. However, when patients are placed on two extracorporeal circuits simultaneously, the risk of complications increases significantly. These include electrolyte imbalances, anticoagulation challenges, hemodynamic instability, and the potential for either circuit to be compromised. The ECMO and Apheresis team recognized that even minor miscommunication could lead to life-threatening complications in these complex tandem therapies. Checklists are widely recognized in healthcare as effective tools to promote safety and identify human error before critical events occur. A checklist was developed to mitigate the increased risk of abnormalities in electrolytes, anticoagulation levels, and hemodynamics by ensuring that each team member understands the potential issues identified and addresses them before initiating apheresis on ECMO patients. The Apheresis Tandem Safety Timeout checklist facilitates closed-loop communication, defining roles, verifying system readiness, and identifying possible adverse events that may arise during the procedure. Given the high likelihood of technical challenges, such as maintaining blood flow in two circuits simultaneously, avoiding pressure differentials, and managing the risk of air emboli, the checklist ensures that the ECMO and Apheresis team are thoroughly prepared for each tandem procedure. By standardizing communication, the checklist enhances team coordination and reduces the likelihood of system failures or patient complications. The ongoing refinement of the checklist, based on quantitative and qualitative data from each procedure, has led to safer, more efficient tandem therapies. The checklist remains a vital tool in managing the complexity of these cases, allowing multiple teams to provide optimal care to critically ill patients who require simultaneous extracorporeal therapies.
-

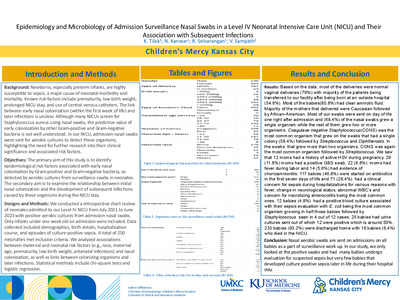
Viral Detection in Anterior Nasal Swabs Versus Nasopharyngeal Swabs in Children
Nicole Neeley, Abby Kietzman, Rangaraj Selvarangan, Dithi Banerjee, Jennifer Goldman, and Jennifer Schuster
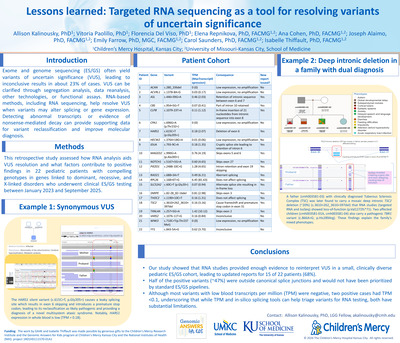
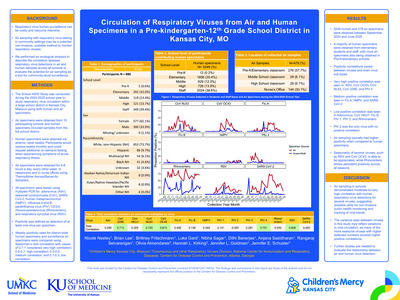
Background: Respiratory viruses are a significant cause of pediatric illness and healthcare utilization. Diagnostic testing for respiratory viruses is generally performed using nasopharyngeal (NP) specimens obtained by trained medical staff, limiting testing to medical settings. Evaluating additional sampling methods in children, such as anterior nasal swab (NS) specimens may expand access to diagnostic testing and aid public health surveillance. Methods: Eligible children hospitalized at Children’s Mercy Hospital in Kansas City who had a standard of care NP specimen collected for nucleic acid amplification testing for respiratory viruses were enrolled. Research NS specimens were obtained through self, caregiver, or staff collection. Specimens were tested on QIAstat-Dx-Analzyer using QIAstat-Dx Respiratory SARS-Cov-2 Panel and included: adenovirus, seasonal coronavirus (229E, HKU1, NL63, OC43), SARS-CoV-2, human metapneumovirus (hMPV) A+B, influenza A/A H1/A H3/A H1N1/pdm09, influenza B, parainfluenza virus 1/2/3/4, rhinovirus/enterovirus (RV/EV), and respiratory syncytial virus (RSV) A+B. Statistical analysis for sensitivity with 95% confidence intervals was calculated with NP as the gold standard. Further sub-analysis evaluating time to NS collection and test results (NP specimens as time zero and NS specimens grouped from 1-24 hours, 25-48 hours, and 49+ hours) was performed. Pairs with both NP and NS specimens having viruses detected or the same virus(es) detected were considered completely concordant. Specimens with multiple viruses detected on NP swab but only a single virus detected on NS swab, or vice versa, were considered partially concordant. Specimens with one virus detected on NS or NP and none detected on its pair were considered discordant. Results: One hundred and forty-seven pairs, each including one NP and one NS specimen, were obtained. Of the 147 pairs, 114 (77.5%) had complete concordance – 86 (58.5%) had viruses detected and 28 (19%) had no viruses detected. Fourteen (9.5%) pairs were partially concordant, and 19 (13%) were discordant. Sensitivity of NS specimens collected within 48 hours of their NP pair was ≥80% for all viruses except seasonal coronavirus (sensitivity 42.9%) (Table 1). NS specimens for adenovirus, influenza, parainfluenza, RSV, and SARS-CoV-2 were 100% sensitive when collected within 24 hours of NP specimens. Conclusion: Overall, NS are a potential alternative method for respiratory virus detection in the pediatric population. This less invasive collection method allows for broader use outside of medical settings, including respiratory virus surveillance in community settings. Future studies with closely time-matched NS and NP collection are needed to evaluate individual virus type detections.
-

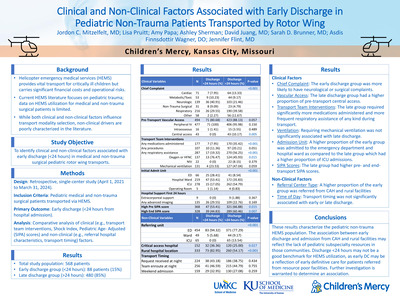
A Case of Heterotaxy and Common Atrioventricular Canal with Bradycardia
Mohamed Aashiq Abdul Ghayum, Jenna Schermerhorn, Hayley S. Hancock, Kelsey Brattrud, Melanie Kathol, and Maria Kiaffas
Background: Heterotaxy-polysplenia syndrome (otherwise known as left atrial isomerism) should be suspected in the presence of complete atrioventricular canal defect (CAVC) with interruption of the inferior vena cava (IVC), atrioventricular block (AVB), and viscero-cardiac heterotaxy. The prognosis remains dismal for the fetus with such entity, especially in the presence of major structural heart disease and high-grade atrioventricular block. Early diagnosis, close follow up, and appropriate delivery planning, allows for effective stabilization of the baby after birth and might improve survival. Methods: A 26-year-old mother at 26 weeks gestational age was referred for cardiac evaluation of cardiomegaly, suspected CAVC and bradycardia. Maternal SSA and SSB antibodies were negative. Fetal echocardiogram showed moderate cardiomegaly, bradycardia with 3° AVB with ventricular rate of 64 beats per minute. Anatomy was consistent with heterotaxy {S/A,D,S}, hypoplastic left atrioventricular valve, unbalanced, right-dominant CAVC, dysplastic pulmonary valve, interrupted IVC with azygous continuation to a persistent left superior vena cava draining to a dilated coronary sinus. Partial anomalous pulmonary venous connection and coarctation of the aorta were suspected. Biventricular function was low normal with ventricular non-compaction. Ductus venosus Doppler was notable for a-wave reversal. Umbilical artery and middle cerebral artery waveforms were normal. Biweekly follow-up revealed worsening extracardiac Dopplers and decreasing ventricular function. Results: Given the prematurity, bradycardia, complex cardiac anatomy, non-compaction and ventricular dysfunction, prognosis was considered unfavorable. An integrated consult involving fetal cardiology, neonatology, Electrophysiology (EP) and Palliative care teams was undertaken. The family was counseled for guarded prognosis and high risk for demise, need for postnatal permanent pacemaker and surgical repair leading to a single ventricle pathway with possibility for heart transplant. A 2.79 kg female was delivered by c-section at 35 weeks 5 days; Apgar score was 4,4,and 8. The newborn was immediately transferred for placement of temporary pacing wires with subsequent transfer to the cardiac intensive care unit for stabilization and further management. Coarctation repair, PDA ligation and permanent pacemaker placement were performed at 4 weeks of age. Progressive biventricular dysfunction, bilateral outflow tract obstruction and pacemaker dependency resulted in transplant listing of the patient with a successful orthotopic heart transplantation taking place at 4 months of life and has continued to do well on follow up. Conclusions: Heterotaxy polysplenia syndrome should be suspected in cases with CAVC with interruption of the IVC, and AVB. The presence of major structural heart disease and high-grade AV block carries a guarded prognosis, with survival to discharge from the hospital after delivery at term or near term reported to be less than 50%; in cases of prematurity, survival is expected to be even lower. In our patient, early diagnosis, appropriate counseling, close follow-up and meticulous delivery planning allowed successful perinatal stabilization with timely pacing and effective supportive management. Timely listing and eventual heart transplantation resulted in the survival of this patient.
-

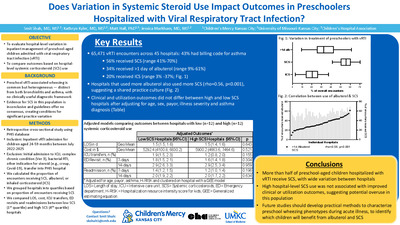
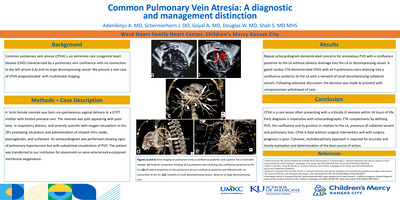
Common Pulmonary Vein Atresia: A Diagnostic and Management Distinction
Adenike Adenikinju, Jenna Schermerhorn, Anmol Goyal, William Douglas, and Sanket Shah
Common pulmonary vein atresia (CPVA) is an extremely rare congenital heart disease (CHD) characterized by a pulmonary vein confluence with no connection to the left atrium (LA) and no large decompressing vessel. We present a rare case of CPVA prognosticated with multimodal imaging.
-

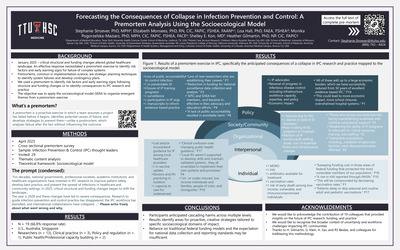
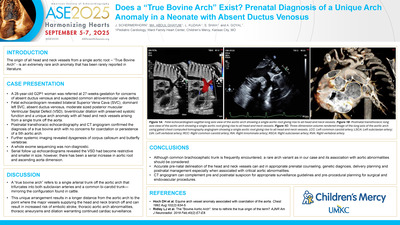
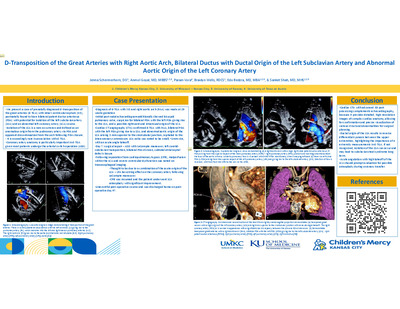
D-Transposition of the Great Arteries with Right Aortic Arch, Bilateral Ductus with Ductal Origin of the Left Subclavian Artery and Abnormal Aortic Origin of the Left Coronary Artery
Jenna Schermerhorn, Anmol Goyal, Param Vora, Braidyn Wells, Edo Bedzra, and Sanket Shah
We present a case of prenatally diagnosed d-transposition of the great arteries (d-TGA) with intact ventricular septum (IVS), postnatally found to have bilateral patent ductus arteriosus (PDA) with potential for isolation of the left subclavian artery (LSA) and an abnormal left coronary artery (LCA) course. Isolation of the LSA is a rare occurrence and defined as an anomalous origin from the pulmonary artery via PDA and apparent discontinuation from the arch following PDA closure. It is exceedingly rare in association with d-TGA. Coronary artery anatomy is particularly important in d-TGA given most patients undergo the arterial switch operation (ASO).
-

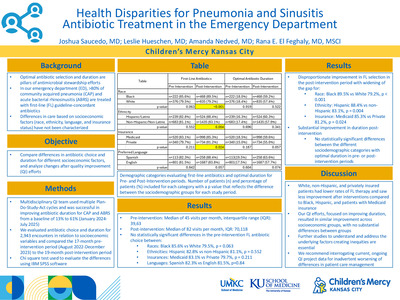
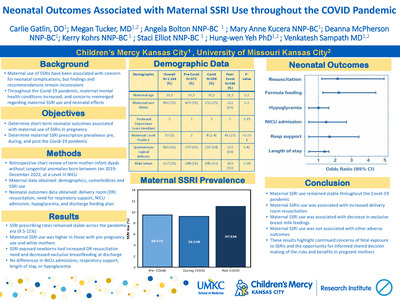
Duration of Labor and Umbilical Artery Acidosis in Critical Congenital Heart Disease
Sarah Gwazdacz, Teresa Nguyen, Henry Yeh, Mary T. Donofrio, Timothy Bennett, and Amanda McIntosh
• Background (83 words): Standard delivery protocols for most prenatally diagnosed CCHD is induction of labor at 39 weeks with aims of a vaginal delivery (VD) near a tertiary care center. There is no benefit to planned Cesarean delivery (CD) over VD for most infants with CCHD. However, longer durations of labor (DOL) in CCHD have been described as a risk factor for umbilical artery (UA) acidosis. We aim to describe the relationship between DOL and UA pH and neonatal outcomes in those with prenatally diagnosed CCHD. • Methods (150 words): Retrospective chart review of prenatally diagnosed with CCHD born at Children’s Mercy from 2012 – 2023. Inclusion criteria was CCHD defined as anticipated neonatal intervention or prostaglandin dependence, single ventricle (SV) circulation, or risk of hemodynamic instability with placental separation. Excluded fetal demise, multiple gestations, prematurity, post-maturity, and comfort cares. Divided subjects into 3 groups: those who had VD, CD after a trial of labor (TOL), or CD without a TOL. The primary outcome was UA pH. Secondary outcomes were delivery room intubation, perinatal brain injury, and peak lactate, cardiac arrest, death, or inotropic support in the first 24 hours of life. Collected demographic and clinical information for the maternal-fetal dyad. Divided CCHD diagnoses into 4 groups based on SV versus biventricular anatomy and the presence of systemic outflow obstruction. Welch 2-sample test or ANOVA were used for inter-group comparisons. For associations, multivariable linear regression modeling was performed. • Results: (150 words) Analyzed 201 VD, 32 CD after a TOL, and 90 scheduled CD without a TOL patients. Between the groups, there was no difference in birth weight (BW), gestational age (GA), intrauterine growth restriction (IUGR), and UA pH. Mothers with planned CD were older and delivered fetuses with higher rates of genetic syndromes. On univariate analysis, DOL in VD group was associated with lower UA pH (estimate -0.0006707 (95% CI: [-0.00130, -0.00005], P-value: 0.037). This remained significant on multivariable analysis controlling for GA, BW, hydrops, genetic syndromes, and IUGR (P-value = 0.011). Looking at CCHD subgroups, DOL and UA pH only had a significant association in neonates with SV anatomy and systemic obstruction (P-value= 0.009). DOL and lactate had a significant relationship on univariate (estimate 0.01479 (95% CI: [0.00307,0.02651], P-value= 0.014) and multivariate analysis (p-value = 0.015). There was not a significant relationship between DOL and other secondary outcomes. • Conclusion (51 words) In this single center retrospective study of fetuses with CCHD, longer duration of labor was associated with higher neonatal lactate levels. It was associated with lower UA pH in neonates with single ventricle anatomy and systemic obstruction. This may be a modifiable risk factor in certain subsets of prenatally diagnosed CCHD.
-

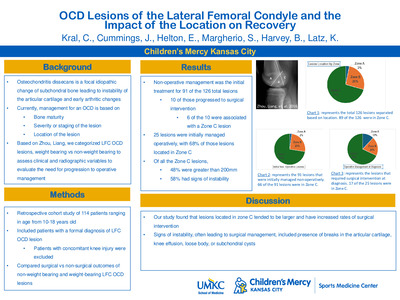
OCD Lesions of the Lateral Femoral Condyle and the Impact of the Location on Recovery
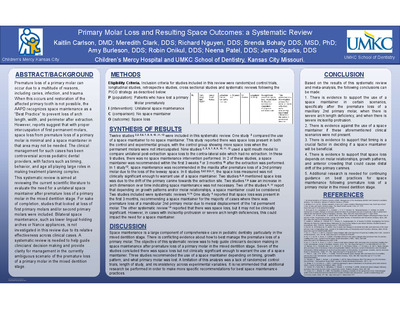
Catharine Kral, Joshua Cummings, Ellie Helton, Shannon Margherio, Brian S. Harvey, and Kevin Latz
Descriptive study based on Zhou, Liang, et al. we categorized the LFC OCD lesions into weight bearing and non-weight bearing lesions to assess clinical and radiographic variables and evaluate the need for progression to operative management.
-

Discrepancy Between Hyaluronic Acid Levels And Mri-Based Measurements Of Hepatic Fat And Fibrosis
Daniel Aaron Borman, Rachel Chevalier, Jonathan Wagner, Michele T. Pritchard, Sherwin S. Chan, Nathan S. Artz, Johnston Fite, Yoon Cho, Valentina Shakhnovich, Veronica Williams, and Voytek Slowik
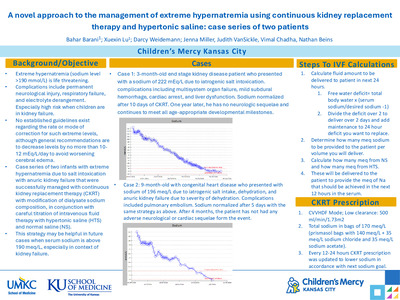
Introduction Metabolic-dysfunction-associated steatotic liver disease (MASLD) is the most common liver disease in children in the United States and, when left untreated, can progress to liver fibrosis. Clinicians currently utilize imaging and biopsy to assess fibrosis in this patient population as there is no validated serum biomarker available for detecting fibrosis. Previous research suggests that serum hyaluronic acid levels are predictive of hepatic fibrosis in children with MASLD. Methods Retrospective data were obtained from the Children’s Mercy Hospital Liver Lab study. Pediatric subjects with both hyaluronic acid (HA) samples and MRI evaluation within a month were identified and included for evaluation. Hyaluronic acid was evaluated via an ELISA-like assay. Measurements of hepatic fat fraction (HFF) and elastography were obtained via averaged MRI region of interest evaluation . SPSS software was utilized to assess correlation between anthropometric measurements, hyaluronic acid, and MRI data, including both HFF and elastography. Results A total of 59 patients with 98 unique data points were identified for analysis. Moderate correlations were found between BMI z-score and HFF (r=0.36, p=0.002) and elastography (r=0.47, p<0.001). No statistically significant correlation was identified between HA and BMI z-score (r=-0.09, p=0.348), HFF (r=-0.05, p=0.633), or elastography (r=-0.20, p=0.051). Conclusion In contrast to previous literature, this study did not demonstrate a statistically significant correlation between hyaluronic acid levels and MRI-based measurements of hepatic fat or fibrosis. Further research is needed to identify biochemical markers to predict fibrosis in children with MASLD.
-

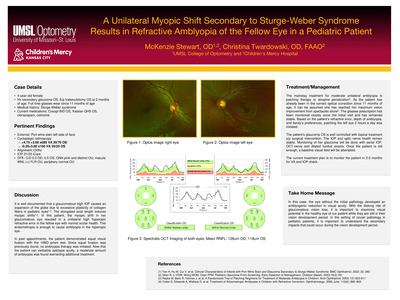
A Unilateral Myopic Shift Secondary to Sturge-Weber Syndrome Results in Refractive Amblyopia of the Fellow Eye in a Pediatric Patient
McKenzie Stewart and Christina Twardowski
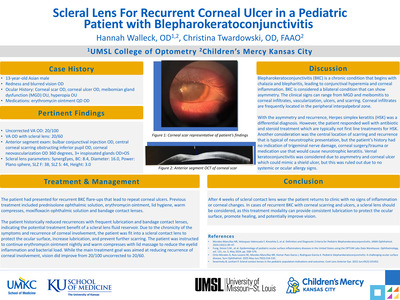
A 4-year-old patient with unilateral glaucoma secondary to Sturge-Weber Syndrome causes a myopic shift. The fellow healthy eye maintains high hyperopia resulting in anisometropic refractive amblyopia, requiring occlusion therapy. It is well documented that a glaucomatous high IOP causes an expansion of the globe due to excessive plasticity of collagen fibers in pediatric eyes. The elongated axial length induces myopic shifts. In this patient, the myopic shift in her glaucomatous eye resulted in a unilateral high hyperopic refractive error in the fellow eye with normal ocular health. This anisometropia is enough to cause amblyopia in the hyperopic eye. In past appointments, the patient demonstrated equal visual fixation with the 10BD prism test. Since equal fixation was previously found, no amblyopia therapy was initiated. Now that the patient can verbalize optotype acuity, a moderate amount of amblyopia was found warranting additional treatment. The mainstay treatment for moderate unilateral amblyopia is patching therapy or atropine penalization. As the patient has already been in the correct optical correction since 11 months of age, it can be assumed she has reached her maximum vision improvement from spectacles alone. The glasses prescription has been monitored closely since the initial visit and has remained stable. Based on the patient’s refractive error, depth of amblyopia, and family’s preferences, patching the left eye 2 hours a day was initiated. In this case, the eye without the initial pathology developed an amblyogenic reduction in visual acuity. With the lifelong risk of glaucomatous vision loss, it is important to maximize visual potential in the healthy eye of our patient while they are still in their vision development period. In the setting of ocular pathology in pediatric patients, it is important to understand the secondary impacts that could occur during the vision development period.
-

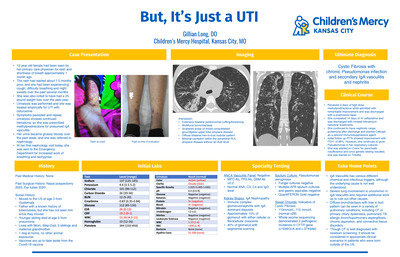
But, It's Just a UTI
Gillian Long
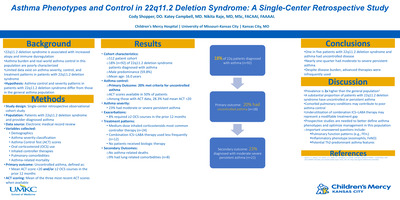
IgA Vasculitis is a commonly seen presentation in the pediatric population. The constellation of symptoms typically includes purpuric rash, joint pain, abdominal pain and hematuria. This 12 year old female was seen by her pediatrician for rash on her legs, shortness of breath, cough and night sweats that all started around 2 months ago. Additionally, a 25 pound weight loss was noted over the past year. The rash appeared as nonblanching purpura on her lower extremities, lending suspicion to IgA Vasculitis. She was first treated for UTI with cefuroxime, and then treated with steroids. Urinalysis showed persistent hematuria and she was referred to nephrology. At her first visit, she was sent to the Emergency Department for tachypnea and increased work of breathing. Baseline labs showed normal electrolytes and kidney function, elevated inflammatory markers (CRP of 19.1 and ESR of 26), and mild leukocytosis. Urinalysis showed 3+ blood and 3+ protein. Chest CT demonstrated extensive bilateral peribronchial cuffing, multifocal bronchiectasis, scattered upper lobe airspace disease, and a diffuse treein-bud nodular pattern. Initial differential included vasculitis, disseminated tuberculosis or fungal infection, or primary pulmonary disease. Ultimately, multiple specialty services were consulted. Rheumatology workup included ANCA vasculitis panel, ANA, C3, C4 and IgG levels, all negative. Nephrology obtained a kidney biopsy, which was consistent with IgA Nephropathy. Infectious Diseases requested multiple AFB sputum cultures and gastric aspirates, along with Quantiferon Gold and Fungal cultures, with the only positive finding being Pseudomonas aeruginosa growth in the sputum. Lastly, Pulmonology recommended sweat chloride tests, both positive; so whole exome sequencing was obtained and showed 2 pathogenic mutations in the CFTR gene, confirming a diagnosis of cystic fibrosis. The final diagnosis was Cystic Fibrosis with chronic Pseudomonas infection and secondary IgA vasculitis and Trikafta. Her PFTs continue to improve and she has not re quired readmission to the hospital since the nephritis. She was treated with pulse steroids, IV antibiotics and eventually started on Cellcept and diagnosis was made. While this patient did have a secondary IgA Vasculitis, not all of her symptoms were typical. Severe lung involvement is uncommon in IgA Vasculitis and requires additional workup. Additionally, while cystic fibrosis is well diagnosed with newborn screening, it should be considered in appropriate clinical scenarios when newborn screening was not obtained.
-

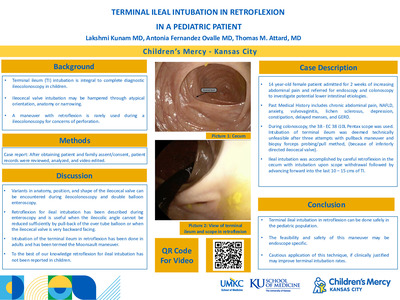
Terminal Ileal Intubation In Retroflexion In A Pediatric Patient
Lakshmi Kunam, Antonia Fernandez Ovalle, and Thomas M. Attard
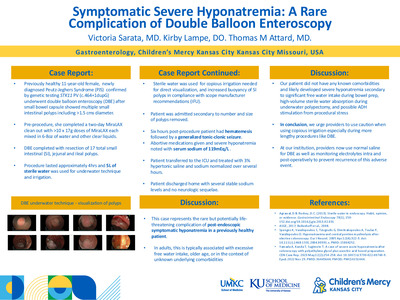
Background: Terminal ileum (TI) intubation is integral to complete diagnostic ileocolonoscopy in children. It is necessary to determine terminal ileal involvement in patients with a broad spectrum of pathologic processes. In some cases the standard method of intubation does not lead to success and retroflexion is needed. Here we describe the case of terminal ileal intubation in retroflexion on a 14 year old female. Case description: 14 year-old female patient with a past medical history of chronic abdominal pain, NAFLD, anxiety, vulvovaginitis, lichen sclerosus, depression, constipation, delayed menses, and GERD who was admitted for 2 weeks of escalating symptoms and referred for endoscopy and colonoscopy to investigate potential lower intestinal etiologies. During colonoscopy, the 38 - EC 38 i10L Pentax scope was used. Intubation of terminal ileum was therefore necessary for completeness of exam but was deemed technically unfeasible after three attempts with pullback maneuver (because of inferiorly directed ileocecal valve). Ileal intubation was accomplished by careful retroflexion in the cecum with intubation upon scope withdrawal followed by advancing forward into the last 10 – 15 cms of TI. Discussion: Retroflexion for ileal intubation has been described during double balloon Enteroscopy and is useful when the ileocolic angle cannot be reduced sufficiently by pull-back of the overtube balloon or when the ileocecal valve is very backward facing. These issues with anatomy, position, and shape of the ileocecal valve are present during ileocolonoscopy as well. However, a maneuver with retroflexion is rarely used for concerns of perforation. Intubation of the terminal ileum in retroflexion has been done in adults and has been termed the Moonsault manuevar. To the best of our knowledge retroflexion for ileal intubation has not been documented in children. Conclusion: Our experience demonstrates that terminal ileal intubation in retroflexion can be done safely in the pediatric population. Assessing the outcomes of this in other similar patients will assist in determination of further guidelines of this maneuver and optimal patients for safe execution of this maneuver.
-

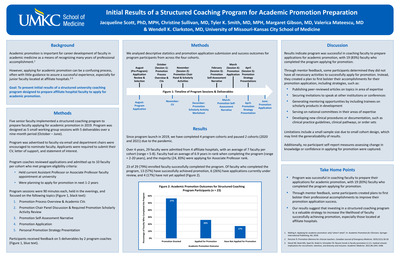
Variation in Provider Specialization among 139 Non-affiliated Real-World Data Contributors
Joshua Koni, Rose Reynolds, Janelle R. Noel-Macdonnell, and Mark A. Hoffman
Oracle EHR Real-World Data (OERWD) is a national de-identified data set useful for observational findings across 139 non-affiliated healthcare systems. Data in OERWD is associated with a de-identified provider ID categorized and documented using National Uniform Claim Committee (NUCC) taxonomy codes. There are 2,421,948 providers in OERWD associated with both their specialty and contributing organization. We profile the data for overall distribution and co-occurrence of specialties, enabling research related to treatment patterns and outcomes.
-
 For A Boy With Ipex Syndrome by Ali H. Alnajim and Salman Aljubran")
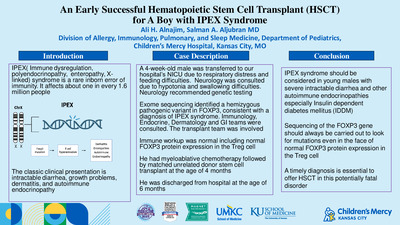
An Early Successful Hematopoietic Stem Cell Transplant (Hsct) For A Boy With Ipex Syndrome
Ali H. Alnajim and Salman Aljubran
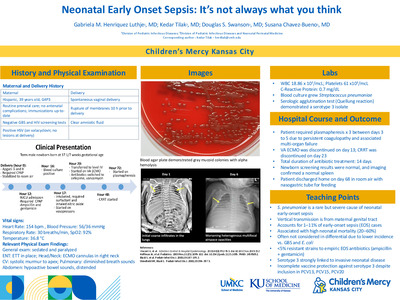
Immune dysregulation, polyendocrinopathy, enteropathy, X-linked (IPEX) syndrome is a rare inborn error of immunity. It affects about one in every 1.6 million people. It is caused by mutations in the forkhead box P3 (FOXP3) gene on chromosome Xp11.23. FOXP3 is a vital regulator of T cell development and function. Dysfunctional FOXP3 allows the hyperactivation of T cells, resulting in skin rash, enteropathy, diabetes, thyroiditis, hemolytic anemia, and thrombocytopenia. The classic clinical presentation is intractable diarrhea, growth problems, dermatitis, and autoimmune endocrinopathy. Case Description: A 4-week-old male was transferred to our hospital’s NICU due to respiratory distress and feeding difficulties. Neurology was consulted due to hypotonia and swallowing difficulties. Neurology recommended genetic testing. Exome sequencing identified a hemizygous pathogenic variant in FOXP3, consistent with a diagnosis of IPEX syndrome. Immunology, Endocrine, Dermatology and GI teams were consulted. The transplant team was involved. Immune workup was normal including normal FOXP3 protein expression in the Treg cell. He had myeloablative chemotherapy followed by matched unrelated donor stem cell transplant at the age of 4 months. He was discharged from hospital at the age of 6 months. Discussion: IPEX syndrome should be considered in young males with severe intractable diarrhea and other autoimmune endocrinopathies especially Insulin dependent diabetes mellitus (IDDM). Sequencing of the FOXP3 gene should always be carried out to look for mutations even in the face of normal FOXP3 protein expression in the Treg cell. A timely diagnosis is essential to offer HSCT in this potentially fatal disorder.
-

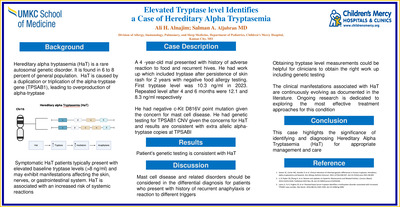
Elevated Tryptase Level Identifies A Case Of Hereditary Alpha Tryptasemia
Ali H. Alnajim and Salman Aljubran
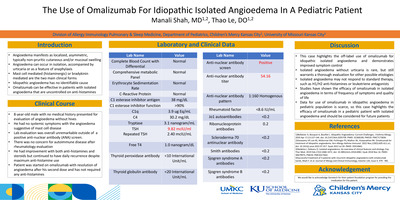
Introduction Hereditary alpha tryptasemia (HaT) is a rare genetic disorder characterized by elevated serum tryptase levels due to duplication or triplication of the TPSAB1 gene. Affecting 6 to 8 percent of the population, HaT presents with diverse symptoms, including idiopathic anaphylaxis, skin rashes, and gastrointestinal issues. This report highlights a case that underscores the complexities and diagnostic challenges of HaT. Case Description A 4-year-old male presented with recurrent skin rashes and gastrointestinal symptoms following ingestion of certain foods, despite negative allergy tests. Persistent symptoms led to further investigations, revealing elevated tryptase levels of 10.3 ng/ml, 12.1 ng/ml, and 8.3 ng/ml over several months. The c-Kit D816V mutation test was negative, prompting genetic testing for TPSAB1 CNV, which confirmed HaT. Discussion The diagnosis of HaT in this patient illustrates the need for a comprehensive diagnostic approach in individuals with recurrent anaphylaxis and unexplained allergic reactions. Elevated tryptase levels served as a crucial biomarker, guiding genetic testing and confirming HaT. This case highlights the importance of early identification and management of HaT to prevent severe systemic reactions. As clinical understanding of HaT evolves, integrating genetic testing into routine practice will enhance diagnostic accuracy and patient care.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}