
These posters have been presented at meetings in Children's Mercy and around the world. They represent research that was done at the time they were created, and may not represent medical knowledge or practice as it exists at the time viewers access these posters.
-

Investigating the Association between Mast Cell Activation Syndrome and Irritable Bowel Syndrome
Ishaan Jakhar, Maggie Urschler, Medha Singh, Suman Sahil, and Hassan Ahmad
Investigating the Association between Mast Cell Activation Syndrome and Irritable Bowel Syndrome Introduction Mast Cell Activation Syndrome (MCAS) involves the inappropriate release of chemical mediators resulting in varied episodic symptoms. Irritable Bowel Syndrome (IBS) is a common functional abdominal disorder where mucosal immune alterations play a key role. Since mast cells function as gatekeepers for the intestinal interface, we examined what proportion of patients diagnosed with MCAS also had IBS along with comorbid risk factors. Methods All patients in our study were 18 years of age or older. We used Cerner Healthfacts to gather our cohorts of patients with MCAS, IBS. We examined potential comorbid risk factors for MCAS using multivariable regression. Results We identified 2,508 patients with MCAS, mean age of48.7 ± 17.7 years with 67.7% (1,698) being female. 79.9% (2,003) were Caucasian, 8.3% (209) were African American. 11.5% (288/2,508) of patients with MCAS had IBS as well. The most common comorbid autoimmune disorder (AiD) was autoimmune thyroid disease (220). On multivariable regression, the factors associated with a higher risk of IBS in those with MCAS included cholestatic liver disease (OR 9.95), depression (OR 2.03), anxiety (OR 1.73), female gender (OR 1.64), autoimmune disorders (OR 1.63), and asthma (OR 1.56). Conclusions MCAS and IBS have symptom overlap with diarrhea and abdominal cramping. 11.48% of MCAS patients had IBS, indicating it may be worthwhile to inquire about bowel habits. Clinicians should also consider autoimmune thyroid disease in MCAS patients. There may be merit in exploring IBS therapies for MCAS patients.
-

Privacy preserving self-service DeGAUSS Based Geomarker Portal
Harpreet Gill, Kushal Vallambhatla, Mark A. Hoffman, Kevin Power, and Catherine Jackson
DeGAUSS offers a privacy-preserving capability to annotate a list of addresses with geomarker information that is useful for social determinants and other research. The standard delivery of DeGAUSS requires command line proficiency, potentially limiting the group of users. We provide a self-service portal that enables researchers to load a file and receive a downloadable annotated output file. In our pilot phase, the system has processed 481 calls for more than 45,000 addresses at Children’s Mercy.
-

Understanding Macrophage Phagocytosis in Pediatric Leukemia
Molly Leyda, Jacqelyn Nemechek, John Szarejko, Fang Tao, Tykeem Manor, Douglas Myers, and John M. Perry
Macrophages are a diverse and widespread type of innate immune cell which play an important role in homeostasis and defense. In a process called phagocytosis, macrophages engulf dying cells, foreign substances, and pathogens. Importantly, macrophages can present antigens from phagocytosed cells allowing them to initiate an adaptive immune response against remaining cells of the same type. Despite the immunosuppressive nature of the tumor microenvironment, macrophages often infiltrate tumors where they can either promote or inhibit cancer development, though the specific conditions influencing their pro- vs anti-cancer activity remain enigmatic. Recently, macrophages have been brought into the spotlight of immunotherapy research due to the hope of harnessing their ability to migrate into tumors, phagocytose cancer cells, and mobilize an antitumor T-cell response. However, questions remain about how macrophages recognize, or fail to recognize, cancerous cells for clearance, and how they can promote vs inhibit tumor progression. To identify modulators of macrophage activation, we have developed a model to visualize and quantify phagocytosis. In this model, bone marrow-derived macrophages are stained with CMFDA, a green cell tracker dye. Cancer cells are stained with pHrodo red, a pH sensitive fluorogenic probe which is designed to fluoresce brighter when inside the acidic phagosome, indicating phagocytosis has occurred. Macrophages are co-cultured with the cancerous target cells then imaged and analyzed. Phagocytosed cells can be visualized through fluorescence microscopy and the number of fluorescent engulfed cells quantified with flow cytometry. This in vitro model allows us to test how macrophages differentially engulf target cells based on various conditions such as macrophage polarization state or cancer cell phenotype. Data acquired from these experiments helps us delineate which characteristics of cancer cells are recognized by macrophages allowing us to better understand the role of phagocytosis in cancer. Future studies will test modified macrophage states in our tumor models and determine how polarization can be exploited to alter the spectrum of pro- and anti-cancer macrophage activities.
-

Candida Chorioretinitis in Immunocompromised Patient with Candida Tropicalis Fungemia Secondary to Chemotherapy
Jourdan Valkner Krause
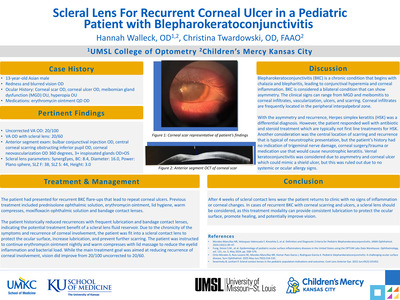
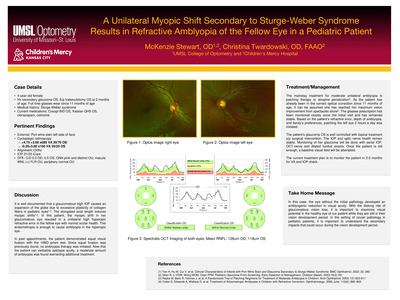
Summary: An immunocompromised patient with candida tropicalis fungemia secondary to chemotherapy presented for follow up of candida chorioretinitis. This infection puts the patient at high risk for CNVM formation and must be followed closely. Case History: • 3-year-old Hispanic female • CC: Candida chorioretinitis follow up • POH: Bilateral orbital chloromas and optic nerve atrophy • PMH: Acute myeloid leukemia, Candida tropicalis fungemia • Meds: o Amphotericin B liposomal 85 mg 42.5 mL, IV, q24hr o Flucytosine 500 mg Capsule *NF* 1,000 mg 2 capsule, PO/NG, q6hr o Micafungin 100 mg 100 mL, IV, q24hr *Plus numerous chemotherapy, pain and other systemic medications. Pertinent Findings: •Clinical: o DFE: One small, <1/2 disc diameter, white lesion inferior to macula OD. Slightly elevated with pigmented borders • Physical: o Immunocompromised • Laboratory testing: o Culture confirmation of Candida tropicalis fungemia o MRI: innumerable foci of nodular and ringlike contrast enhancement involving the brain, brainstem, and cerebellum most compatible with CNS dissemination of fungal disease. There is additional dissemination of fungal disease with involvement of the orbits and scalp. The presence of restricted diffusion within the rim-enhancing collection of the right orbit as described on the CT examination is most compatible with an abscess. Differential Diagnosis: • Toxoplasmosis • White dot syndrome • Cotton wool spot • Retinal tuft Diagnosis Discussion: Immunocompromised patients are susceptible to life threatening infections that are otherwise rare in the immunonormal. With any concern for infection, a thorough work up is needed to initiate proper treatment quickly. In this patient, cultures were positive for Candida tropicalis fungemia. Amphotericin B, micafungin and flucytosine were started. A baseline eye exam was performed and bilateral candida chorioretinitis was diagnosed. Two lesions near the macula OD and one lesion in the periphery OS were observed. After continuous antifungal treatment, only one lesion with pigmented edges remained near the macula OD and no lesions OS at 1 month follow up. With no additional signs to suggest active infection, pigmentation around the remaining lesion led to diagnosis of inactive candida chorioretinitis. Treatment/Management Discussion: Although the infection appears to be inactive, it is crucial to follow this patient every 6 weeks while the patient remains immunocompromised due to high risk of reactivation. There is also risk of CNVM formation. With the lesion’s close proximity to the macula, this must be carefully monitored with DFE and fundus imaging at every 6 week exam. In addition, it is anticipated the reflex seen during retinoscopy will be altered if changes to the macula occur. Alteration in the reflex would be an additional sign leading to the assumption the disease has progressed. The patient should continue taking systemic antifungals as prescribed by infectious disease team until instructed otherwise. Due to this patient’s young age, and still being within the visual development period, it is important to monitor for amblyopia since the lesion resides within the macula. With the patient having equal 20/50 acuity OD and OS, no amblyopia treatment is indicated at this time, but will be closely watched. Conclusion: Immunocompromised patients are predisposed to life threatening infections. In individuals with a history of infection, it is imperative to follow them closely, no matter if the infection is active or inactive. This group is at a higher risk of reactivation, thus should be monitored until the immune system recovers. In patient’s with any form of chorioretinitis, there is a risk of CNVM formation, even once immunonormal. Careful DFE and imaging should be performed at every follow up.
-

Dexamethasone for BPD while on Non-invasive positive pressure ventilation
Priya Tiwari, Jansynn Radford, Michael Norberg, and Alain Cuna
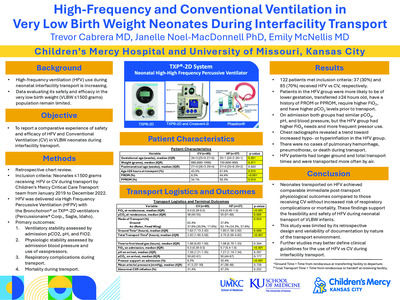
Background: Postnatal dexamethasone (DEX) has traditionally been reserved for preterm infants on prolonged mechanical ventilation, with reported rates of successful extubation at 47% to 76%. Recent emphasis on avoiding mechanical ventilation has resulted in preterm infants being increasingly supported with chronic non-invasive ventilation (NIV). The use of DEX for weaning preterm infants on chronic NIV remains largely unexplored. Objective: To determine efficacy of postnatal DEX in weaning infants on chronic NIV, and to identify factors and outcomes associated with successful weaning. Methods: Single-center retrospective study (2010-2022) of preterm infants ≤32 weeks gestation treated with postnatal DEX while on chronic NIV. Data on baseline demographics, respiratory characteristics at start and end of treatment, and clinical outcomes were collected. Primary outcome was rate of successful weaning from NIV to high-flow nasal cannula (HFNC). Other outcomes included factors and outcomes associated with successful weaning. Results: A total of 56 infants (mean gestational age 26 weeks, mean birth weight 890 grams) received postnatal DEX while on NIV. The average postnatal day and postmenstrual age at time of treatment were 78 days and 37 weeks, respectively. DEX treatment resulted in a significant decrease in oxygen and ventilation support from baseline to end of treatment (Fig 1). Overall, the rate of successful weaning to HFNC was 46% (26/56). Infants treated with postnatal DEX for the first time had similar rates of successful weaning compared to infants who had received prior DEX treatment (43% vs 39%, P =0.79). Factors associated with successful weaning to HFNC were earlier age and lower NIV and oxygen support at time of DEX treatment (Table 1). Infants with successful weaning were more likely to be discharged earlier with less bronchopulmonary dysplasia and less retinopathy of prematurity compared to infants with unsuccessful weaning (Table 2). Other complications of prematurity were similar between the two groups (Table 2). Conclusion: In our level IV NICU, efficacy of postnatal DEX to wean infants on chronic NIV was 46%. Our results suggest that DEX may also be useful in infants on chronic NIV, but further studies are needed to fully determine efficacy and safety.
-

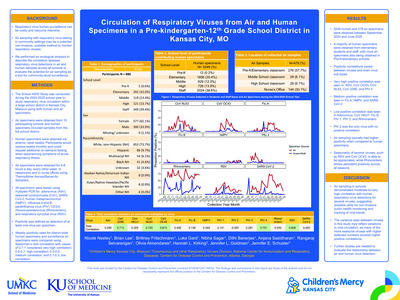
Factors associated with respiratory pathogen panel utilization in children hospitalized with acute respiratory illness — New Vaccine Surveillance Network, Kansas City, 2017–2021
Edward Lyon, Brian R. Lee, Benjamin Clopper, Heidi L. Moline, Rangaraj Selvarangan, and Jennifer Schuster
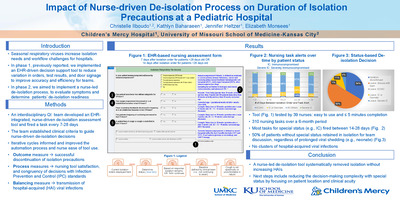
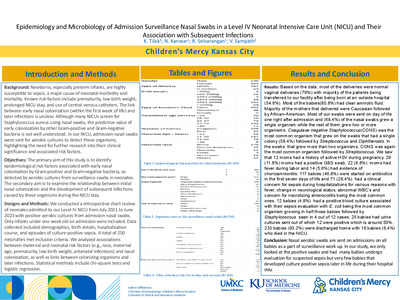
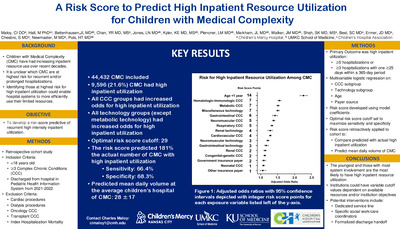
Background: Respiratory pathogen panels (RPP) are multiplex PCR platforms that detect several respiratory viruses from one specimen. For most children hospitalized with acute respiratory illness (ARI), management is supportive, and detection of a specific virus from RPP does not impact clinical care. Therefore, clinical RPP use is not standardized, and ordering is at the discretion of the clinician. We sought to understand factors associated with RPP utilization among pediatric patients hospitalized with ARI. Methods: From October 2017 to September 2021, participants < 18 years hospitalized with ARI were enrolled at a single site in the New Vaccine Surveillance Network (NVSN). Eligible patients were residents of Jackson County, MO, had one or more ARI symptoms (e.g., cough, fever, nasal congestion) lasting < 14 days, and were enrolled within 48 hours of admission. Parent interviews and medical chart reviews were conducted. All participants had a research RPP, but results were not available to the clinical providers. Clinical providers were able to order a clinical RPP (cRPP), for which they received test results. Characteristics of NVSN enrollees hospitalized with ARI with and without a cRPP are described. Lastly, medical complexity was assessed via the pediatric complex chronic conditions classification system (CCC) then analyzed via chi- square test between groups. Findings: During the study period, 1,038 participants were enrolled, and 555 (53.4%) received a cRPP. Most, 299 (53%), cRPPs were ordered in the emergency department or urgent care before admission. Age was a significant factor associated with cRPP use (Table 1). cRPP participants were more likely to have complex chronic conditions, and/or technology dependence. No difference in cRPP use was observed by race/ethnicity, payer status, or sex. More participants were enrolled in 2020-2021, but the overall usage of cRPP is similar between years (Table 2). Conclusions: In this large cohort of children hospitalized with ARI, medical complexity, technological dependence, and age < 2 months were associated with increased utilization of cRPPs. Understanding the impact of cRPP on clinical care requires further investigation to better understand the utility of these tests.
-

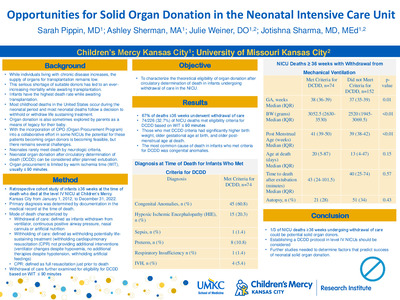
Impact of Fetal Health Center on Mode of Neonatal Death
Erin Bolen, Ashley Sherman, Julie Weiner, and Jotishna Sharma
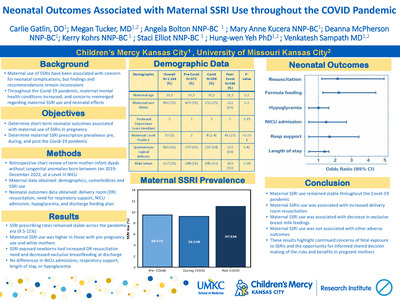
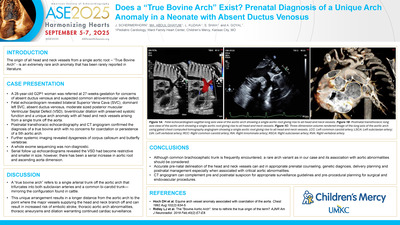
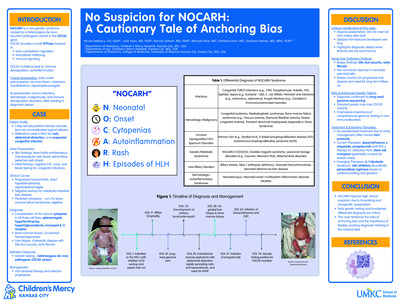
Introduction There has been significant innovation and technological advancement in prenatal diagnosis, fetal therapeutic intervention, and establishment of fetal health centers (FHC) at children’s hospitals with dedicated delivery services for high-risk neonates and expedited access to level IV neonatal intensive care units (NICU). Morality trends have been examined on individual bases and within diagnostic groups, but there have been few studies that examine overall modes of mortality in the NICU population across diagnoses after the implementation of a dedicated FHC. This study aims to compare modes of death at a level IV children’s hospital NICU between infants born at the fetal health center (inborn) and those transferred from referral centers (outborn). Study Design/Methods Patients who died at the Children’s Mercy Hospital NICU from January 2012-December 2022 were identified. FHC deliveries started in 2011. Via retrospective chart review, data were collected on place of birth and mode of death (CPR within six hours of death, withholding of potential interventions, or withdrawal of existing interventions). Results were evaluated with a 2-tailed z test. Further analysis will be undertaken. Results Over the 10-year study period, there were 10,862 admissions and 563 (5.2%) deaths. Of the deaths, 35.6% were inborn and 64.5% outborn. Of total admissions, 1,857 (17%) were inborn with 200 (10.7%) deaths. Outborn infants accounted for 9,005 admissions with 363 (4%) deaths. Data were available for 561 deaths, including all inborn deaths. Figures 1 (inborn) and 2 (outborn) show modes of death by year as a percentage. Modes of death were compared based on place of birth in Figure 3. Differences for withdrawal and withholding of interventions between outborn and inborn infants were significant with p=<0.00001 while the difference for receiving CPR approached but did not reach significance with p=0.073. Discussion The data demonstrate a significant difference in the percentage of withdrawal of intervention and withholding of intervention as the primary mode of death between inborn and outborn infants. This could be secondary to initial stabilization at outside hospitals prior to transport or indicate differences in the underlying diagnoses. This could also be secondary to inborn births receiving extensive prenatal counselling at the FHC with a do not resuscitate (DNR) at birth or limited intervention plan already in place. Further analyses based on diagnoses and type of birth plan will be undertaken. The presence of immediate post-natal withholding of care will be further evaluated with multivariate analysis based on age of death. Year-by-year data also demonstrates a trend of increased rates of CPR prior to death in the outborn group. FHC programs focus on congenital abnormalities that are amenable to prenatal diagnosis which may lead to an overrepresentation of devastating congenital abnormalities in this group. Further multivariate analysis will be undertaken to assess if this or other variables may be responsible for the differences in modes of death between populations. Conclusion Inborn newborns born at a fetal health center had a higher mortality compared to outborn infants and were more likely than outborn infants to have interventions held.
-

Increasing the Rate of Infants Rooming In with their Mothers with Low Acuity Congenital Heart Disease
Anna Nelson, Amy Marks, and Ekta Patel
Background The Children’s Mercy Fetal Health Center (FHC) was created to be able to deliver infants with complex fetal diagnoses including congenital heart disease. Mothers are referred from all over the Midwest region for their babies to have access to specialized care immediately after birth. Nearly all babies born in the FHC are admitted to our neonatal intensive care unit (NICU), as there are not well-established guidelines for keeping babies with their mothers if they have low-risk congenital heart disease that do not need intensive care continuous monitoring. Maternal infant bonding starts before an infant is born and becomes stronger in those first few moments after birth. Maternal infant bonding is important to help establish breastfeeding if desired and for early childhood development. Previously, only 27% of the patients with these diagnoses that would have been safe to room in with their mothers did. We aim to increase the rate of neonates born with low acuity congenital heart disease that room-in with their mothers in the FHC from 27% to 47% by October 2023. Methods We targeted infants with prenatal diagnoses of likely asymptomatic vascular rings, balanced AV canal, low risk intermittent fetal supraventricular tachycardia, tetralogy of Fallot without concern for pulmonary obstruction or low risk coarctation of the aorta. The first PDSA cycle implemented a protocol that was developed in collaboration with Pediatric Cardiologists to help providers assess the appropriateness of allowing a patient to room in with the mother with intermittent monitoring of vital signs. This protocol also dictates how frequently vital signs should be assessed by nursing once a baby is rooming-in with its mother. Education was provided to the physicians, NNPs and nurses about implementing the protocol. The second PDSA cycle included Fetal Cardiology APRNs discussing the appropriateness of patients rooming in with their mothers at weekly Fetal Health Center meetings. The quantitative data is collected monthly based upon FHC weekly patient e-mails and review of the medical records. Results The rate of infants rooming-in increased to 38% following implementation of the first PDSA cycle and up to 52% following implementation of the second PDSA cycle. Discussion We were able to increase the number of infants with low acuity congenital heart disease that roomed-in with their mothers in the FHC without any rapid responses. The next step is to survey families to better understand their experience of having their infant room-in with them in the FHC.
-

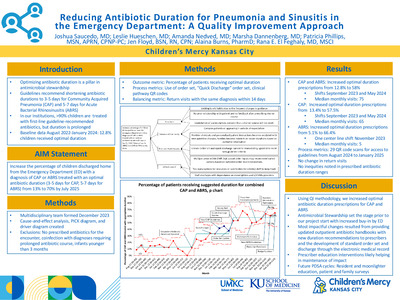
Increasing vaccination rates of 23-valent pneumococcal polysaccharide vaccine among patients at high-risk for invasive pneumococcal disease.
Edward Lyon, Tracey Wetzel, Ann L. Wirtz, Douglas Swanson, Rachel Moran, Jessica Peters, Christine Symes, Liset Olarte, and Rana El Feghaly
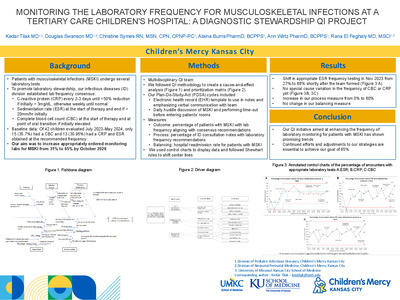
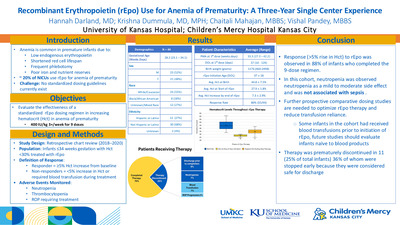
Introduction: Pneumococcal disease causes significant morbidity and mortality in children. Routine childhood immunizations protect for 13 or 15 pneumococcal serotypes via two pneumococcal conjugated vaccines. Patients with immunocompromising and chronic medical conditions are at high risk of invasive pneumococcal disease. A 23-valent pneumococcal polysaccharide vaccine (PPSV23) is recommended in these patients to protect against more pneumococcal serotypes, but many patients have not received it. Our AIM is to increase PPSV23 vaccination rates among eligible patients in both the inpatient and outpatient infectious diseases (ID) settings from a baseline of 44% to 55% by October 2024. Methods: In collaboration with Children’s Mercy integrated care solutions, we created a report of eligible patients evaluated by ID in the inpatient and outpatient settings. This report captures pneumococcal immunization history of patients eligible for PPSV23. In October 2022, we formed a multi-disciplinary team of ID nurses, a pharmacist, providers, and a patient advocate. We identified several potential causes of low PPSV23 vaccination rate and developed countermeasures (figure 1). Since October 2022, we have discussed the project weekly during our divisional huddle. In January 2023, we matched outpatient and inpatient reports to include maximal information and created a 2-way communication strategy where outpatient nursing staff notifies ID providers of patients who qualify for PPSV23. In February 2023, we created an EMR shared phrase to include in ID provider notes and a badge buddy with qualifying conditions for PPSV23 vaccination. Results: Following the initiation of the project we have seen an increase in qualifying patients who have received PPSV23 that has so far been sustained for 6 months (48-56%); we also see narrowing of the control limits implying improved process (figure 2). Discussion: We were able to increase PPSV23 vaccination of eligible high-risk patients in both the outpatient and inpatient settings. If this trend is sustained, we will be able to move our center line in 2 months. We have multiple additional plan-do-study-act cycles planned over the next several months to include electronic medical record changes, collaboration with different specialties and family education.
-

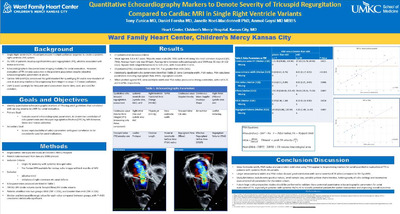
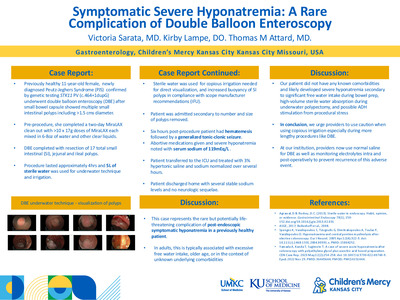
Latency Time From Prior Authorization Submission To Initiation Of Biologic Therapy In Inflammatory Bowel Disease
Shannon Capraro, Janelle R. Noel-Macdonnell PhD, Lauren Disselhoff, Layne Sieve, and Rachel Chevalier
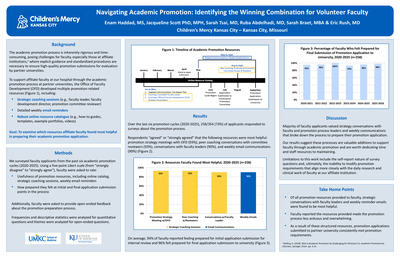
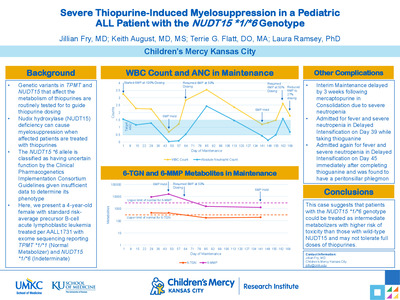
Background For pediatric patients with a diagnosis of inflammatory bowel disease (IBD), initiation of biologic therapy can be essential to attain disease control. Unfortunately, patients often experience delays in receiving the first dose of these medications due to the need for insurance companies to approve medication prior authorizations (PA). Physicians and support staff spend many working hours collating and transferring information regarding urgency to payors. To our knowledge, no studies exist to evaluate the factors that contribute to how quickly a medication is approved in pediatric patients. We set out here to evaluate which demographic and disease factors contribute to the lag time between submission of medication prior authorization for IBD biologic therapy and administration of that therapy. Methods Our pilot cohort consists of 102 patients with IBD who initiated biologics as an outpatient at our tertiary care hospital between the years of 2018-2023. Clinical information regarding disease status, previous therapies, surgical history, laboratory information, and medication administration information was obtained from the chart. Descriptive statistics were performed and followed by bivariate summaries for insurance status (Medicaid users vs. not), initial denial of biologic, and type of biologic. Wilcoxon Rank Sum Tests and Kruskal-Wallis Test were used to compare time from PA to first dose depending on variable of interest. Results Demographics are included in Table 1. Patients were median age of 14.7 years (interquartile range [IQR] 11.5-17.0) and were 52.9% male. Most patients (80/102; 78.4%) have Crohn’s disease. In this cohort, the median time from submission of prior authorization to administration of medication (lag time) was 15.0 days (IQR 12.0-24.0) with maximum times up to 53 days. When evaluating between medications, infliximab had a significantly lower median lag time (median 14d; IQR 10-16d) compared to ustekinumab (17.5d; IQR 13-28) or adalimumab (18d; IQR 14-25d) but not vedolizumadb (16d; IQR 11-26) (Figure 1). No other pairings showed a significant difference. Pediatric Ulcerative Colitis Activity Index (PUCAI) decreased the lag time 1.5 days for every 10-point increase in PUCAI. Hemoglobin, albumin, ESR, and CRP contributions to lag time varied between medications. Lag time does not vary significantly between state insurance (Medicaid) and private insurance (Figure 2). Additionally, an initial denial of the prior authorization requiring appeal does not prolong lag time. Conclusion Early initiation of biologic therapy can delay the progression of disease to stricturing or penetrating disease 2 . However, providers experience significant challenges administering these medications in a timely manner. Notably, pediatric patients with IBD often wait at least two weeks to receive their first dose of biologic therapy. Our preliminary analysis does not indicate that severity of illness or type of insurance make clinically significant differences. It is important to remark that our population was limited in the number of Medicaid patients, so more data will be essential to corroborate this analysis. Infliximab shows the quickest availability perhaps due to its long history on the market, availability of biosimilars, or widespread use. Further analysis of our collected cohort of approximately 400 patients is pending including analysis of outcomes.
-

Life Threatening Anemia and Acidosis Secondary to Systemic Loxoscelism in a Pediatric Patient
Rohan Akhouri, Vincent J. Calleo, and Leslie Hueschen
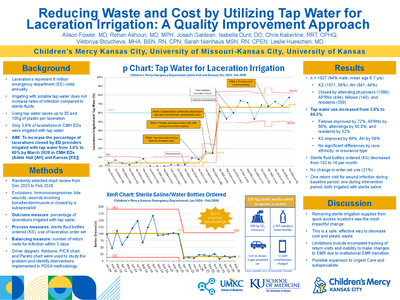
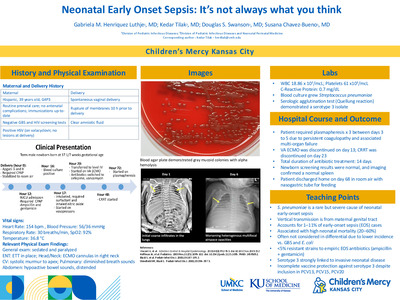
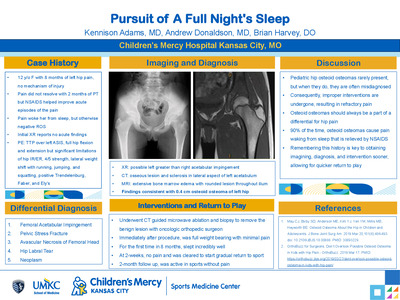
Introduction Rashes are common in pediatric patients and most resolve without significant patient illness. In rare cases, they can represent life-threatening disease entities. History is crucial to determine a rash’s etiology, and barriers like developmental delay and language can complicate accurate diagnosis. We present a case of hemodynamic instability and hemolysis without known envenomation, which was diagnosed as systemic loxoscelism. Case Description A 10-year-old male with developmental delay presented with decreased activity and reduced oral intake for 4 days. An interpreter was used due to a language barrier. Initial vital signs were T 36.6°C, HR=120, RR=20, BP=117/66, and SpO2 96%. The child was listless with 1+ peripheral pulses and a capillary refill of 4 seconds. Skin exam showed a warm, hyperpigmented rash with rough texture on his trunk and upper extremities. Initial VBG showed a pH=7.04 and pCO2=27. His CBC showed hemolytic anemia with Hg=3.2g/dL and extreme leukocytosis with WBC=61x10*3/uL. After initial fluid bolus the patient became hypotensive, and labs showed worsening acidosis with a pH=6.89, pCO2=22, and lactate of 27mmol/L. Resuscitative efforts included fluid boluses, antibiotics, blood transfusion, sodium bicarbonate, and high flow supplemental O2. He was subsequently admitted to the PICU. After initial stabilization, further history revealed the patient had a rash and cellulitis on his left shoulder and completed treatment with amoxicillin one week prior to presentation. During his PICU course, multiple subspecialty services were consulted to assist with his workup. He received additional packed red blood cells (PRBC), rasburicase, steroids, and antibiotics. His rash evolved with desquamating areas and eschar formation at the left shoulder. Based on the extensive systemic symptoms, negative work-up for other etiologies, and an evolving eschar, the diagnosis of systemic loxoscelism was made. After 5 days, the patient recovered with supportive measures and is currently being followed for hemolytic anemia. Discussion Only 5 % of Brown recluse spider (Loxosceles reclusa) bites develop severe systemic manifestations. Life threatening toxicity can include severe hemolysis, acidosis, and autonomic instability. Treatments are largely supportive and include IV fluids, PRBC transfusions, and steroids. Antibiotics are often indicated if there are concerns for infection, and hemodialysis may be indicated for life threatening acidosis. Often loxoscelism patients do not know they have a spider bite which can delay diagnosis. Some other challenges with the initial diagnosis and management of this case included language barrier and the patients developmental delay with decreased mentation. Conclusion Systemic loxoscelism is a rare and life-threatening condition that should be considered in patients with hemolysis and acidosis, especially in the setting of eschar formation. Diagnosing rare conditions in patients with language barriers and developmental delay can be challenging, and provider awareness can increase the chances of a proper diagnosis.
-

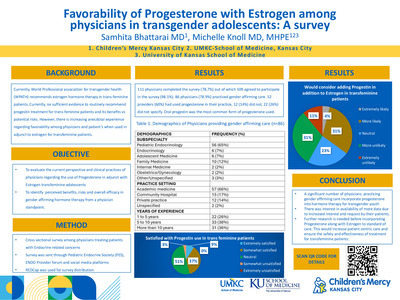
National Prescribing Practices for Dystonia Among Providers in the United States
Sarah Paige Davis, Natalie J. Kane, Haley Botteron, and Rose N. Gelineau-Morel
Objective: While multiple oral medications are used to treat dystonia, limited information exists on current prescribing practices. This study analyzes prescribing practices for dystonia in the United States, evaluating variations in dosing and impact of co-morbidities. Methods: Querying the Cerner Real World database from 2014 to 2019 for children age 0-18 with an ICD-10 diagnosis containing “dystonia” resulted in 11,300 inpatient and outpatient encounters. Information extracted included current dystonia medications (baclofen, clonidine, carbidopa-levodopa, gabapentin, tetrabenazine, trihexyphenidyl, and benzodiazepines including diazepam, clonazepam, midazolam, and lorazepam), medication dosing, and co-morbid diagnoses of cerebral palsy, epilepsy, or spasticity. Encounters without current weight were excluded from medication dosage analysis. Results: Benzodiazepines were most commonly prescribed for dystonia (61.2%), then baclofen (12.0%) and clonidine (9.5%). Patients with cerebral palsy (n=5639) were prescribed baclofen more than clonidine (16.2% vs 7.0%), while patients without cerebral palsy (n=5731) were prescribed clonidine more frequently than baclofen (11.7% vs 7.6%). All medications showed decreased mean dosing in milligram per kilogram (mg/kg) as patient weight range increased. Mean weight-based dosing for baclofen varied by weight group from 0.162 mg/kg/dose (110-120 kg group, mean dose 18.3 mg) to 0.662 mg/kg/dose (0-20 kg group, mean dose 9.3 mg). Conclusion: Benzodiazepines, baclofen, and clonidine are the most common medications prescribed for dystonia in the United States. Medication dosing is variable, with patients of higher weights receiving smaller weight-adjusted doses. There is a need for dystonia medication selection and dosing guidelines to standardize care and inform dosing recommendations for clinical trials.
-

Oscillometry in Term Neonates without Respiratory Disease
Anna Nelson, Cheri Gauldin, Brooke Smith, Venkatesh Sampath, and Winston M. Manimtim
Background Bronchopulmonary dysplasia (BPD) is one of the most common complications of prematurity. While severity of BPD is defined by need and type of respiratory support at 36 weeks, it does not distinguish between endotypes of disease. Recent studies suggest that infants with severe BPD have parenchymal, airway and pulmonary vascular disease. Determining the BPD phenotype could help guide future individualized therapy. Oscillometry is a bedside tool that measures the resistance of the airways and the reactance of the pulmonary parenchyma. Normative values of oscillometry need to be established to serve as a comparison prior to establishing oscillometry characteristics of the different types of BPD. This study aims to determine normative values of oscillometry for neonates without respiratory disease. Methods Neonates born at a gestational age of ≥ 36 weeks and in room air were recruited at < 29 days of age. Exclusion criteria included current supplemental oxygen or positive pressure support. Neonates were tested at their bedside while asleep, supine, with head and neck in neutral positioning. The Tremoflo N-100 oscillometry device was applied to the neonate’s face with a simple face mask and 2Liters/min bias flow was introduced into the system. Neonates were breathing spontaneously while the oscillometry device introduced 6 different frequencies (7 Hz, 13 Hz, 20 Hz, 29 Hz and 35 Hz) into the neonate’s respiratory system. The device then determined the reactance and resistance of the respiratory system at each frequency. Neonates were tested 3 times, in 30 second intervals, with a few minutes rest allowed between each test. Results Eight patients have been recruited to participate at this time. The participant group has an average gestational age of 38.1 weeks, average birth weight of 3176 grams and average birth length of 50.9 cm. Preliminary data demonstrates consistent reactance values at 37, 29 and 20 Hz, with reactance spacing out some as the frequency decreases. The measured resistance at these frequencies (37 and 29 Hz) is also clustered, although the resistance values remain consistent at 13 Hz as well. The resistance is greatest at the lowest frequency of 7 Hz. Two test subjects have outlying data, but this does not appear to be related to gestational age or size of the subject. There was no difference in reactance or resistance based on gestational age, birth weight or birth length. Discussion Our findings are consistent with previous studies that have demonstrated resistance in the airways is highest at the lowest frequency of 7 Hz and resistance decreases with increasing frequency (Klinger et al.) Reactance is most negative at the lowest frequencies and increases with increasing frequency. Oscillometry provides consistent and reliable data for evaluating the pulmonary function of term, healthy newborns.
-

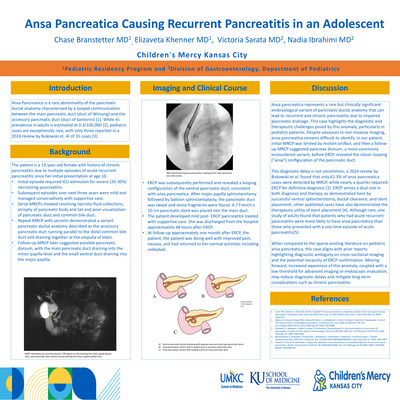
Rumination Syndrome Diagnosis Supported by Colon Manometry in a Pediatric Patient
Alex Biller, John Rosen, and Amornluck Krasaelap
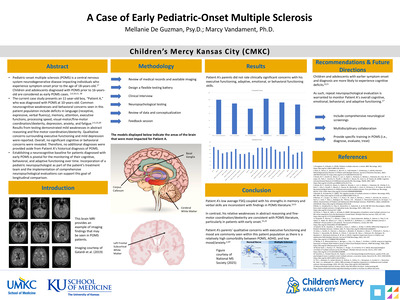
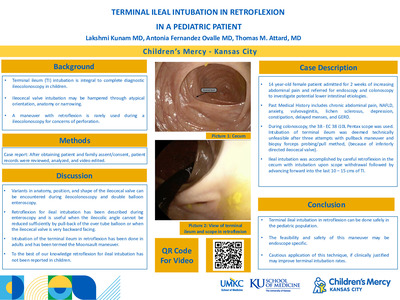
Introduction: Rumination syndrome is a disorder of gut-brain interaction characterized by effortless repetitive postprandial regurgitation, reswallowing, and/or spitting.(1) This condition is caused by increased intragastric pressure due to abdominal muscle contractions, leading to the opening of the lower esophageal sphincter and the return of gastric content into the esophagus.(1) Rumination is a clinical diagnosis after the exclusion of other etiologies of symptoms. The diagnosis of rumination is clinical, but supportive evidence can be obtained through esophageal or antroduodenal manometry.(2) We present a unique case report of rumination syndrome diagnosis supported by data obtained during colon manometry in a pediatric patient. Case: We describe the case of a 13-year-old male with autistic spectrum disorder who presented with chronic constipation, fecal soiling, and poor response to standard laxative treatments. An anorectal and colon manometry was performed prior to an antegrade continence enema procedure. The anorectal manometry showed normal resting anal pressures and recto-anal inhibitory reflex but revealed dyssynergic defecation. During the colon manometry, normal contractions were observed in the proximal colon, but during the postprandial phase, a simultaneous increase in pressure ("r" waves) was detected across all sensors in the colon. (Figure 1) Coinciding with this increase in pressure, the patient was observed to regurgitate and rechew food without experiencing any pain or discomfort. The family reported that the patient had been exhibiting this behavior since early childhood. In addition to modifying the patient's bowel regimen, diaphragmatic breathing exercises were recommended to address the rumination syndrome. Discussion: This is the first reported case in which rumination syndrome was diagnosed using colon manometry. The presence of repetitive regurgitation and reswallowing during the postprandial phase alone would have been sufficient for establishing the diagnosis. Additionally, the simultaneous increase in pressure ("r" waves) observed across multiple colon sensors supports the diagnosis of rumination syndrome. These pressure waves likely originate from skeletal abdominal muscle contractions rather than from the stomach or intestines. Conclusion: Rumination syndrome is diagnosed based on the clinical presentation of effortless repetitive postprandial regurgitation, reswallowing, and/or spitting. Colon manometry, which detects spontaneous increases in pressure across multiple sensors due to abdominal muscle contractions, can be a valuable tool in supporting the diagnosis of rumination syndrome.
-

Sangrado del Tubo Digestivo Alto Secundario a Infección de Adenovirus
Moises Alatorre-Jimenez, Sarah T. Edwards, and Thomas M. Attard
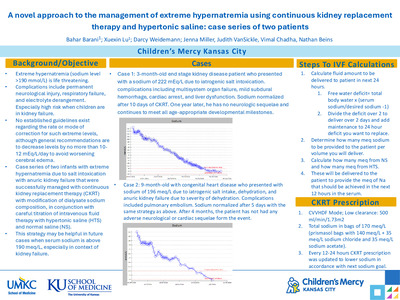
Titulo: Sangrado del Tubo Digestivo Alto Secundario a Infección de Adenovirus Introducción: El Sangrado del tubo digestivo alto (STDA) es causado por múltiples etiologías incluyendo gastritis, varices, esofagitis, anomalidades vasculares, cuerpos extraños, y ulceras (1). Dentro de estas causas se conoce que infecciones virales pueden producir ulceras causando sangrado los más comunes son el virus de Epstein- Barr, Covid-19, Herpesvirus-6, Herpesvirus-7 y Citomegalovirus (1,2,3,4,5). Presentamos el caso de un paciente con STDA severo a causa de infección por adenovirus. Reporte de Caso: Paciente de 22 meses de edad, previamente sano que se presenta al servicio de Urgencias debido a un día de fatiga, anorexia y melena. El paciente presento a la hora de ingreso presento episodios de hematemesis. Laboratorios al momento demostraron anemia con hemoglobina de 8.2gm/dL, leucopenia 2.7 x 10x 103/mL, acidosis, elevación de las transaminasas (AST 553 U/L, ALT 417 U/L) y TP/INR normal. El paciente requirió varios paquetes de sangre, elevando su hemoglobina a 10.4 gm/dL y empezó tratamiento con infusión continua de octreotida y pantoprazol IV. A pesar del tratamiento continuo con hematemesis y la hemoglobina disminuyo a 6.7 gm/dL en menos de 8 horas post transfusión. El paciente fue llevado al quirófano para control hemorrágico con endoscopia. Se identifico de inicio un coagulo de gran tamaño (fig.1) que fue succionado demostrando múltiples ulceraciones serpiginosas profundas predominantemente en el fondo gástrico (fig 2). Múltiples de las ulceraciones tenían sangrado lento y se procedió a control con Hemospray®. Múltiples estudios virales incluyendo sangre, heces, o respiratorios concluyeron positivo para Adenovirus en PCR. Posterior al procedimiento el sangrado se detuvo y los laboratorios regresaron a valores normales. Se repitió la endoscopia tres meses visualmente normales. Discusión: Se han presentado varios casos en la literatura de STDA causado por en algunos casos por una infección viral (1). Los casos de ulceras por adenovirus son reportados en pacientes adultos y/o inmunocomprometidos (6). No hay casos reportados en pacientes pediátricos previamente sanos con infección de adenovirus causando STDA. La identificación de adenovirus en ulceras gástricas pudiera ayudar en un futuro a evitar iniciar tratamiento con antivirales, aunque pocos casos en la literatura (5). Conclusión: Reportamos este caso de pacientes pediátrico STDA causado por ulceras por adenovirus donde no se han encontrado casos reportados previamente en la literatura.
-

Teaching and Tomorrow: Children's Mercy Hospital Pediatric Gastroenterology Fellowship Program
Children's Mercy Kansas City
-

The Implementation of a Pectus Bar Insertion ERAS Pathway
Todd A. Glenski, Emily Weisberg, Christian M. Taylor, Brandon Layton, Andrea Melanson, and Sameer Lalani
-

A Genomics Driven Pluripotent Stem Cell Model of Infant Acute Lymphoblastic Leukemia
Meagan Vacek, Jacqelyn Nemechek, Julia Draper, Irina Pushel, Bradley Thornton, Molly Leyda, Priyanka Prem Kumar, Midhat S. Farooqi, Jay L. Vivian, Erin M. Guest, and John M. Perry
Acute lymphoblastic leukemia in infants (iALL) is a high-risk subtype of childhood leukemia, with poor survival outcomes despite intensive therapies. Rearrangement of KMT2A (KMT2A-r) on chromosome 11q23 is the most frequent cytogenetic abnormality in iALL, occurring in 70% of cases. KMT2A-r is associated with chemotherapy resistance, early relapse, and rapid leukemic progression, all of which contribute to poor survival outcomes. The most common KMT2A-r in iALL is KMT2A::AFF1 (MLL::AF4), derived from t(4;11)(q21;23) and arises in utero as shown in multiple clinical studies. Infant ALL’s cell of origin is thought to be a very early hematopoietic precursor, with transcriptomic studies of iALL blasts showing similarities to hematopoietic stem and progenitor cells (HSPCs), multipotent progenitors and early lymphoid progenitors (ELPs). Despite this, much is unknown regarding how KMT2A::AFF1 transforms early hematopoiesis, the cell types of origin, or how it alters the severity of the disease. Additionally, existing iALL models fail to mimic human disease, which creates an essential, ongoing need for the development of representative model systems for this devastating disease. To understand the development and progression of iALL, we have created a highly controlled human induced pluripotent stem (iPS) cell model to uncover the genomic and epigenetic landscape and cellular evolution of KMT2A::AFF1 iALL. Preliminary studies reveal our ability to differentiate human iPS cells into functional HSPCs with multilineage differentiation capacity and successfully express the doxycycline inducible KMT2A::Aff1 transgene in a controlled manner. We have also generated an in-house reference library of single cell RNA sequencing data and have compared transcriptomes of KMT2A-r blasts from iALL patients. This data revealed KMT2A-r cells are transcriptionally similar to ELPs. The goal for future investigations is to use single cell genomics to investigate transcriptomic changes during hematopoietic differentiation of our KMT2A:Aff1 iPS cell line. We also plan to compare these cells to publicly available single cell RNA sequencing data from multiple datasets that encompass fetal bone marrow and HSPC development. Through this research we expect to discover unique mechanisms of iALL emergence and progression with the long-term goal to uncover targets specific to iALL for the development of new therapies.
-

Exploring bidirectionality in US pediatric global health programs
Anik Patel, Pauline Kamau, Ashley Combs, and Megan McHenry
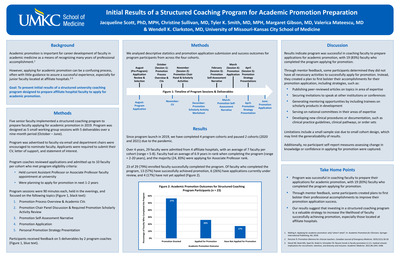
Introduction: Over the last two decades, GH programs have offered experiences at partner sites through established global health partnerships (GHPs). Historically, GHPs have been one-directional, favoring partners from resource-rich settings. These partnerships are now being reevaluated through the lens of equity and decolonization. We seek to understand how US pediatric GH faculty define the concept of “bidirectionality”, assess perspectives on their institution’s practice of bidirectional activities, and explore perceived benefits and challenges to prioritizing bidirectionality within their own GHPs. Methods: This is a cross-sectional qualitative survey study on bidirectionality of 206 AAMC-accredited US pediatric residency programs. 24 survey responses from global health faculty or staff at these programs were received. The REDCap-based online survey was developed by iterative repetition with a diverse author group. Data was collected from January 18, 2023 to February 20, 2023. Free-text responses were reviewed and coded through an inductive approach. Results: The majority of participants were “very familiar” with bidirectionality. Bidirectionality was described in terms of reciprocity, equity, and collaboration. Examples of programs’ own efforts to be bidirectional varied, and examples given varied to the degree of achieving bidirectionality. Perceived benefits of bidirectionality included friendship and mutual respect, educational opportunities, and opportunities to achieve equity. Perceived challenges of bidirectionality included technical barriers, cultural barriers and mismatched expectations, and financial barriers. Despite challenges, participants expressed persistence and the ability to be flexible in order to create and maintain bidirectional GHPs. Conclusions: A shared concept of bidirectionality exists, whereby partners collaborate at the personal and institutional level, forming a relationship based on mutual respect and understanding, resulting in a reciprocal and equitable exchange of benefits. Perceived benefits of bidirectionality can be difficult to quantify and justify in comparison to perceived challenges of bidirectionality. US pediatric GH programs should continue to reevaluate their own GHPs to assess if they are achieving true bidirectionality.
-

“It's so expensive and isn’t any better! Or is it?” A Comparative Analysis of Price per ECMO Hour, Intracranial Hemorrhage, and Survival Rates in Neonates on Bivalirudin vs. Heparin
Johanna I. Orrick, Jessie Charbonneau, Kari L. Davidson, Alexandra Oschman, and John M. Daniel IV
Background: Heparin has been the anticoagulant of choice for Neonatal ECMO for the past thirty years. It has the benefit of being well studied and having a low production cost. As bivalirudin is a newer anticoagulant, it has not been as widely studied and has a higher production cost, many centers are concerned about changing to a newer, more expensive agent. Bivalirudin has been studied from both an efficacy and cost perspective in adult patients (Sun et al 2021) and pediatric VAD populations (Burnstein et al 2023). While some safety and efficacy data exist for neonates, there are few if any cost analyses between Heparin and Bivalirudin. Methods: This was a single center, retrospective study conducted over 51 months in neonates receiving heparin or bivalirudin at an 86-bed, Level 4 NICU. The primary objective was to evaluate the price per ECMO hour, incidence of intracranial hemorrhage (ICH), and survival rates were examined. Data from 68 patients was collected (diagnosis, gestational age, anticoagulation type and cost, ECMO duration, number and cost of component changes, anticoagulation lab costs and frequency, ICH occurrence, and survival outcome). Total cost per ECMO hour was calculated. Drug costs were calculated utilizing average wholesale price (AWP). Quantitative analysis was conducted using two-tailed tests and chi-squared analyses. Significance was set at p = 0.05. Results: No significant differences between weight and gestational age were noted. Thirty-nine patients received continuous infusion heparin, and 29 received bivalirudin infusions with short periods of heparin for trialing off ECMO per hospital protocol. No statistically significant difference was found in cost per ECMO hour between bivalirudin ($54.14) and heparin ($58.27). There was a trend towards significance in survival for patients treated with bivalirudin compared to heparin, with a statistically significant decrease in ICH seen with bivalirudin (p < 0.05). Conclusion: Our study is one of the first to illustrate that the cost difference per hour of ECMO between heparin and bivalirudin is negligible, approximately $4.00. Additional analysis utilizing proprietary, center specific, contract pricing revealed cost savings with bivalirudin. Additionally, there was a clinically and statistically significant reduction in ICH using bivalirudin over heparin. While our data did not show a statistically significant difference in survival, our data did trend towards significance. As this was a small sample size and single center study, wide study across the ECMO community is warranted.
-

Rare Complications Associated with Use of Bovine Pericardium
Mohamed Aashiq Abdul Ghayum, Nitin Madan, William Gibson, and Sanket Shah
Background Bovine Pericardium (BP), with numerous and improving preparation techniques, has been used extensively for over 50 years in repair of simple and complex congenital heart defects. It has several advantages over other surgical materials. However, there is a paucity of data in the pediatric population regarding complications associated with BP. Herein, we report two rare complications noted with BP use. Case Description Case 1. A 14-month-old male, with trisomy 21 and complete Atrioventricular canal defect, repaired using BP. A routine surveillance echocardiogram showed a mass attached to the atrial septum and atrial aspect of the left atrioventricular valve (Figure 1A). Surgical intervention was deemed necessary as serial echocardiogram after admission showed an enlarging mass. Pathology showed a fibrin thrombus undergoing transition to granulation tissue. Case 2. A 10-month-old girl, with mosaic trisomy 9 and Tetralogy of Fallot, underwent a transannular patch repair using BP. An outpatient follow-up echocardiogram showed fluid collection around RVOT patch with intraluminal compression with a confirmatory CT angiogram (Figure 1B). Redo median sternotomy revealed purulent appearing fluid within an intact patch. Fluid culture showed no growth and pathology sections revealed fibrous tissue with a mixed inflammatory cell infiltrate including necrotizing granulomas. Conclusion These two cases illustrate that, albeit rare, complications can occur with the use of BP in the pediatric population. In our patients, thrombus and sterile abscess occurred within six months postoperatively and were incidentally identified. Literature is presently inconclusive about the exact mechanism for the inflammatory reaction noted with BP use and warrants further research.
-

ECMO Clinical Practice Committee: Empowering the frontline staff
Michelle McKain, Shayna Evans, Johanna I. Orrick, and Kari L. Davidson
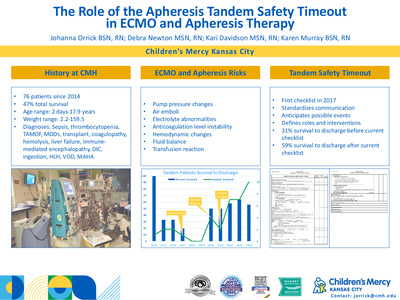
Background: Extracorporeal Membrane Oxygenation (ECMO) is a complex artificial life support for patients with severe respiratory and cardiac failure. Children’s Mercy was an early ECMO pioneer, establishing a program in 1987. Despite CM’s successful history, wide variations existed between regional management of ECMO (Schwartz et al., 2022). Studies show that patient outcomes, resources, staff satisfaction, and financial metrics improve with implementation of an interprofessional shared governance team (Olender et al., 2019; Schwartz et al., 2022). In 2016, the ECMO Clinical Practice Committee (ECP) was created, tasked with addressing projects aimed at ECMO process improvements. Methods: ECP members include Registered Nurses (RNs) and Respiratory therapists (RTs) from ECMO leadership, ECMO Core Team (primers), and ECMO bedside specialists. Their home units include the Neonatal, Pediatric, and Cardiac Intensive Care Units. The committee meets every other month to focus on education, retention, clinical practice improvement, protocol development, and project implementation. It is led by an ECMO bedside specialist RN. ECP receives ideas from Situation Target Project (STP) submissions or passed down from ECMO leadership and specialist meetings. Results: Successful ECP projects have included safe ECMO patient mobility plans, anticoagulation guidelines, staffing model change and development, education offerings for non-ECMO caregivers, tandem therapy protocols, standardizing patient assessments, and development of the ECMO Quality Improvement (EQI) checklist. These implementations have improved patient care, optimized resource management, enhanced multidisciplinary cooperation, and increased bedside staff satisfaction. Conclusion: Environments where the bedside staff contribute to decision-making processes are linked to employee satisfaction and improved patient outcomes (Kowalski et al., 2020). Children’s Mercy’s ECMO program’s growth and success are due in no small part to ECP’s collaboration, innovation, and dedication.
-

An Unusual Cardiomegaly Culprit: Case Report Of A Hemodynamically Significant Portosystemic Shunt
Zoetta L. McLoughlin MD, Melanie Kathol, and Amanda McIntosh
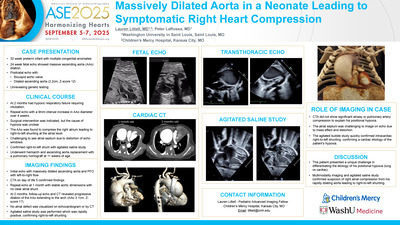
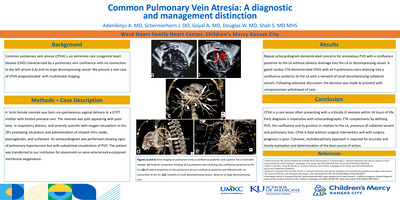
Background: Cardiomegaly discovered in the fetal or neonatal period may be the first sign of cardiac disease. However, the differential diagnosis for cardiomegaly with a structurally and functionally normal heart includes cardiomyopathies as well as non-cardiac etiologies, including extracardiac shunt lesions and vascular malformations, among others. Thus, unexplained cardiomegaly requires further investigation for extracardiac anomalies. In this case, we focus on an unusual etiology of diffuse cardiac dilatation – intrahepatic portosystemic shunt – that was initially misdiagnosed as dilated cardiomyopathy. Case Description: A 9-year-old male with history of learning difficulty and tall stature was seen for follow-up of diffuse cardiomegaly present since fetal life, initially diagnosed as likely dilated cardiomyopathy. He was otherwise healthy and asymptomatic. Echocardiogram demonstrated persistent four chamber and aortic root dilatation with preserved biventricular systolic function, normal wall thickness, and normal valvular function. However, a new finding of hepatic vein dilatation prompted further evaluation. Abdominal ultrasound showed abnormal intrahepatic vasculature concerning for portosystemic shunt. After confirmation on CT angiogram, he underwent resection of the abnormal vascular connection. He had an uncomplicated post-operative course and repeat echocardiogram showed improvement in ventricular size. Conclusion: Cardiomegaly is a common presentation of underlying cardiac disease but can less commonly be caused by extracardiac abnormalities. Here, we highlight a case of intrahepatic portosystemic shunt as an uncommon, yet important etiology to consider when evaluating unexplained cardiomegaly in a pediatric patient.
-

Delirium on Admission to the CICU
Spencer Wittmeyer, Jaime Silva-Gburek, and Kelly S. Tieves
Background: Delirium is increasingly recognized in the pediatric cardiac intensive care unit (CICU) with an incidence up to 67% and is associated with worse outcomes including increased mortality, prolonged hospitalization, and increased rates of intubation and mechanical circulatory support. The Cornell Assessment for Pediatric Delirium (CAPD) is the only validated tool for the diagnosis of delirium in the pediatric population. The CAPD may be limited in children with developmental disabilities as it does not account for baseline ability in scoring. Prior work has identified low specificity for the CAPD in children with developmental disabilities and those requiring mechanical ventilation. This may lead to overdiagnosis and possible ‘overtreatment’ with pharmacologic therapies for delirium. Study aims were to identify the incidence of patients who were diagnosed with delirium upon CICU admission and describe characteristics of this population including age, developmental status, and medical complexity. Methods: Retrospective single-center cohort study. All children admitted to the CICU between October 1, 2021 to December 31, 2022. Delirium was defined as a CAPD score >9. Results: In total, 683 patients were admitted with a median age of 10 months. Admission delirium screening was performed in 584 (85%) patients, 196 (33.3%) met the a priori definition of delirium. Younger patients were more likely to have a positive delirium screen on admit with a median age of 6 months compared to 17 months in those with a negative screen (p=0.00). There were no significant differences in the frequency of chromosome abnormality (p=0.17), duration of CICU (p=0.196) or hospital length of stay (p=0.09) in patients with or without a positive delirium screen. Conclusion: Infants were more likely to screen positive for delirium upon admission to the CICU. Further investigation is needed to explore factors associated with positive CICU admission delirium screen.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}