
These posters have been presented at meetings in Children's Mercy and around the world. They represent research that was done at the time they were created, and may not represent medical knowledge or practice as it exists at the time viewers access these posters.
-

Impact of Remote Monitoring During the Interstage Period on Outcomes in Single Ventricle Patients Across Socioeconomic Groups
Bianca Cherestal, Lori Erickson, Janelle R. Noel-Macdonnell, Girish S. Shirali, Hayley S. Hancock, Doaa Aly, and Natalie Jayaram
Background: Despite improvements in outcomes over time, morbidity and mortality for infants with single ventricle (SV) heart disease remains high. Among other risk factors for mortality, infants of low socioeconomic status (SES) are known to be particularly vulnerable following stage 1 palliation. We sought to determine whether use of a novel remote monitoring program, CHAMP (Cardiac High Acuity Monitoring Program), mitigates differences in outcomes by SES for infants with SV during the interstage period. Methods: Using the CHAMP database, we identified 607infants across 11 institutions enrolled in the program between 2014–2021. All enrolled patients’ families were provided with a Windows-based tablet with built in cellular capability, at no cost to them, and video capability allowing for instantaneous transfer of patient information to the care team. Patients were divided into SES tertiles based upon six unique variables relating to SES status. Hierarchical logistic regression, adjusted for potential confounding characteristics, was used to determine the association between SES and mortality or transplant during the time between the first and second palliative procedures (interstage period). Results: Of 607 infants in the study cohort, 44 (7.2%) died or were listed for transplant during the interstage period. In univariate analysis, non-hispanic/non-latino patients, patients with renal failure following stage 1 palliation, patients with ventricular dysfunction prior to discharge, and patients with AV-valve regurgitation prior to discharge were at higher risk for mortality or need for transplant during the interstage period. The rate of mortality or need for transplant between SES tertiles was not statistically significant (p=0.18). Even after multivariable adjustment, the odds of mortality or transplant were no different for those in the middle [odds ratio (OR) 2.170, 95% confidence interval (CI) 0.789, 5.971, p=0.133] or highest (OR 1.003, 95% CI 0.297, 3.388, p=0.996) SES tertile compared to patients in the lowest SES tertile. Conclusion: In a large cohort of infants with SV heart disease enrolled in a digital remote monitoring program during the interstage period, we found no difference in outcomes based upon SES. The findings of this study are in contrast to findings from prior studies showing worse outcomes for SV patients of low SES. Our study suggests this novel technology could help mitigate differences in outcomes for this fragile population of patients.
-

Safety, Timing, and Outcomes of Early Postoperative Cardiac Catheterization Following Congenital Heart Surgery
Karoline Krzywda, Jeremy Affolter, Darcie Al-Hassan, William Gibson, Ryan Romans, and Kelly S. Tieves
Intro: Historically, early postoperative (<6weeks) cardiac catheterization (EPOCC) was considered high risk and often delayed. Recently, the safety of early postoperative cardiac catheterization has been demonstrated. The timing of catheterization in the struggling postoperative patient remains variable and optimal timing remains uncertain. There is limited data on the impact of EPOCC on outcomes such as length of stay, duration of mechanical ventilatory or extracorporeal support, and surgical or catheter- based interventions. The aim of this study was to describe our experience with EPOCC and its impact on management, length of stay, and duration of mechanical ventilatory support. Methods: This is a descriptive retrospective cohort study of patients who underwent cardiac surgery between 01/01/2010 and 12/31/2019 and cardiac catheterization within 30 days after surgery. Patients with catheterization for LA decompression on ECMO, endomyocardial biopsy, or BAS post hybrid procedure were excluded. We collected information surrounding timing, indication, and complications of catheterization, duration of mechanical ventilation/ECMO, and ICU/hospital LOS and compared these differences in patients who underwent EPOCC < 72hours (earlier) versus >72hours (later). Data was analyzed using IBM SPSS, version 28. Chi-square and Student’s t-test, or appropriate nonparametric tests were used to compare categorical and continuous variables, respectively. Results: There were 2542 surgeries performed during the study period with 167 patients undergoing cardiac catheterization within the defined 30 days. Twenty-six patients met exclusion criteria, leaving 141 patients for analyses. Median time from surgery to EPOCC was 10 days (1-30), with 26 patients(18.4%) having an earlier EPOCC. Interventions were performed in 70 patients (49.6%), not statistically different in those with earlier vs later EPOCC [n=9 (12.9%) vs 61 (87.1%), p=0.09]. Most common interventions included arch (n=9), atrial septum (n=9), collateral (n=9), and combination procedures (n=13). Complications of catheterization occurred in 10 patients (7%), not statistically different in the earlier vs later groups [n=6 (60% ) vs 4 (40%), p= 0.09]. Majority of complications were related to arrhythmia/ST segment depression, none included death or stroke. Patients with earlier EPOCC were statistically older (3 mos vs 1.5 mos, p=0.02) and weighed more (5.4kg vs 3.9kg, p=0.006) than those in the later EPOCC group. There were no statistically significant differences in median ICU length of stay (17.9d vs 28d, p=0.09), hospital length of stay (29.6d vs 49.9d, p=0.16), duration of mechanical ventilation (11.4d vs 13.4d, p=0.11) or duration of extracorporeal support (7.0d vs 15d, p=0.06) in the earlier vs later EPOCC groups. Discussion: The occurrence of complications related to EPOCC in our cohort was low, consistent with previously published work. While we did not demonstrate statistically significant differences in outcomes in patients who had catheterization performed earlier vs later after surgery, there is a trend towards significance with a higher number of catheter- based interventions, longer length of stay and duration of extracorporeal support in those patients who underwent later EPOCC. EPOCC appears to be safe when done < 72hours following surgery and we speculate that earlier catheterization may result in earlier intervention and a resultant decrease in extracorporeal support, ICU, and hospital length of stay. Our study is limited by the retrospective nature and small sample size. Further investigation is warranted.
-

Hemoglobin A1c Increase in Youth at Risk for Developing Type 2 Diabetes Mellitus During the COVID-19 Pandemic
Erica Wee, Ashley Sherman, Mark A. Clements, Kelsee Halpin, and Yun Yan
-

Hyperinsulinemic Hypoglycemia and Growth Hormone Deficiency secondary to 20p11 deletion
Erica Wee, Kavitha Dileepan, Sarah Tsai, and Emily Paprocki
-

Myocardial work by strain echocardiography: a predictor of exercise capacity in the Fontan population
Amulya Buddhavarapu, Suma Goudar, David A. White, Daniel Forsha, and Doaa Aly
INTRODUCTION: Global myocardial work index (GWI) obtained by non-invasive pressure-strain loops is a fast-emerging tool to assess myocardial contractility, independent of loading conditions. Data about the feasibility and utility of this modality in single ventricles are still lacking. AIM: We aimed to explore the relationship between the non-invasive myocardial work indices and exercise parameters in the Fontan population. METHOD: Fontan patients were prospectively evaluated by exercise testing and echocardiography. The systemic ventricle was tracked in 3 orthogonal apical planes for global longitudinal strain (GLS). Pressure-strain loops were generated against brachial blood pressure (surrogate for ventricular systolic pressure in the absence of outflow obstruction). GWI, global work efficiency (GWE), global constructive work (GCW) and global wasted work (GWW) were calculated. Peak VO2 and percentage of predicted peak VO2 were recorded during the same visit. RESULTS: Seventeen Fontan patients were included, 10 (58%) of whom had systemic left ventricle. Mean age was 13.8 y (range 9-21 y). Peak VO2 was 24.7 ± 5.9 ml/kg/min and predicted VO2% was 57.4 ± 11.1%. GLS was -14% ± 2.5%. Mean GWI was 979.9 ± 232 mmHg% which showed a strong correlation with the predicted VO2% (r=0.78, p < 0.001). Similarly, there was a strong correlation between GWE (mean= 87 ± 4.8%) and predicted VO2% (r=0.76, p=0.001). Less correlation was found between GLS and predicted VO2% (r=-0.58, p=0.019). GCW was 1293 ± 399 mmHg% and GWW was 161.1 ± 88 mmHg%. GWW had a moderate negative correlation with peak VO2 and predicted VO2% (r= -0.45, p=0.07 and r=-0.48, p= 0.06 respectively). CONCLUSION: Peak exercise capacity- a proven prognostic marker in the Fontan population, correlates strongly with GWI and GWE. Therefore, indices of myocardial work by non-invasive pressure strain loops are feasible measures in Fontan patients that may provide new insights into risk stratification.
-

Use of CGM in Monitoring Neonatal Diabetes
Emily Metzinger and Kelsee Halpin
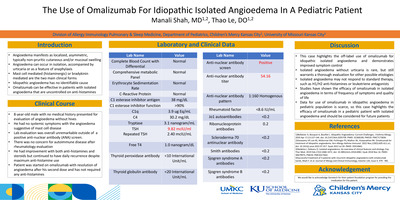
Introduction Although continuous glucose monitoring (CGM) has increased in patients with Type 1 diabetes, its use in the neonatal population has remained limited. Neonates, particularly preterm infants, are at risk of impaired glucose control. Several studies have looked at the use of these devices in improving care for premature infants without diabetes. We describe a case of a very low birth infant with neonatal diabetes secondary to a GATA-6 mutation. Clinical Case This is a late preterm infant with IUGR, truncus arteriosus, and neonatal diabetes. Exome genetic panel showed a mutation in GATA-6. Her neonatal diabetes was challenging to control due to variable blood sugars and sensitivity to insulin. Weight gain remained poor. A CGM (Dexcom G6) was placed when the infant was 1.59kg to optimize her diabetes management and improve weight gain. An insulin titration chart was used to adjust her IV regular insulin infusion according to the CGM glucose levels and trend arrows. The following outcomes were reviewed and analyzed fourteen days before and after CGM placement: glucose levels (238 vs. 177 mg/dL), percentage of glucose levels within target range of 70-180mg/dL (31% vs 51%), average number of daily POC glucose checks (10.2 vs. 6.9), average amount of insulin received per day (0.42 vs 0.52 units/day), and average weight gain (11.4 vs. 20.7 grams/day). The discrepancy between POC and CGM glucose was also analyzed. CGM was within 20% of POC values 44% of the time and within 30% POC values 70% of the time. Adverse side effects of CGM were also noted. The patient was started on antibiotics following a small abscess identified underneath the CGM site. Bruising and skin breakdown were noted at the site, and the patient completed a course of antibiotics for the cutaneous infection. There were no other concerns of infection related to CGM for the first 2.5 months following CGM placement. Conclusion This case highlights that CGM can effectively be used to optimize glucose management in neonatal diabetes in a very low birth weight infant. However, the area where the CGM is placed needs to be monitored for signs of infection. The use of continuous glucose monitoring (CGM) in newborn infants has remained limited even though newborn infants are at risk of impaired glucose control. We describe a case of a very low birth weight infant with neonatal diabetes in which a CGM was placed. Following placement of a CGM, average glucose levels were lower, the average amount of insulin received per day was increased, and average weight gain per day improved. Adverse side effects included infection at the site of the CGM. This case highlights that CGM can be used to optimize glucose management in neonatal diabetes.
-
 in An Infant Presenting with Respiratory Failure in An Infant Presenting with Respiratory Failure and Arterial Calcification by Lilah Melzer, Catharine Kral, Bonnie Sullivan, Eric T. Rush, and Erin Khan")
A Rare Case of Suspected Generalized Arterial Calcification of Infancy (GACI) in An Infant Presenting with Respiratory Failure in An Infant Presenting with Respiratory Failure and Arterial Calcification
Lilah Melzer, Catharine Kral, Bonnie Sullivan, Eric T. Rush, and Erin Khan
-

Case presentation: Pulpal Obliteration in Primary Dentition of an 8-year-old, Differential Diagnosis Dental Dysplasia Type II.
Tara Craven, Amy Burleson, Brenda S. Bohaty, Jenna Sparks, Neena Patel, and Aparna Naidu
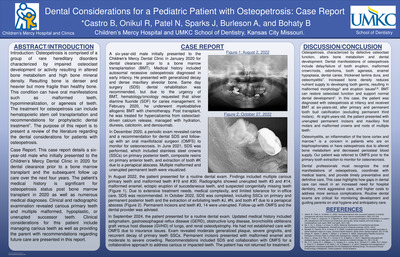
Tooth development anomalies can happen at many stages of cell development and are relatively common. These anomalies can be isolated findings however, they may also indicate minor or major associated syndromes and identification of these findings are essential to providing comprehensive care for patients. Dentin Dysplasia Type II is a rare autosomal dominant disease resulting from a disruption in the apposition stage of cell development. This disease affects the primary teeth and clinical manifestations can include bulbous crowns, cervical constriction, mild discoloration (amber color) and pulp obliteration. Permanent teeth tend to look typical but can demonstrate thistle-tube shaped pulps and/or multiple pulp stones. This case presentation discusses an 8-year-old male patient who presented with chronic decay and enlarged pulps noted at first clinical exam and radiographic interpretation. Following restorative treatment, the patient experienced loss of Stainless-Steel Crown (SSC) with remaining coronal tooth structure due to pulpal obliteration. A differential diagnosis of Dentin Dysplasia Type II was determined with the aid of a local oral pathologist. Patient was advised to seek genetic testing to improve treatment planning capabilities and further recommendations.
-

Characteristics of High-Acuity Patient Transfers to the PICU for Status Asthmaticus
Lilah Melzer, Marc Sycip, and Jade B. Tam-Williams
-

Concurrent COVID19 pneumonia and systemic inflammatory syndrome in a two-week-old requiring ECMO
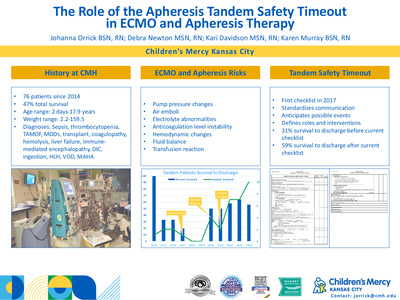
Jennie Godwin, Ayan Rajgarhia, Johanna I. Orrick, Jenna Miller, and John M. Daniel IV
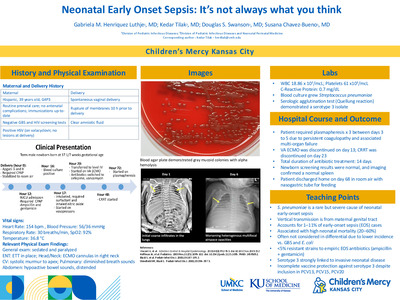
Objectives: * Initially, newborns seemed to be relatively spared from severe COVID-19. However, with the emergence of the B.1.617.2 (Delta) variant hospitalization rates among children aged 0-4 years increased by 10-fold by the middle of August 2021. We present a case of a 2-week-old previously healthy preterm, twin, male infant who developed severe COVID-19 pneumonia, subsequent acute respiratory distress syndrome (ARDS), and an inflammatory syndrome requiring VA – ECMO support for 22 days. Methods: * A retrospective chart review was performed after successful weaning from ECMO. Parental permission for a case report was obtained in compliance with institutional standards. Results: * Multiple challenges were encountered during this patient’s 22 days on ECMO. Rising markers of inflammation (LDH, Ferritin, D-dimer, CRP, ESR, troponin) made us concerned for multi-system inflammatory syndrome (MIS) in the setting of pneumonia. This complicated our treatment plan and led to a limited trial of immunomodulating agents in a baby with concurrent viral pneumonia. Dexamethasone, IVIg, and Anakinra were used. After treatment with these agents, clinical improvement began with a slowly clearing chest x-ray (Table 1 and 2) and weaning of ECMO flows. He developed seizures concerning for stroke in the setting of stable markers of coagulation, necessitating faster weaning and earlier ECMO decannulation than desired. Imaging studies showing extensive change to the lung architecture and ultimately required tracheostomy placement. Conclusions: * Severe COVID19 in infants remains a rare condition. Most infants have mild symptoms and recover completely. Unfortunately, some develop severe illness requiring extracorporeal life support. These infants can be successfully managed on ECMO during their acute crisis. The presents of a what appears to be a concurrent hyperinflammatory syndrome presents additional management challenges, but use of immunomodulating agents should be considered in infants.
-

CVST As A Rare Complication of Acute Pediatric COVID-19
Erin Bolen, Jonathan Ermer, and Mukta Sharma
A case report and literature-review derived case series of pediatric central venous sinus thrombosis as a late complication of COVID-19.
-

Improvement in Follow-up Communication for Resident-Identified Patient Safety and Hospital Process Issues
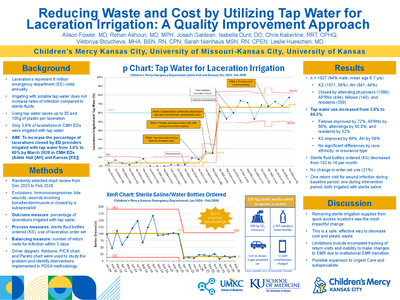
Ross Newman, Angela Etzenhouser, Emily Killough, Danielle Reed, Allison Adam, Michelle Brown, Kelly Meyer, Denise Bratcher, and Nicholas Clark
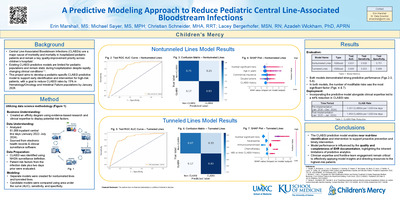
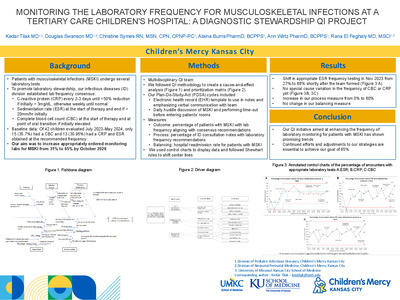
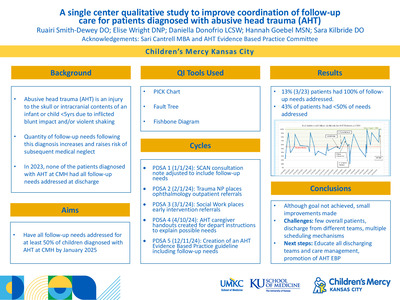
BACKGROUND: Lean concepts, including Daily Management Systems (DMS), have been adopted by health systems to prioritize high-quality and efficient care. Since 2018, our residency program has utilized a daily readiness huddle (key component of DMS) to prepare inpatient residents for their workday. This is a time when residents can raise administrative and/or clinical patient safety concerns. Concerns unable to be immediately resolved locally are designated as Quick Hits (QH) and escalated through residency and hospital leadership with resolutions cascaded back to frontline providers. With <10% of residents on inpatient services each month, a gap in overall resident awareness of findings from resolved QH exists, posing potential patient safety risks. OBJECTIVE/AIM: We aimed to improve the weekly percentage of findings from resolved QH communicated to every resident (rather than only those in attendance at the daily readiness huddle) from 0% to >95% within 6 months. METHODS: A core team was created consisting of residency program leadership (DIO, Program Directors, Chief Residents). Root causes were identified and guided interventions. Outcome measure was percentage of weekly QH communicated to all residents. Process measure was weekly QH identified for escalation. Findings of resolved QH were shared at bi-weekly residency program meetings/minutes. Plan-Do-Study-Act Cycles included: 1) Standardizing process of identifying QH requiring report-back to all residents, and 2) Audit and feedback to program leadership regarding transmission of resolved QH with adjustment in standard work when needed. Due to rarity of patient safety events, these were unable to be tracked. Run charts assessed improvement over time. RESULTS: Over 20 weeks, 83 QH were identified with 45 requiring escalation beyond residency program leadership for resolution including to physician safety officer and CEO huddles. Outcome measure showed sustained, special-cause improvement from 0% to 100% by Week 15 following Cycle #2 (Fig 1). Process measure remained unchanged at 4.2 QH averaged per week. CONCLUSIONS: Using improvement methodology, we were able to achieve sustained improvement above our goal of communicating findings of resolved QH to all residents. Audit and feedback appeared to have the greatest impact on our outcome measure. Further study is needed, but this closed-loop communication process may also provide beneficial impacts to patient safety.
-

Memory T Cell Populations in Human Leukemia
Sara McElroy, Fang Tao, John Szarejko, and John M. Perry
Background Incorporating the immune system into cancer management is an area of robust research. Treatment modalities aimed at activating cytotoxic T cells against malignancies include immune checkpoint inhibitors, bispecific T-cell engagers, and chimeric antigen receptor (CAR) tumor-specific T cells. Most anti-cancer T cell research is narrowly focused, but knowledge about the nature of diverse sub-populations of T cells in cancer, particularly memory T cells, is vital prior to potential incorporation into therapies. T memory stem cells (Tscm) are of interest due to their longevity and powerful abilities of self-renewal and creating the full spectrum of memory CD8+ T cells, including central memory (Tcm) and effector memory cells (Tem). Objective To determine potential presence and frequency of memory T cell populations in human leukemia at diagnosis and after induction chemotherapy. Design/Method Children’s Mercy Cancer Center Biorepository provided samples from 16 patients with premature B cell acute lymphoblastic leukemia (pre-B ALL) from peripheral blood (PB) and/or bone marrow (BM). Timepoints were diagnosis and day 29 (D29) of induction chemotherapy. Flow cytometric analysis of cytotoxic memory T cell populations was performed and analyzed using descriptive statistics and the t-test. Results Despite sample variability, the absolute cell counts were not significantly different. The live cell percent was lower at diagnosis than D29 (PB- 57.2% vs 79.4%, p=0.001; BM- 41.7% vs 77.0%, p<0.001). T cell frequencies were lower at D29 (PB- 14.8% vs 5.74%, p=0.014; BM- 9.5% vs 5.9%, p=0.217). CD4+ and CD8+ T cells were not significantly different between diagnosis and D29. Among CD8+ T cells, naïve cells markedly increased from diagnosis to D29 (PB- 53.6% vs 82.2%, p < 0.001; BM- 38.8% vs 80.3%, p < 0.001) with a corresponding significant decrease in Tem (PB- 15.1% vs 4.2%, p=0.002; BM- 21.6% vs 4.7%, p < 0.001). Tscm (reported as a % of CD8+ T cells) were detected in all samples at diagnosis (PB range- 0.49-12.2%; BM range- 0.12-4.4%). After induction, two patients had no Tscm detected. The remainder demonstrated varying numbers of Tscm (PB range- 0.038-23.4%; BM range- 0.013-17.4%). Differences between diagnosis and D29 were not significant; however, percentages of Tscm were lower in 9 of 12 patients after chemotherapy. Conclusion Induction chemotherapy led to decreased differentiated CD8+ T cells with recovery of mostly naïve cells by D29. Furthermore, we established the presence of Tscm in most pediatric pre-B ALL samples. The decline of Tscm in most patients requires functional analyses to determine their role in leukemia and potential for use in immunotherapy.
-

Oligodontia, Mandibular Hypoplasia and Microglossia in Pediatric Patients: Review of the Literature and Report of a Case
Gage Williams, Robin Onikul, Jenna Sparks, Neena Patel, Amy Burleson, and Brenda S. Bohaty
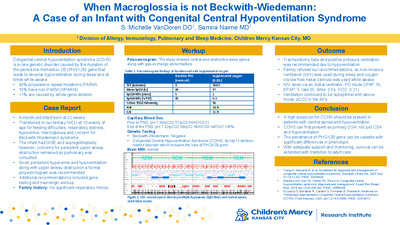
Introduction: The combined findings of oligodontia, mandibular hypoplasia and congenital malformation of the tongue (hypoplasia) is relatively rare in children. This presentation discusses the case of a 6-year-old female patient who presented to the dental clinic at The Children’s Mercy Hospital in Kansas City, Missouri for emergent care secondary to gross dental caries. Additional findings at the initial visit were that of oligodontia, microglossia, micrognathia, and mandibular hypoplasia. A review of the medical history indicated that due to the physical anomalies noted at birth, a genetic microarray was completed indicating some variants of unknow clinical significance. As these forms of pathology uncommonly present without a connection to a specific syndrome, further genetic evaluation is warranted. This presentation reviews the clinical findings noted in the case, potential treatment options for future care and the importance of appropriate collaborative care with other medical professionals.
-

Recurrent Primary Spontaneous Pneumothorax Masquerading as a Congenital Pulmonary Airway Malformation in a Young Female
Chandra Swanson, Justin Sobrino, Tolulope A. Oyetunji MD MPH, and Erin Khan
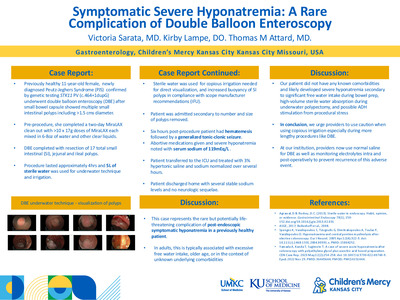
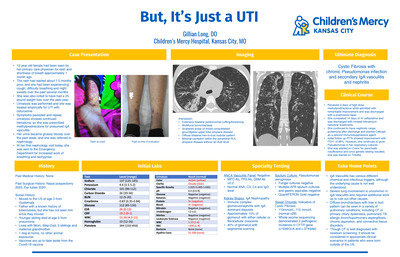
Introduction: Spontaneous pneumothoraxes in children are uncommon, may be idiopathic or associated with underlying pulmonary disease, and can present management challenges. We present a 12-year-old female with recurrent right sided spontaneous pneumothorax in the setting of an asymptomatic SARS-Co-V2 (COVID) infection and imaging concerning for congenital lobar overinflation (CLO) versus congenital pulmonary airway malformation (CPAM), prompting surgical intervention. Case: A 12-year-old pre-menstrual female with remote history of eczema, asthma, and environmental allergies presented from an outside facility with four-days of progressive chest pain and dyspnea on exertion and diagnosis of right-sided spontaneous pneumothorax, improving after pigtail chest tube placement. Physical exam was significant for tall thin body habitus; family history was significant for paternal spontaneous pneumothorax as an adolescent. She was incidentally found to be COVID positive. Chest plain films (CXRs) showed subcutaneous emphysema and persistent right-sided pneumothorax. Clamping trial failed, prompting removal of the pigtail and placement of 12F chest tube with resultant near complete re-expansion. On serial CXRs, a right hilar cystic lucency was newly identified. Chest CT confirmed the right upper lobe (RUL) air-filled cystic structure and abrupt narrowing of the RUL posterior segmental bronchus, concerning for CLO versus CPAM. Chest tube was successfully removed on day 6, and she was discharged home with planned follow-up. Three months later, she was readmitted for recurrent right-sided spontaneous pneumothorax diagnosed after one day of chest pain, cough, and dyspnea. Laboratory testing revealed mild leukopenia and anemia; she was COVID negative. A chest tube was placed and set to wall suction. Due to persistent pneumothorax, this was replaced with a pigtail drain on day 5. CXRs demonstrated persistent cystic RUL lung mass. With her prior COVID infection now resolved, RUL wedge resection was completed via video-assisted thoracoscopic surgery on day 8. She tolerated the procedure well and was discharged on day 10 with resolving pneumothorax. Tissue for pathology results revealed pleural fibrosis and focal hemorrhage without malignancy, most consistent with a ruptured bleb. At one week follow up, she remained stable without complications. Discussion: Pneumothoraxes in tall, thin adolescents are often categorized as primary spontaneous. Most pneumothoraxes resolve with conservative management and often do not require surgical intervention. Congenital lung malformations are a rare secondary cause in children and may be detected on CXR. Chest imaging should be carefully reviewed for congenital malformations requiring specific surgical intervention. These findings, along with the patient’s clinical course, may assist in determining management.
-

Sedation Services Offered at Pediatric Dental Offices in the United States as Reported on Publicly Available Practice Websites
Stefanie Curtis, Jane Witt, Brenda S. Bohaty, Robin Onikul, Amy Burleson, Jenna Sparks, and Neena Patel
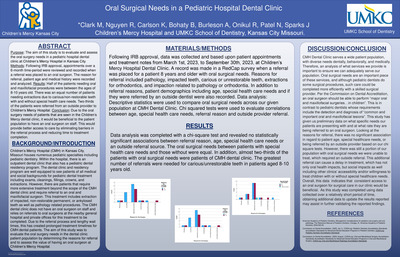
Background: As early childhood caries impacts children throughout the United States, restorative dental procedures are often needed. The literature indicates that due to a variety of factors, parents may research their child’s dental condition and try to find options for care that they perceive as least traumatic for their children. These options frequently include sedation and general anesthesia. This background research is typically completed via the internet on public websites. Purpose: The purpose of this investigation was to identify if information regarding specific types of sedation/anesthesia services offered by pediatric dental providers are available on practice websites and to determine if the type of information available differed depending upon practice location. Methods: Pediatric dental practices based in states located in Northeast, Southwest and Western districts as delineated by the AAPD were included in the study. Practices were identified using the ABPD webpage as practices with Board Certified Pediatric dentist practitioners. Specific information regarding the availability of oral conscious sedation, IV sedation, and general anesthesia were assessed and analyzed using descriptive statistics. Results/Conclusions: A total of 432 pediatric dental practice websites were evaluated. 34% of websites analyzed were from the Southwestern district, 30% from the Northeast district and 36% from the Western district. While the majority of all public websites analyzed either did not mention specifically which types of sedation were offered or were unclear about the information, there were however, some statistically significant differences among regions in regard to the type of information available.
-

Treatment of Recurrent Wilms Tumor with Irinotecan/Temozolomide
Meagan Vacek and Terrie Flatt
Background: Despite improvement in relapse free survival (RFS) in recurrent Wilms tumor, the 4-year RFS rate for patients treated with vincristine/dactinomycin/doxorubicin is approximately 40%. Ifosfamide, carboplatin and etoposide are commonly used in relapsed solid tumors, but have significant toxicities and require hospital admission for administration. Our patient focused on quality of life, and this led to exploration of other treatment options. Objective: Describe a case of multiply relapsed Wilms tumor with management on oral irinotecan/temozolomide for improved quality of life and remission for almost 1 year. Design/Method: Case Report Results: The patient is an 11-year-old female diagnosed with Wilms tumor at 6 years of age in Honduras who received approximately 6 months of chemotherapy with Vincristine and a nephrectomy. Staging in Honduras was unknown. Due to financial difficulties, she was unable to continue treatment and family immigrated to the United States. One year after initial diagnosis, imaging revealed large chest mass and intracardiac masses. Biopsy confirmed recurrent Wilms and she received modified NWTS/AREN0534 regimen. Patient responded well to this regimen and then underwent surgical resections and whole lung radiation. At 20 months off therapy, she was found to have a lung nodule, confirmed to be recurrent Wilms tumor. As this was her second recurrence, both patient and family chose a chemotherapy regimen allowing for the best quality of life. She received Irinotecan 90mg/m2/dose PO on days 1-5 and Temozolomide 40mg/m2/dose PO on days 1-5, 8-12, 15-19. She received the 2-drug regimen for 10, 28-day cycles without toxicities or hospitalizations, allowing her to attend school. At the end of cycle 10, she had a third recurrence. Irinotecan is a camptothecin prodrug shown to have activity against adult solid tumors. Topotecan of the same drug class also showed activity in children with favorable histology Wilms tumor with a 48% response rate in heavily pretreated patients. Temozolomide (TMZ) has activity against adult solid tumors with promising results in xenograft models of pediatric solid tumors. O6-methylguanine-DNA methyltransferase (MGMT) is a DNA repair enzyme which inhibits the anti-tumor effect of alkylating agents, like TMZ. Negative MGMT protein expression increases the sensitivity to alkylating agents and can predict the response to temozolomide. Our patient was MGMT negative. Conclusion: Irinotecan/Temozolomide should continue to be explored as an option for relapsed/refractory solid tumors as it can achieve remission for a substantial period while allowing for improved quality of life.
-
 presenting with spontaneous necrosis and Clostridium perfringens co-infection by Ronald Palmen, Abbey Elsbernd, Kristin Palmen, and Kathyrn Kyler")
Wilms Tumor (WT) presenting with spontaneous necrosis and Clostridium perfringens co-infection
Ronald Palmen, Abbey Elsbernd, Kristin Palmen, and Kathyrn Kyler
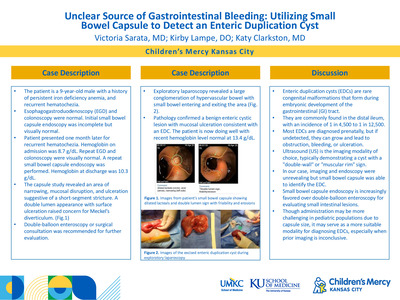
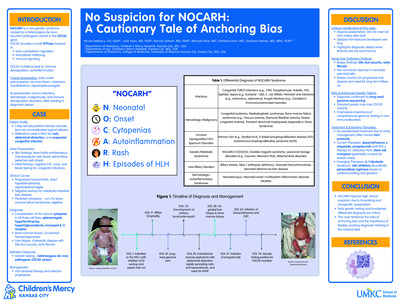
Wilm’s Tumor (WT) is the most common renal malignancy of childhood. The initial presentation of WT may mimic infection or other malignancies with nonspecific symptoms including fever, abdominal/flank pain, or hematuria. We describe a case of WT with spontaneous necrosis obscured by overlying Clostridium perfringens infection. A previously healthy 5-year-old girl presented to the emergency department with a two-day history of flank pain and fevers. She was tachycardic (130 bpm), hypertensive (116/75), and febrile (101.7F). Her abdomen was distended with left-sided flank tenderness without a palpable mass. Initial laboratory testing revealed elevated CRP (70mg/dL) and leukocytosis (22.56 x 109 /L). Urinalysis showed 5-10 WBCs but was otherwise normal. A CT abdomen/pelvis with contrast demonstrated a mass-like structure in the left upper quadrant, surrounding and splaying the left adrenal gland with inferior displacement of the left kidney. The patient was hospitalized for evaluation and received empiric ceftriaxone. Additional laboratory studies were obtained including urine cultures, plasma normetanephrine and metanephrine levels, as well as Vanillylmandelic Acid (VMA) and Homovanillic acid (HVA) levels. All were within normal limits. Her symptoms, leukocytosis and CRP improved with resolution of fevers after 5 days. Given the ambiguous clinical picture favoring infectious versus oncologic diagnoses, open surgical biopsy of the left kidney and surrounding mass was performed. Pathology demonstrated a phlegmonous appearance of the left kidney and fibrovascular proliferation with inflammation and no evidence of malignancy. Tissue cultures were positive for Clostridium perfringens. At discharge, the patient transitioned to a 10-week course of cefixime for C. perfringens kidney infection with outpatient follow-up. Repeat CT abdomen/pelvis obtained 4 weeks after discharge demonstrated decreased size of the renal mass. In outpatient follow-up, repeat ultrasounds minimally improved, therefore a second renal biopsy was obtained 13 weeks after discharge. The biopsy identified monomorphic small cells in varying stages of cell death with positive WT1 protein, consistent with WT. This case features an unusual presentation of WT with spontaneous necrosis and concomitant C. perfringens infection. Our patient’s presentation was suspicious, however her initial negative biopsy was masked by the presence of secondary bacterial infection and necrosis, leading to delayed oncology referral and treatment. This case underscores the importance of avoiding confirmation bias in the setting of ambiguous clinical presentations. WT may mimic other pediatric renal pathologies clinically and radiologically, such as renal hemorrhage, abscess, or other malignancies. This poses a diagnostic challenge for providers, particularly when both infection and malignancy are observed.
-

17-year-old ballet dancer with 4 years of right upper extremity pain
Mariah Sisson and Brian S. Harvey
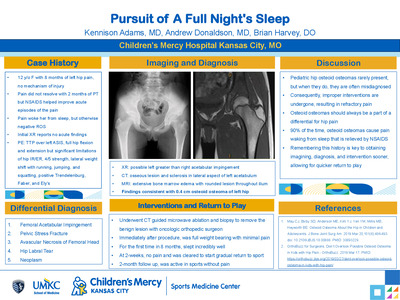
History:No known injury. Intermittent, dull, radiating. Starting at the shoulder and moving to the medial elbow, but sometimes only at the medial elbow with numbness of the 4th/5th digits. No limitations in ballet. Extended course to see Sports Medicine. PCP - failed treatment for herpetic whitlow, referred to dermatology. Dermatology - bilateral Raynaud's syndrome & Pernio, referred to rheumatology. Rheumatology - having RUE numbness, referred to neurology & PT. Neurology - tenderness to palpation at the anterior shoulder, referred to Sports Medicine. PT - getting stronger, but symptomatically making minimal improvement. PE:Cardiac: capillary refill normal. MSK: RUE: Inspection: No erythema, edema, or bruising. Lower trapezius wasting visible when examining back/scapula. Palpation: Tenderness at medial epicondyle but not same pain she has previously experienced. No tenderness to palpation throughout remainder of RUE. ROM: Full ROM without pain or numbness. Strength: Normal strength. Special Tests: Spurling's negative, Roos negative, Adson's positive with loss of palpable radial pulse. Differential:Thoracic Outlet Syndrome, Cervical Neuropathy, Right Shoulder Tendinopathy, Scapular Dyskinesia, Medial Epicondylitis. Discussion:Initial presentation was interesting with overall non-specific symptoms and many specialists who had new findings, including bilateral Raynaud's syndrome. Patient was unable to truly localize if the pain was from her neck, shoulder, or elbow, but endorsed pain at times in all these locations and had no symptoms on day of clinic visit. It wasn't until the positive Adson's test that the diagnosis started to become clearer, or at least moved thoracic outlet syndrome to the top of the differential diagnosis. Concern for thoracic outlet syndrome guided further management.
-

A rare cause of elbow pain with a controversial name
Thomas Munro and Brian Harvey
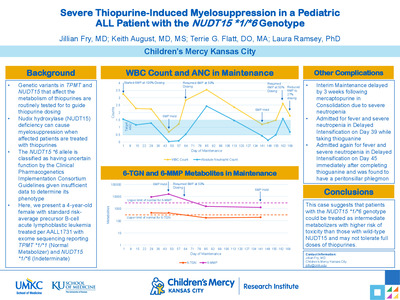
History: 13-year-old right hand dominant male presenting with 1-year concerns of bilateral elbow locking, popping, and pain. Right elbow tends to be affected more frequently than left. Patient states that at random, when he is trying to extend at the elbow joint, his elbows will "lock up". He will not be able to extend past this region and has significant pain when this occurs. He has to proceed back into elbow flexion and again try to "push through" into full extension. This will result in a loud pop followed by about 5-10 minutes of pain which slowly resolves. This happens typically once a day for about 4 days out of the week. He denies any mechanism of injury and specifically denies any previous elbow contact injuries. He is in 8th grade and participates in baseball, basketball, and tennis. Physical Examination: Constitutional- Well-developed well-nourished. MSK: Bilateral Elbow. Neuro- sensation intact in the distal UE bilat Vascular- 2+ pulses in upper/lower extremity. Inspection - no swelling, bruising, erythema or skin changes. Palpation: -Non-tender: medial/lateral epicondyle, radial head, olecranon, triceps. - Tender: Radio-capitellar Joint, Flexor-Pronator Complex, Extension-Supination Complex. Range of motion of the elbow -Normal: flexion, extension, pronation, supination. Strength- normal elbow flexion, elbow extension, wrist flexion, wrist extension, pronation/supination. Special Testing Test: Valgus- no pain, Varus- No pain, Moving Valgus- no pain, Tinel's test negative Differential Diagnosis: 1. Capitellar OCD 2. Panner disease 3. Loose bony fragment in the joint space 4. Repetitive elbow subluxation 5. Arteriovenous malformation Tests & Results: After obtaining history and completing the physical exam bilateral elbow x-rays were ordered. X-ray read from radiology showed No fracture or dislocation involving the bilateral elbows with clinical overread and physical exam correlation showing concerns for possible trochlear OCD lesions bilaterally. MRI was obtained showing mild so called fishtail deformities of the bilateral humeri. Final/Working Diagnosis: Hegemann's Disease (post-traumatic disturbance of the epiphysis of the humeral trochlea). Discussion: Hegemann's Disease is a rare diagnosis. It presents with elbow pain, locking sensation, decreased range of motion, and sometimes swelling. A discussion has begun on whether this diagnosis would more properly exists on the same playing field as the rare but more well-known, fishtail deformity. The etiology of both have been postulated to be secondary to disruption of the vulnerable vascular supply of the trochlea. It has been proposed that these two diagnoses be lumped together and more accurately termed post-traumatic disturbance of the epiphysis of the trochlea. Our patient providers another example of such a deformity without a clear inciting injury. It is unique in its bilateral nature. Outcome: This patient was instructed on activity modification (held from sport and instructed to avoid throwing and arm weight-bearing activities) and began formal PT. The rarity of this disease lends to the lack of a consensus treatment though some form of activity modification seems to be common. Return to Activity and Follow-Up: Patient has yet to return to full activity and is continuing physical therapy. In our patient it is possible that if vascular supply recovers before closure of the physeal plate, the injury will remodel into a normal trochlea but could also still ultimately develop a fishtail deformity.
-

Caregiver Mental Health Screening in a Pediatric Feeding Clinic
Dana Bakula, Laura Slosky, Kelsey Dean, Ann M. Davis, and Sarah T. Edwards
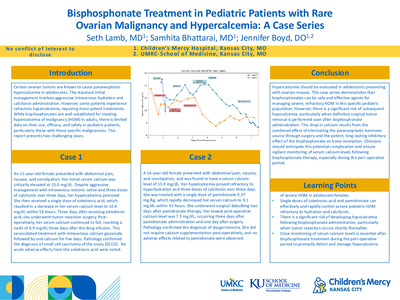
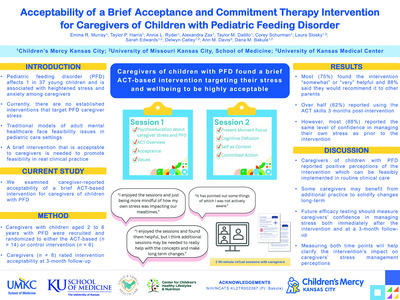
Introduction: One in four adults have mental health (MH) problems. Caregivers of children with feeding problems are at even higher risk for mental health (MH) problems, including depression, anxiety, and posttraumatic stress. Caregiver MH concerns have a negative impact on caregiver and child quality of life and are specifically linked to suboptimal child feeding practices. Thus, it is critical to identify caregiver MH problems in pediatric feeding settings. However, it can be challenging to comprehensively screen for caregiver MH in a busy pediatric feeding clinic. This emphasizes the importance of a feasible and brief method for screening caregiver MH. Methods: From 2019-present our multidisciplinary feeding clinic has been administering a 2-item caregiver MH questionnaire to caregivers presenting for a new visit with their child. The questionnaire asks if one or more of the primary caregivers in the home has a MH problem, and what the problem is. We descriptively evaluated these screenings compared to base rates in the literature. Results: Caregivers of 327 children were screened, and 40% of caregivers endorsed at least one caregiver in the home had a mental health problem, such as depression, anxiety, or PTSD. Among caregivers of children under the age of one year, 45% of caregivers reported MH problems (many of which were post-partum depression and anxiety). These data are in line with rates observed in the literature, indicating that roughly 40% of caregivers of children with feeding problems have MH problems. Conclusions: This two-item screener shows promise in identifying caregiver MH problems, as positive screens were similar to observed rates in the literature. However, additional research is needed to evaluate sensitivity and specificity of this measure. Although not a perfect screener, this two-item screener was quite feasible to implement, as it easily integrated into new visit paperwork. Caregivers who screen positive meet our team social worker and/or psychologist to discuss their MH concerns and connect caregivers with resources. More research is needed to refine best practices in caregiver MH screening in pediatric feeding settings. Further, given these high rates of MH problems, point of care interventions to address caregiver MH in clinic would be ideal, and would reduce barriers to seeking care in the community. This may be particularly important for caregivers of infants, given high rates of postpartum MH problems.
-

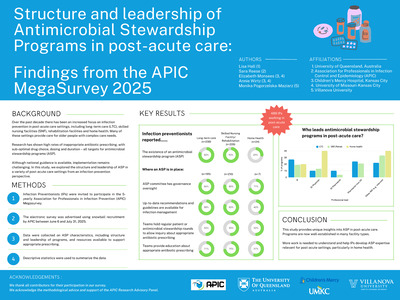
Healthcare Needs and Experiences of Detained Youth
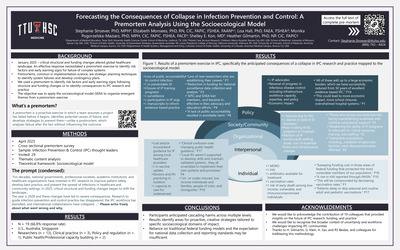
April McNeill-Johnson, Zuri Hudson, Brittany Moore, Dumebi Okocha, Megha Ramaswamy, and Kimberly A Randell
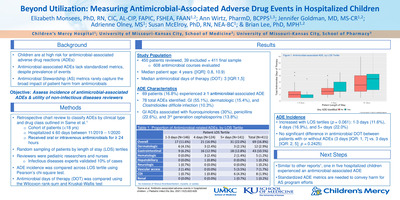
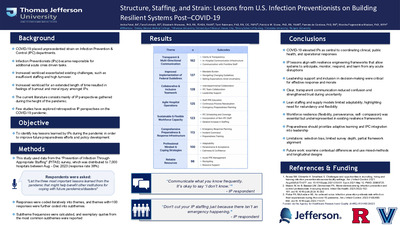
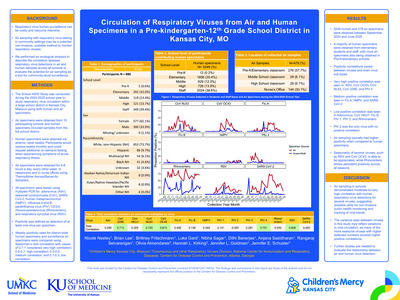
COVID-19 : Perspectives from Youth in Detention Background: The COVID-19 pandemic amplified health disparities among youth in detention. Understanding perspectives of these youth on the pandemic and COVID-19 vaccination may identify strategies to mitigate pandemic-related health disparities in this group. Objective: To explore perspectives on the COVID-19 pandemic, effect on detention experience & the COVID vaccine among youth in detention. Methods: This is a secondary analysis of a study examining healthcare needs and experiences of youth in detention. We recruited a convenience sample of youth (14-17 years) detained in urban midwestern juvenile detention centers from January-November 2021. We conducted semi-structured individual interviews & used a thematic analysis approach to code interview transcripts, after which codes were consolidated into themes. In early interviews, participants spontaneously discussed the COVID-19 pandemic, prompting addition of interview questions to further explore this. Participants completed an anonymous demographic questionnaire at the conclusion of the interview. Results: 15 youth (Table 1) discussed COVID-19 to date, with interviews ongoing. Youth had varied opinions on the gravity of the pandemic. Most thought that COVID-19 was a significant issue, but some felt the pandemic was fictitious. Youth obtained information primarily from family, friends, social media, and commercial news sources. Most youth voiced that they would not get the COVID-19 vaccine. Many expressed general distrust of the vaccine. Concerns included the speed of vaccine development and implementation and misconceptions about how the vaccine works. Some also felt they are immune to COVID-19 due to their youth and health. Among those who were vaccinated, parental preference and personal gain (i.e., travel, sport participation) drove vaccination acceptance. Youth suggested targeted educational strategies to increase youth vaccine uptake. Youth described negative impacts of the pandemic on their detention experiences. Visitation was limited with bans on personal touch, halts placed on packages being delivered from the outside community, and a 10-day quarantine was mandated at detention entry. See Table 2 for illustrative quotes. Conclusions: Youth in detention have varied perspectives on the gravity of the COVID-19 pandemic. Vaccine misconceptions and perceived lack of vulnerability to COVID-19 contributed to vaccine hesitancy. Vaccine uptake by youth in detention may be improved by partnering with parents, highlighting personal gain, and youth-targeted education.
-

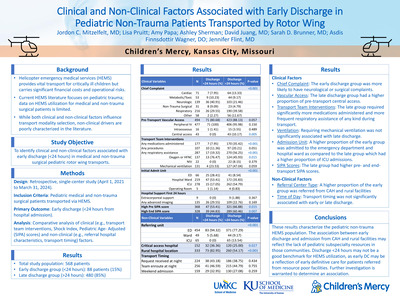
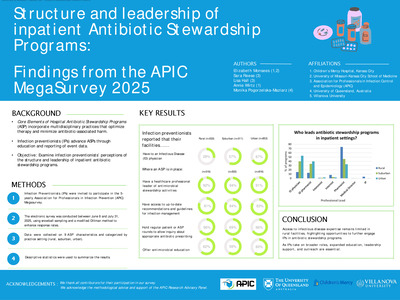
Identifying Predictive Factors for Patients Transferred From Floor to PICU within 24 hours of Admission by a Pediatric Critical Care Transport Team
Gina Patel, Lisa Carney, Brian S. Olsen, and Jennifer Flint
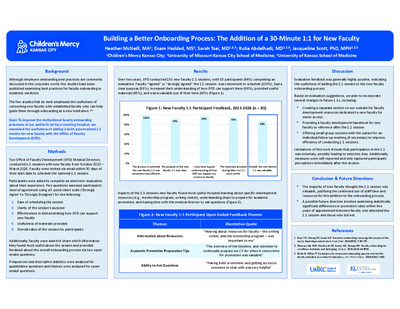
Abstract Objectives: Appropriate triage and disposition during transport can reduce the need for unplanned transfers to the pediatric intensive care unit (PICU) within 24 hours of admission. The pediatric early warning score (PEWS) is utilized to monitor for inpatient clinical deterioration and acuity during transport at our hospital. We sought to determine predictive factors of patients admitted to the inpatient ward who required PICU transfer within 24 hours following transport by Children’s Mercy Critical Care Transport (CMCCT) team. We hypothesized patients with respiratory illness and PEWS > 4 during interfacility transport are at higher risk of PICU transfer within 24 hours of admission. Methods: A retrospective, case-controlled chart review of 100 total transports by CMCCT between January 2018 - December 2020 was performed. We included patients 1 month to 18 years of age admitted to the inpatient ward with respiratory illness and excluded patients with congenital heart disease. PICU transfers within 24 hours were compared to the control group who did not require PICU transfer. Metrics from pre-transport, transport, floor and first 24 hours after PICU transfer were recorded into the Research Electronic Data Capture Database (REDCap). Results: PICU transfers had a median PEWS score of 4 [3,5, p= 0.036] compared to a PEWS of 3 [2,4, p= 0.036] in patients who remained on the floor. PEWS scores were grouped into green (0-2), yellow (3) and red zone ( > 4) based on our institutional floor protocol for multivariate analysis. A trend towards higher transport PEWS scores for PICU transfers within 24 hours was noted with 30/50 (OR 2.02, p= 0.141) having the highest transport PEWS in the red zone as compared to the control group but was not statistically significant. A trend towards higher admission PEWS for PICU transfers was also noted. A higher floor admission PEWS in the red zone was statistically significant for PICU transfer with 23/50 (OR 4.95, p= 0.001). There were no differences between the 2 groups related to prematurity (p= 0.795), home oxygen (p= 0.999), high flow nasal cannula (p= 0.262), or continuous beta agonist (p= 0.454). Patients transferred to the PICU did have lower weights (11.7, [7.8, 17.7], p= 0.09) compared to those who remained on the floor (median 14.7, [IQR 10.3,20.1], p = 0.09), however, this was not statistically significant. Conclusion: Our analysis showed a trend towards higher transport PEWS for patients who required subsequent PICU transfer but was not statistically significant, suggesting PEWS alone may not be a useful scoring tool to determine patient disposition during transport. A higher PEWS score after hospital admission on the general pediatric floor was associated with PICU transfer. Future directions should include additional study with larger sample sizes analyzing other risk factors or interventions during interfacility transport that might predict PICU transfer after admission to the floor.
-
 Study by Katherine L. Kurzinski, Yunwen Xu, Derek NG, Susan Furth, George Schwartz, and Bradley A. Warady")
Potassium Status in Pediatric Chronic Kidney Disease: A Preliminary Report from the Chronic Kidney Disease in Children (CKiD) Study
Katherine L. Kurzinski, Yunwen Xu, Derek NG, Susan Furth, George Schwartz, and Bradley A. Warady
-

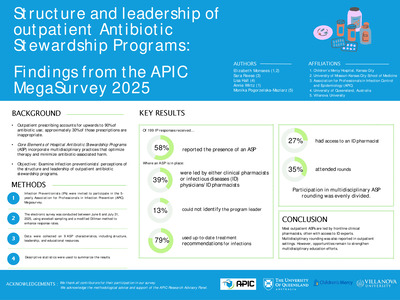
Rare variants in renal developmental genes and the risk of hypertension and CKD: a UK Biobank study
Benjamin Spector, Byunggil Yoo, Neil Miller, and Laurel K. Willig
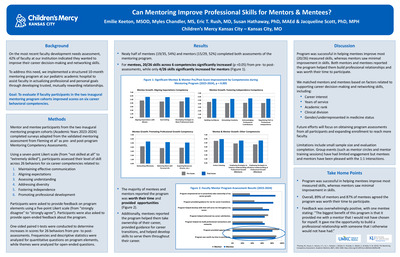
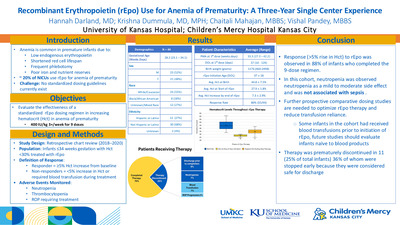
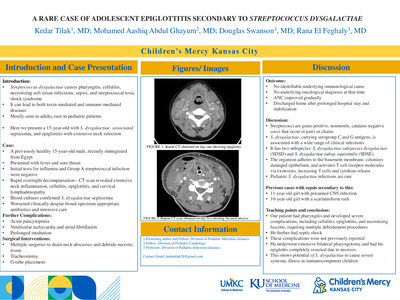
Background: Prior studies show chronic kidney disease (CKD) is heritable but only a few common variants have been associated with CKD and kidney dysfunction. Much of CKD heritability remains unknown and limited studies have explored the role of rare genetic variants in this missing heritability. Objectives: Identify rare genetic variants in renal developmental genes associated with hypertension and CKD. Methods: We examined the association between rare variants in 58 candidate genes from five renal developmental compartments and presence of CKD and elevated blood pressure (BP) in 49,989 individuals using whole exome sequencing and phenotypic data from the UK Biobank. Criteria for qualifying rare variants included a minor allele frequency < 0.1% and classification as pathogenic, likely pathogenic, or variant of uncertain significance (VUS) using in-house characterization software. Logistic regression models were generated for each compartment to determine the predictive ability of qualifying variants for the outcomes of elevated BP and CKD, with additional subgroup analysis by genetic ethnicity. Genes were selected for inclusion in regression models based on p < 0.25 using Chi-square univariate analysis. Genes included for each developmental compartment’s regression model are summarized in Tables 1 & 2. Results: Qualifying variants in 5 genes across 3 developmental compartments were significant predictors of elevated BP; qualifying variants in 4 genes across 4 developmental compartments were predictive of CKD. In subgroup analysis of individuals genetically identified as Caucasian, qualifying variants in 4 genes across 3 compartments were predictive of elevated BP; qualifying variants in 3 genes across 2 compartments were predictive of CKD. For individuals genetically identified as non-Caucasian qualifying variants in 3 genes across 2 compartments were predictive of elevated BP; qualifying variants in 6 genes across 2 compartments were predictive of CKD (Tables 1 & 2). The distribution of qualifying variant types (i.e. pathogenic, likely pathogenic, VUS) within genes containing rare variants predictive of disease were predominately VUSs (Figure 1). Conclusion: Rare variants in some renal developmental genes are associated with elevated BP and CKD and may help explain a portion of the missing heritability. However, the significances of variants differ by ethnicity, and the majority are classified as VUSs requiring further characterization.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}