
These posters have been presented at meetings in Children's Mercy and around the world. They represent research that was done at the time they were created, and may not represent medical knowledge or practice as it exists at the time viewers access these posters.
-

Development of a Kineisophobia Scale for Adolescents with Heart Disease: A Preliminary Analysis of Validity and Reliability
David A. White, Jami Gross-Toalson, Emily Cramer, Lindsey Malloy-Walton, Mollie Walton, Laura Martis, Brandy Enneking, Kelli M. Teson, Jessica S. Watson, Dara Watkins, and William R. Black
-

Identification of critical illness-related corticosteroid insufficiency after congenital heart surgery with next generation sequencing
Juan S. Farias, Nicholas Diehl, Lori A. Erickson, Jenny Marshall, Nataliya Kibiryeva, Kelly S. Tieves, Jorge Cross-Bu, and Jaime Silva-Gburek
Introduction: Critical illness-related corticosteroid insufficiency (CIRCI) which is characterized by relative inadequate cortisol levels in relation to increased demand during periods of severe stress is common after cardiac surgery and is a cause of hemodynamic instability. The purpose of this study was to identify possible genetic abnormalities related to CIRCI in pediatric patients after congenital heart surgery. Methods: Single-center retrospective study of neonates who underwent cardiac surgery between August 2018 to July 2020. We included patients who had obtained postoperative cortisol levels and next gen DNA-sequencing (NGS) as previous standard of care. Analysis methods are displayed in Figure 1. Results: Seven gene mutations were present in 75-100% of patients with CIRCI with a 0-25% incidence of those corresponding mutations in patients in the non-CIRCI group. The CIRCI group had 100% incidence of heterozygous gene mutation on STX1A with splicing and loss of function compared to 0% incidence in the non-CIRCI group. No differences were seen in demographics between both groups. The CIRCI group with STX1A mutation had lower cortisol level and longer intensive care length of stay. There were no differences in median mixed venous oxygen saturation and vasoactive inotropic score upon immediate postoperative admission, duration of mechanical ventilation, and hospital stay compared to the non-CIRCI group without STX1A mutation. Conclusion: Rapid testing for gene mutations, specifically STX1A, has the potential to detect patients at risk for critical illness-related corticosteroid insufficiency with hemodynamic instability. Further research in larger patient cohorts is required to determine the statistical and clinical significance of these genetic abnormalities.
-

Multi-disciplinary Collaboration And The Use Of Technology in The Reduction Of Cardiac Surgical Site Infections
Kelly Fehlhafer, Tiffany Mullen, Elizabeth Chang, Stacy Reynolds, Shannon Lysaught, Stephanie Doughty, and Jessica Nichols
-

Standard Atrial Epicardial Wire Placement Leads to Improved Atrial Signal Identification and Pacemaker Sensing
Nir Atlas, William Gibson, J Hermsen, A Harmon, J Torgeson, Lindsey Malloy-Walton, and N Von Bergen
Background: Atrial arrhythmias are common after pediatric cardiac surgery and are associated with increased morbidity and mortality. Atrial epicardial wires (AEW), utilized to diagnose and treat atrial arrhythmias, are known to malfunction during post-operative care. There are no pediatric prospective studies examining ideal placement of AEW. Methods: This prospective multicenter pilot study compared atrial amplitudes, pacing sensitivities and thresholds via AEW placed at Bachmann’s Bundle (BB) and the right-sided interatrial groove (RSIG) versus the surgeon’s standard placement (control locations) in 26 patients aged less than six years old undergoing cardiac surgery. Participants received four total AEW - two at the experimental locations (BB-RSIG) and two at control locations. An AtriAmp system was used to obtain an atrial ECG to calculate atrial and ventricular amplitudes. We documented pacing sensitivities and thresholds by connecting AEW to a temporary pacing box. We calculated descriptive statistics and used ANOVA test to detect differences across groups. Results: N=26 patients were represented. There were no demographic differences between hospitals. The combined mean patient characteristics at time of surgery included: age 3.2 yr (SD 3.6), weight 14.6 kg (SD 12.4), cardiopulmonary bypass time 111.8 min (SD 51.1). Within hospitals and combined, comparison of AEW characteristics showed greater atrial amplitude at BB-RSIG versus control locations (Table). Phrenic nerve capture was common during test pacing (n=13/26). Conclusion: This is the first prospective multicenter pediatric study to suggest that standard atrial wire site selection may improve atrial signals obtained from the atrial epicardial wires.
-

Treatment of Post-Operative Pain in Children with Severe Neurologic Impairment
Jordan Keys, Jessica L. Bettenhausen, Jessica L. Markham, and Matthew Hall
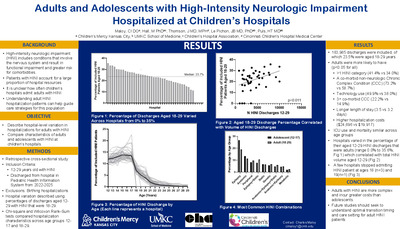
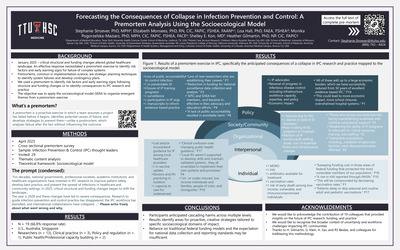
Introduction The assessment of pain in children with severe neurologic impairment (SNI) can be more challenging than in neurotypical children. Objective To describe: 1) the type, number of classes, and duration of post-operative pain medications for common procedures among children with SNI and 2) the variability in pain management strategies across children's hospitals, specifically for opioid administration. Methods This retrospective cohort study, using the Pediatric Health Information System database, included children aged 0-21 years hospitalized with SNI who underwent common procedures during 2019. We defined SNI using previously described high-intensity neurologic impairment (HINI) diagnosis codes and identified six common (>500 encounters) procedures among our population (e.g. fracture treatment, tracheostomy, spinal fusion, ventriculoperitoneal shunt placement (VP shunt), colostomy, or heart valve repair) using the clinical classifications software (CCS). Children excluded from this cohort did not undergo any of the six preselected procedures, had multiple procedures performed, or received an organ transplant. Medication classes were defined using the Classification of Palliative Care Pain Medications. Non-opioid medications were excluded from analysis to hone in on opioid administration. Clinical information was summarized using bivariate statistics. Results The cohort consisted of 7180 children; 65.9% had 1 HINI diagnosis, and 12.0% had 3 or more HINI diagnoses. The proportion of post-operative days with pain medications ranged from the least 28.8% (VP shunt) to the most 71.7% (spinal fusion). The number of classes of pain medications ranged from the least 0-1 (VP shunt) to the most 2-4 (Tracheostomy, Table 2). We observed notable variability in the use of opioids across hospitals (0-100% overall, p< 0.001) and by procedure (Range 0-100% across procedures, Figure 1.) Discussion/Conclusion Children with SNI experienced variability in the type, number of classes, and duration of all pain medications delivered post-operatively. This included an inconsistent use of opioids based upon hospital and procedure. Our findings indicate the need for both a standardized approach to the assessment of pain and post-operative pain management for children with SNI.
-

Prevalence of Iron Deficiency in Patients with Inherited Bleeding Disorders
Thomas Cochran, Brian R. Lee, and Shannon L. Carpenter
Background: Patients with bleeding disorders have greater propensity for blood loss and therefore may have a higher prevalence of iron deficiency (ID) when compared to the general population. However, current literature focuses on adolescent females and few studies have assessed the overall prevalence of ID in children with inherited bleeding disorders. Aims: This study aims to identify the prevalence of ID in children with an inherited bleeding disorder. Methods: A retrospective analysis of children with any inherited bleeding disorder seen in Children’s Mercy Hospital’s Hemophilia Treatment Center between 2010 and 2020 was performed. Iron deficiency was defined by recently published serum ferritin thresholds outlined by the National Health and Nutrition Examination Surveys. Results: There were 798 patients with inherited bleeding disorders who were included in this analysis. Of the 306 patients who had serum ferritin collected, 162 (53%) had ID. In patients who had ID, 68% were female and 48% were aged 6 to 15 years. Notably, of the 129 (26%) males with serum ferritin collected, 40% had ID. The proportion of patients who had ID in each age group is displayed in figure 1. Of the 757 patients who had blood counts measured, 346 (46%) were anemic. Of the patients with anemia, 232 (67%) were male. The proportion of anemic patients in each age group is displayed in figure 2. Conclusion: The prevalence of ID in children in our cohort is considerably higher than the 10% prevalence estimated in the general pediatric population. Prior epidemiologic analysis of ID and iron deficiency anemia is mostly focused on adolescent females. However, the high prevalence of anemia in males with inherited bleeding disorders suggests that they are at comparable risk. Considering only 24% of males had ferritin collected, it is possible that the prevalence of ID in males is higher than this report suggests.
-

Central Hypothyroidism Following Neonatal Graves' Presentation
Emily Metzinger and Kelsee Halpin
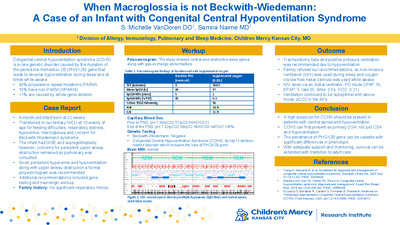
Background: Neonatal Graves’ disease is a rare disorder of neonatal autoimmune hyperthyroidism secondary to the transplacental passage of thyroid-stimulating hormone receptor antibodies. Although neonatal Graves’ disease is transient, it is associated with cardiac dysfunction, intrauterine growth restriction, prematurity, craniosynostosis, and developmental delay and can be life-threatening. Additionally, infants with neonatal Graves’ disease can rarely present with primary or central hypothyroidism later in infancy or childhood. This is suspected to be due to the disruption in the hypothalamic-pituitary-thyroid axis or development of the thyroid gland. Clinical Case: Here we describe a case of neonatal Graves’ disease that has been complicated by persistent central hypothyroidism requiring levothyroxine treatment. This was a preterm infant with tachycardia, biventricular heart failure, and hepatomegaly who was transferred to a higher level of care NICU for cardiac and respiratory failure. Pregnancy was complicated by history of maternal Graves’ disease status post radioiodine ablation. Maternal TRAB and thyroid levels were unavailable. Initial thyroid studies on DOL 1 were notable for suppressed TSH of <0.02mcIU/mL, elevated free T4 6.9ng/dL, and elevated total T4 >24.9mcg/dL. Total T3 was normal at 161ng/dL (50-452ng/dL) on DOL 2, and TSI was elevated at 4.8 (TSI Index, normal
-

Supporting Fathers and Partners in the NICU
Tiffany Gladdis
The NICU can be an incredibly stressful environment for both the infant and its parents. Unlike many traumatic events, the NICU experience can often feel like an ongoing trauma, with the stay often involving highs and lows, new diagnoses, changes in prognosis, multiple procedures, and a rollercoaster of emotions. Additionally, the NICU can also trigger trauma responses for parents who have had previous traumatic experiences. When working with families in the NICU, it is important to use a Trauma Informed Care lens to ensure that the whole family is understood and adequately supported (Sanders & Hall, 2007). Perinatal Mood and Anxiety Disorders (PMAD) can be a result of prolonged stress related to the trauma of the NICU experience. While much of the attention is often given to the infant and birthing parent, it is important to also consider the impact on the father or non-birthing parent. Both parents are susceptible to developing PMADs and this presentation will focus on the experience of the father or partner.
-

Bone Marrow Transplant For Macrophage Activation Syndrome In Systemic Juvenile Idiopathic Arthritis
Shailly Gaur, Michael J. Holland, J Allyson Hays, and Ibrahim A. Ahmed
7yo w/ systemic juvenile idiopathic arthritis who developed macrophage activation syndrome and interstitial lung disease non-responsive to steroids, immunosuppression, and directed biologics with significant adverse reactions who required chemotherapy and eventual bone marrow transplant leading to complete resolution of symptoms.
-

Clinical Course of a Patient With Agammaglobulinemia Caused by SLC39A7 defect
Thao Le, Emily Farrow, Alvin Singh, Isabelle Thiffault, and Nikita Raje
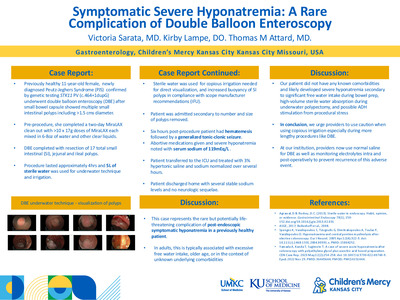
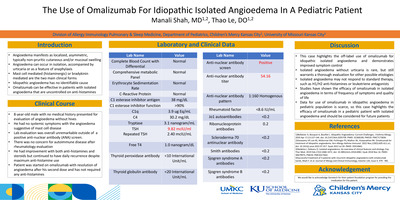
Case Report: A 10-year-old unimmunized boy initially presented to the hospital at 18-months of age with pneumonia and failure to thrive. He had multiple infections including Escherichia coli urosepsis, viral croup, chronic otitis media with bilateral ruptured tympanic membranes, and bacterial pneumonia. On physical examination, he was ill appearing and had diffuse crackles. His laboratory work-up showed leukocytosis, normocytic anemia, undetectable immunoglobulin (Ig) G, A, and E, low IgM (28 mg/dL), absent B cell with normal T cell (7800 mm3) and NK cell (527 mm3) counts, and low zinc level (63 mcg/dL). Genetic testing was negative for Bruton tyrosine kinase (BTK). Ig replacement therapy (IgRT) was initiated. Despite therapy he had persistent chronic rhinosinusitis and chronic cough. Computed tomography (CT) scan of the sinus and chest showed pansinusitis and bronchiectasis with mucoid impaction, predominantly in the lower left lobe. He was treated with inhaled corticosteroids and chest physiotherapy. He underwent functional endoscopic sinus surgery and bronchoscopy, which showed non-typeable Haemophilus. He was then treated with a course of Augmentin. He also consistently grew below the 3rd percentile while his mid-parental target height is close to the 50th percentile. He was started on growth hormone and has responded well. Exome sequencing showed compound heterozygous variants in the SLC39A7 gene encoding the zinc transporter, ZIP7. This leads to an autosomal recessive agammaglobulinemia-9, a primary immunodeficiency syndrome with recurrent bacterial infections associated with agammaglobulinemia and absence of circulating B cells. The family declined prophylactic antibiotics despite persistent infections. At 10 years of age, he continued to have worsening chronic sinusitis and bronchiectasis. A trial of prophylactic antibiotics with Amoxicillin was initiated. Discussion: Our patient is a 10-year-old male with compound heterozygous variants in SLC39A7 presenting with agammaglobulinemia, short stature, and bronchiectasis. He continued to have chronic recurrent sinopulmonary infections despite therapeutic IgG level on IgRT. Starting prophylactic antimicrobials earlier may be helpful in reducing lung injury and preventing infections
-

Clinical Presentation and Differential Diagnosis of a 10-year-old Presenting with Unerupted Maxillary Central Incisor: A Case Report.
Dev Patel, Robin Onikul, Amy Burleson, Brenda S Bohaty, Jenna Sparks, Neena Patel, and A Naidu
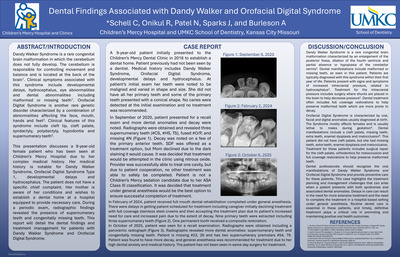
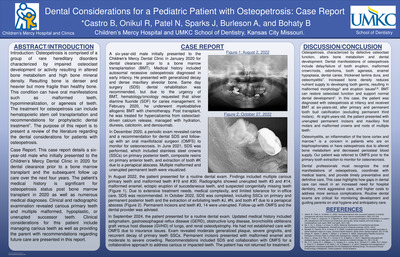
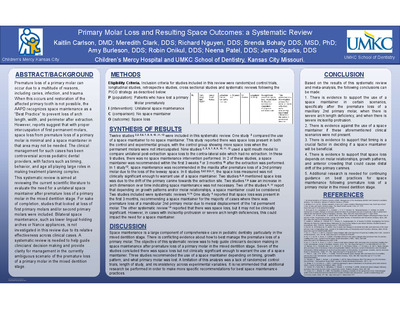
Delayed eruption of permanent teeth can be caused by numerous factors including nutritional deficiencies, tooth positioning, presence of supernumerary tooth, or presence of a cyst impeding eruption. The keys to identifying the cause of delayed eruption are good clinical and radiographic exam, along with obtaining a complete and accurate history from the patient and parent. This case report details a 10-year-old female presenting to the Children’s Mercy Kansas City Dental Clinic with chief concern for an unerupted upper anterior tooth. The patient’s medical history is noncontributory, and she has no known allergies. This case report will include the patient’s clinical and radiographic exam, differential diagnosis, and appropriate referral for definitive care.
-

Comparative Study of Pain Perception with Use of Vibration and/or Cold Stimulation Applied During Local Anesthetic Delivery in a Dental Setting: A Systematic Review
Tara Craven, Gage Williams, and Brenda S Bohaty
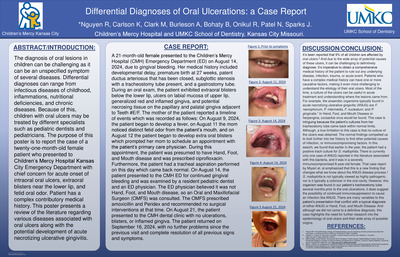
Delivery of local anesthetic can be one of the most difficult parts of the procedure for pediatric patients undergoing dental treatment and can prevent the child from being able to cooperate for treatment as well as instill anxiety for future visits.1 Several methods can be utilized to help mitigate pain control during the local anesthetic injection including behavior management, vibration, cold sensation, warming the anesthetic, and topical anesthetic.4 These methods are essential to helping the child have a good experience and ultimately be able to tolerate treatment for caries management and a long term positive view of the dentist. One technique that has been previously researched is the use of vibration and cold stimulation when delivering local anesthetic. Vibration and cold stimulation can block the afferent pain fibers (A delta and C fibers), an idea based on the gate control theory, thus reducing pain.11 These two methods, cold stimulation and vibration, can be especially advantageous for a pediatric population because they are both non-invasive. This systematic review is aimed at reviewing randomized control studies to evaluate the efficacy of using vibration and/or cold stimulation devices while administering local anesthesic in order to lower pain perception and dental anxiety. Several modern devices have been invented to introduce vibration and/or cold stimulation that can be utilized during dental treatment however, research on these devices is limited. Additionally, a systematic review is needed to guide further research as well as a proposed design study to further evaluate the efficacy of using vibration and/or cold stimulation during local anesthetic delivery.
-

Drug metabolizing enzymes and transporters may help determine effective budesonide dosing in EoE
Laurie McCann, Lisa Harvey, Norah Almahbub, Wendy Y. Wang, Erin C. Boone, Janelle R. Noel-Macdonnell, and Rachel Chevalier
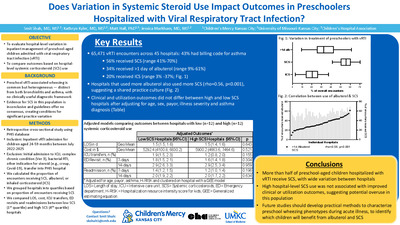
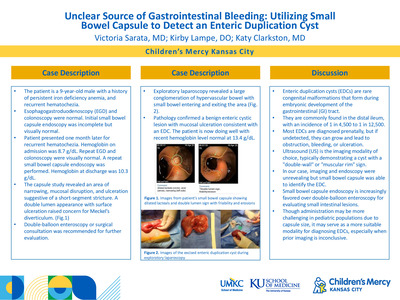
Background: Eosinophilic esophagitis (EoE) is a chronic inflammatory disorder diagnosed in children with painful or difficult swallowing, vomiting, or poor weight gain. Current treatment models adopt a trial-and-error approach in regard EoE treatment, including restrictive elimination diets, proton pump inhibitors, and topical budesonide. This approach can delay effective treatment which increases risk of disease progression and increases medical costs to families for frequent clinic visits and endoscopy. Objectives/Goal: The objective of this study is to determine the CYP3A5 genotype and expression of patients with eosinophilic esophagitis to discover which patients will respond to standard dosing of topical budesonide treatment (1, 2). Budesonide is a known drug substrate of CYP3A5 protein and single polymorphic changes are known to affect drug metabolism. By determining the CYP3A5 genotype, we aim to correlate treatment response to topical budesonide treatment, leading to more targeted and individualized dosing of budesonide. Allelic variant *1 (wild-type) has shown high substrate metabolism (1). Allelic variant *3 (most common), *6 , *7 have shown reduced substrate metabolism (1). The ultimate goal of this study is to aid in the development of a simple serum test to check a patients’ CYP3A5 genotype at the time of EoE diagnosis, prior to initiation of topical budesonide. Methods/Design: This is a single center retrospective study ongoing at Children’s Mercy Hospital in Kansas City, Missouri using serum and esophageal tissue samples from the already established, ongoing Gastroenterology Repository for Information in Pediatrics biorepository (GRIP) from patients <20 years>old, enrolled from 8/1/2017 to 11/1/2022. For this interim analysis, we had samples from 22 patients for genotyping and mRNA extraction. Digital droplet PCR (ddPCR) was used for mRNA quantification. Results: Of the 22 samples, nineteen had *3/*3 CYP3A5 alleles (86.3%), two had *1/*1 alleles (9%), and one had *1/*3 alleles (4.5%). CYP3A5 ratios were performed, and the initial results of this small sample size so far show that expression does not vary between genotype. Compared to CYP3A4, there is more CYP3A5 expression in the esophagus than CYP3A4, as noted in prior studies in adults. ddPCR was able to successfully measure CYP3A5 expression in esophageal biopsies confirming this as a valuable tool to quantify mRNA in these small tissue samples. Conclusions: These initial results are consistent with already published data and will help lay the groundwork for larger, more in-depth studies. We anticipate more data forthcoming, as the collection of consented patients is ongoing. Future, larger prospective studies are needed to further propagate the development of precision therapeutics of budesonide in EoE patients.
-

My Global Health Experience - Eldoret, Kenya
Megan Carroll
Describes her experience in Eldoret as a 4th year medical student.
-

Practicing Pediatrics in Lake Atitlan, Guatemala
Chandra Swanson
Describes her experience working in Lake Atitlan, Guatemala.
-

Solitary Median Maxillary Incisor and Holoprosencephaly: A review of the literature
Benjamin Olson, Robin Onikul, Amy Burleson, Brenda S. Bohaty, Jenna Sparks, and Neena Patel
A solitary median maxillary incisor (SMMCI) is a rare anomaly that affects approximately 1:50,000 live births. The presence of an SMMCI tooth may be an isolated finding or may be associated with other anomalies such as Holoprosencephaly (HPE). Early recognition of SMMCIS is important given the possibility of other associated findings that may impact pediatric growth and development. The purpose of this clinical case is to report the clinical findings associated with a nine-month-old patient who presented to our clinics with a primary solitary median maxillary incisor and a diagnosis of HPE. This presentation will review the literature regarding the medical and dental findings associated with HPE and will discuss strategies for appropriately diagnosing and managing care for such patients.
-

Who’s my child’s main doctor? Caregiver Perceptions of Teaching Teams
Jonathan Ermer, Shelby Chesbro, Jessica Boerner, Jacqueline M. Walker, and Joy L. Solano
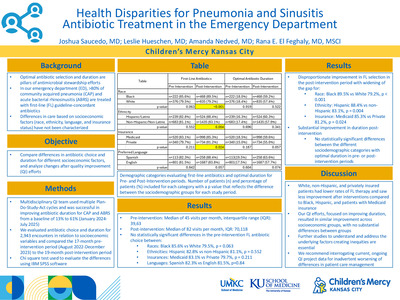
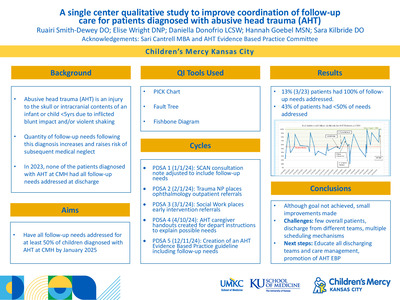
Background: At academic medical centers, children are cared for by large medical teams consisting of multi-level learners including medical students, interns, senior residents and fellows on patient-and family-centered rounds (PFCR). The size and structure of these teaching teams can make it difficult for patients and families to know who is caring for them and establish a trusting relationship. Also, research has shown when residents are perceived as a “team leader,” they learn more. Previous literature in adults has shown that patients often perceive the intern as their “main doctor,” but this has not been studied in pediatrics. Objective: We sought to identify who caregivers identify as their child’s main doctor and recorded the frequency of caregivers who identified the presenter (medical student or intern) as their child’s main doctor. Additionally, we described the frequency of caregivers who were aware that their child was going to be cared for by a large team of doctors at different levels of training. Methods: We conducted a single-institution prospective cohort study using a convenience sample of caregivers admitted to the hospital on pediatric hospital medicine teaching teams that conduct PFCR. After a rounding encounter, we surveyed caregivers who speak English or Spanish. Masked photos of all team members were provided to caregivers when asked to identify the child’s main doctor and the leader of the team. For each patient with permission from the caregiver, we recorded the number of prior admissions, active consultants during the current admission, and number of complex chronic care conditions. Results: A total of 99 patient caregivers were surveyed. Patient demographics are listed below: 46% of respondents did not know their child would be cared for by a large team of doctors, and 43% of respondents did not know learners would be involved in their child’s care. Graphs below indicate who caregivers selected as their main doctor, and in charge of their child’s care team. Discussion: In this study, caregivers varied in who they thought was their child’s main doctor and the leader of their child’s care team. Most were unaware that large medical teams with learners at different levels of their training would care for their child. Work can be done to better orient families and caregivers to teaching teams. This could include a standardized introduction process on admission within each hospital system.
-

A Metabolic, Mechanical, Multi-Organ Masterpiece: Dural Device Support Bridge to En-Bloc Heart-Liver Transplantation in Propionic Acidemia
Rebecca Juhl, Brian Birnbaum, Aliessa P. Barnes, William Gibson, Bhargava Mullapudi, Beth Lang, Megan Faseler, Daniel E. Heble, Victoria Urban, Ryan T. Fischer, Jennifer L. Gannon, and David Sutcliffe
Introduction: Propionic Acidemia (PA) is a disorder related to abnormal protein and lipid metabolism resulting in progressive neurological injury and dilated cardiomyopathy (DCM). Interventions for PA and secondary disease manifestations can require multi-organ transplantation. Herein we report the case of a child with PA and end-stage DCM requiring left ventricular assist device (LVAD) support with eventual heart-liver transplant. Case Report: A 17 year old male diagnosed in childhood with PA developed chronically progressive DCM culminating in end stage heart failure with acute decompensations. In a recurrent admission, he progressed to require dual inotropic support and systemic anticoagulation for new LV thrombus. Heart-liver transplant eligibility was confirmed, and with further clinical deterioration requiring invasive mechanical ventilation and chemical paralysis he underwent durable, intrapericardial LVAD implant as bridge to candidacy. After accomplishing discharge, he achieved intense physical and metabolic-specific nutritional rehabilitation over the span of 3 months, and he was listed for combined heart-liver transplant. In preparation for the complexities related to dual organ transplant from LVAD support, collaborative operative simulations were completed as were adaptations of post operative immunosuppressive and medical management between transplant teams. After a 3 week waitlist duration, he underwent en-bloc heart-liver transplant with successful post operative recovery to discharge within 2 weeks. Summary: Even with effective and specialized nutritional management, DCM secondary to PA can progress to end stage heart failure requiring mechanical support and organ transplantation. Successful rehabilitation via VAD and bridge to multiorgan transplantation requires diligent collaboration across transplant teams. Despite both technical and clinical challenges, successful completion of en-bloc heart-liver transplant from VAD support can be accomplished.
-

Innovative Management of Posterior Upper Thigh Pain In Two Adolescent Athletes
Thomas Munro and Brian Harvey
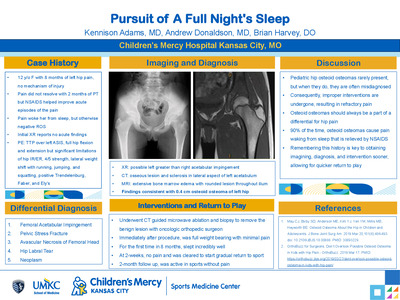
Case history: Two 16-year-old males with posterior upper leg pain. Athlete A reports he had been exploding up to dunk a basketball when he felt a pop with immediate pain in his posterior LLE. He was treated conservatively with activity modification and PT resulting in improvement of symptoms and return to full activity. He returned 15-months after the initial injury due to recurrence of pain. Athlete B stated he had tweaked his hamstring multiple times over the summer and had been working with a physical therapist for rehabilitation. He had attempted full rest for a couple weeks with graded return to activity. He had return to full activity before experiencing a repeat event of severe pain in his posterior upper leg while running at full speed in football. Athlete B stated that if felt like his leg suddenly gave out on him and lost strength. He denies hearing a specific pop. Physical Exam: Athlete A and Athlete B both have normal appearing skin and musculature of the posterior thigh. Both athletes have limited passive extension of the LLE and decreased LLE strength, most significant with resisted knee flexion. Athlete A and B both have focal pain over the left ischial tuberosity with athlete B reporting tenderness extending slightly into the proximal hamstring. No pain is reported when palpating over the ASIS, AIIS, pelvic crest, or greater trochanter. Both athletes have a negative FABER, FABER, and Log Roll. Athlete A has been using crutches to assist with ambulation. Athlete B has a slightly antalgic walking pattern with reported discomfort/pain in left upper extremity. Differential diagnosis: 1) Proximal hamstring strain 2) Ischial tuberosity avulsion fracture/apophysitis 3) Piriformis syndrome 4) Stress fracture (Ischial or femoral) 5) Ischial femoral impingement syndrome Tests and results: - Athlete A: Xray: Left ischial apophysis avulsion fracture. CT: redemonstration of an apophyseal avulsion fracture (1.5cm displaced) with interval development of calcified callus/heterotopic ossification. CT guided fenestration. - Athlete B: Xray: asymmetric appearance the ischial apophyses, with widening/irregularity on the left. MRI Pelvis: Inflammatory marrow signal of the left ischial apophysis. Mild edema around the proximal hamstring tendons. CT guided fenestration. Final/Working Diagnosis: Athlete A: Chronic avulsion fracture of the ischial tuberosity with subsequent nonunion. Athlete B: Acute on chronic ischial tuberosity avulsion fracture. Discussion: There is controversary over the best treatment strategies for pelvic avulsion fractures. In general, non-operative treatment of fractures with < 2cm displacement ( < 1.5 cm for ischial fractures) have a high success rate resulting in healing about 97% of the time. Non-unions are rare, but if they are to occur the ischial tuberosity is a likely location. The use of fenestration as a therapeutic treatment for non-union ischial tuberosity avulsion fractures has been exhibited in a 3 patient case series and 1 case report. We present two athletes with a chronic/acute on chronic ischial tuberosity avulsion fractures who underwent fenestration of the enthesis of the proximal hamstring. Outcomes: Athlete A had initial successful management with pain improvement, healing changes on imaging, and return to sport. Over a 15-month period he exhibited intermittent pain with worsening acute pain. He subsequently underwent an IR guided fenestration. His pain improved and he demonstrated osseous bridging on imaging. Athlete B also underwent fenestration with concerns of acute on chronic injury.
-

Insidious Ankle Swelling
Catharine Kral and Brian Harvey
10-year-old female presented to clinic for left heel pain and swelling. She participates in dance for an estimated 8-9 hours a week. Symptoms started four weeks prior to presentation. She does not remember any inciting event, fall, trauma, or other mechanism of injury prior to onset. She says the pain is localized to the lateral aspect of her calcaneus and extending up to her Achilles. She has never seen any bruising, erythema, or skin changes overlaying the swollen region. Family reports she intermittently has a limp. It is most tender to touch or when she bumps her foot on something. She continued to dance for the first two weeks, as she says her pain has not worsened with dancing. However, she has tried resting the last two weeks with no improvement in symptoms. She has no pain that wakes her up at night. She denies any numbness or tingling in her foot or toes. The case was discussed with Rheumatology who agreed with CRMO and recommended lab work and additional whole-body MRI. ESR was 15 and platelet count 65,000 while additional MRI showed multiple lesions throughout, including bilateral acetabula, superior/inferior pubic symphysis, right femoral neck, right tibia metaphysis, bilateral tibia epiphysis, right great toe, second and third metatarsals. With the lab work, MRI findings and absence of other type b symptoms, CRMO was the leading diagnosis. NSAIDs were started as the common first line treatment for pain control and disease modification.
-

Phlebotomy-Free Days in Common Conditions Among Hospitalized Children and the Association with Clinical Outcomes
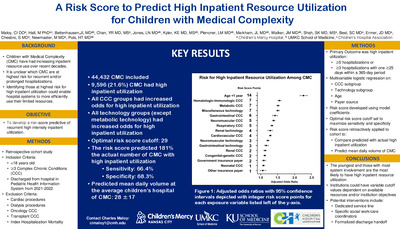
Megan Collins, M Hall, SS Shah, MJ Molloy, PL Aronson, JM Cotter, MJ Steiner, MJ Tchou, JR Stephens, and Jessica L. Markham
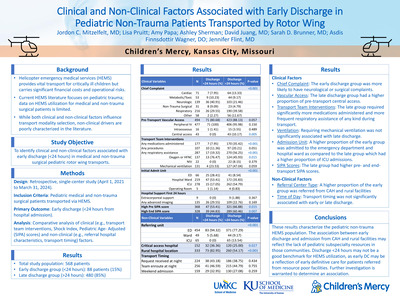
Background: Phlebotomy is an invasive procedure associated with pain and iatrogenic anemia. Minimizing phlebotomy for hospitalized children could improve their experience and avoid unnecessary tests. Objective: To describe: 1) the prevalence of phlebotomy-free days among children hospitalized with common conditions and 2) the association of phlebotomy-free days with clinical outcomes. Design/Methods: We performed a multicenter, cross-sectional study of children hospitalized 1/1/2018 to 12/31/2019 with an All Patient Refined Diagnosis Related Group (APR-DRG) for common infections across 38 hospitals in the Pediatric Health Information System (PHIS) database. We excluded patients with length of stay (LOS) < 2 days, medical complexity, interhospital transfers, and those receiving intensive care. We defined phlebotomy-free days (PFDs) as hospital days with no laboratory blood testing and measured the proportion of PFDs per hospital day (PFD ratio) for each condition and hospital. Hospitals were grouped into low, moderate and high average PFD ratios. Adjusted outcomes were compared across groups and included LOS, costs, and all-cause 14- and 30-day readmission rates. Results: We identified 126,135 patient encounters (Table 1). Bronchiolitis (N=31,302), non-bacterial gastroenteritis (N=20,430), and pneumonia (N=16,031) accounted for the greatest number of hospital days. Bronchiolitis (0.78) and pneumonia (0.54) had the highest overall PFD ratios, while bone and joint infections (0.28) and non-bacterial gastroenteritis (0.30) had the lowest overall PFD ratios. There was wide variation across hospitals and conditions in PFD ratios (Figure 1). We identified 8 hospitals with low, 21 with moderate, and 9 with high PFD ratios (Figure 1 and Table 1). There were statistically significant but small differences in the distributions of age, payer, and H-RISK among patients in the low, moderate, and high PFD hospital groups (Table 1). There were no differences in adjusted outcomes across low, moderate, and high PFD hospital groups (Table 2). Conclusion(s): Among children hospitalized with common infectious conditions, there was variation across conditions and hospitals in the proportion of PFDs per hospital day. Hospitals with low, moderate and high ratios of PFDs had no differences in outcomes. Our data suggest at least some laboratory overuse and opportunities to improve the experience and care of children hospitalized with infections.
-

Sepsis-induced Acute Lung Injury and the Development of Bronchopulmonary Dysplasia in Premature Infants
Jacob S. Ward, Hung-Wen Yeh, Megan Tucker, and Venkatesh Sampath
Background: Bronchopulmonary dysplasia (BPD) is a significant cause of morbidity and mortality in premature infants with several known risk factors. Recent literature described the harmful effect of inflammation on the developing lung. Recently, we showed that late-onset sepsis (LOS) and necrotizing enterocolitis (NEC) causes acute lung injury (ALI) in preterm infants as measured by increases in pulmonary severity scores (PSS). The aim of this study was to investigate the association between LOS-induced ALI and BPD outcomes. We hypothesized that LOS would increase the likelihood of developing BPD, and the associated LOS-induced ALI will add to the ability to predict development of BPD. Objectives: 1) Determine if LOS and number of LOS events increase risk of developing BPD. 2) Determine if LOS-induced ALI is more likely to result in BPD. Methods: A retrospective single-center study of 523 infants < 31 weeks gestation and < 1500 grams admitted prior to day of life 7 from 2010-2020 who survived to at least 36 weeks gestation (Fig. 1). Culture positive and rule-out sepsis events were identified, and PSS scores were calculated starting from -72hr from event up to 1 week after the initiation of antibiotics. BPD was defined as per the NICHD (year 2000) consensus definition. Bivariate associations with BPD were assessed by Wilcoxon rank-sum test and Chi-squared test. BPD was predicted by conditional inference forest using demographic plus (1) LOS and (2) plus ALI summary statistics. Results: Among the 523 eligible infants, 198 had at least 1 sepsis event and 325 had no sepsis event. In the sepsis group, 69% developed BPD compared to only 49% of those without sepsis (Fig. 1). Development of BPD showed bivariate associations with sepsis and number of sepsis events (both p < 0.001, standardized mean difference or SMD 0.21 and 0.41, Table 1), the median area under the PSS curves (SMD 0.19, p-value < 0.008), as well as time points +48hr (SMD 0.2, p-value < 0.006), +72hr (SMD 0.2, p-value 0.007), and +168hr (SMD 0.32, p-value < 0.001). Adding sepsis, number of sepsis events, or PSS measures to demographic variables did not increase area under ROC curve in predicting BPD. Conclusions: Our preterm cohort revealed significant bivariate associations of sepsis, number of sepsis episodes, and PSS for BPD. However, they did not improve prediction accuracy of BPD to the demographic variables. Future work will examine the effect of sepsis-induced ALI on severe BPD and use additional parameters such as CRP to enrich our prediction models.
-

A Case of Hexasomy 15q due to a Tricentric Supernumerary Chromosome 15
Emily Farrow, Laura A. Cross, Bonnie Sullivan, Keely M. Fitzgerald, Joseph Alaimo, Elena Repnikova, John Herriges, and Lei Zhang
Background: A 7-month-old male with a history of developmental delay, plagiocephaly, hypotonia, chronic cough/congestion was admitted for abnormal movements. Prolonged EEG revealed focal epilepsy and epileptic spasms. Genetic testing revealed a complex structurally rearranged chromosome 15 which contains two inverted duplicated chromosome 15s joined together at one end, resulting in partial hexasomy for 15q. Case presentation: The proband was born to a G2P2 33-year-old mother following an uncomplicated pregnancy at 40 weeks 2 days gestation. At birth he was 6lbs 8oz, 20in long, and APGARs were 3/5/9 at 1/5/10 minutes. At delivery he was limp, pale and had poor tone with minimal crying and respiratory depression. He was admitted due to persistent seizure-like activity. Aa prolonged EEG was abnormal, but movements were not seizures, and he was discharged without medication. A newborn hearing screen was failed, and follow-up confirmatory testing showed mixed hearing loss with right greater than left. At 7-months-of age he was readmitted for seizure. Repeat EEG was indicative of clinical and subclinical focal seizures and epileptic spasms. At his last evaluation at, 11 months of age, he has global developmental delay, hypotonia, and wears bilateral hearing aids. He is unable to sit unsupported but does have head control, is able to roll over and grabs objects with both hands. Imaging studies to date have been negative, including MRI, echocardiogram, and renal ultrasound. Epilepsy is currently well controlled with medication. Microarray testing was ordered at 7 months and showed six copies of an ~7.6 Mb segment between the common breakpoints BP1 and BP4, followed by four copies of an ~1.5 Mb segment between BP4 and BP5 in proximal 15q from 15q11.2 to 15q13.3. Methylation and copy number analysis of 15q11.2q13.1 for Prader-Willi (PWS) suggested maternal inheritance. Chromosome analysis demonstrated a male karyotype with 47 chromosomes including an extra tricentric chromosome. Interphase FISH analysis shows six copies of SNRPN (15q11.2) in 92% of nuclei and two copies of SNRPN in 8% of nuclei. Metaphase FISH analysis found two enhanced SNRPN (15q11.2) signals consistent with a total of four copies of SNRPN in this additional derivative chromosome, indicating the chromosome 15 is composed of two inverted duplicated 15s linked each other at the ends as a way of mirror image. Parental chromosomes were normal, confirming de novo inheritance. Conclusions: Although supernumerary marker chromosome (SMC) 15 itself is common, occurring in ~1/30,000 births, individuals with a tricentric der(15), resulting in partial hexasomy 15q are rarely reported. Complimentary techniques including microarray, MLPA, FISH, and G-banding were used to resolve the structure of the SMC 15. In the future, novel technologies, such as optical mapping, may also be beneficial in the resolution of complex structural variants.
-

Evaluating the Impact of Long Read Genomes in Rare Disease: A systematic analysis of 1000 HiFi Genomes
Emily Farrow, Isabelle Thiffault, Ana S A Cohen, Tricia N. Zion, Adam Walter, Margaret Gibson, Chengpeng Bi, Warren A. Cheung, Jeffrey J. Johnston, and T Pastinen
Introduction: Genomic technologies continue to advance at a rapid rate, leading to continued novel gene-disease discoveries. However, despite the exponential increase in new gene discoveries, diagnostic rates in rare disease continue to range from 30-50%. To evaluate the impact of long read genome sequencing (lrGS) in a rare disease cohort, lrGS was implemented systematically in an institution-wide research program, Genomic Answers for Kids (GA4K). Methods: Individuals enrolled in GA4K, with a suspected genetic disorder, that remained undiagnosed after exome or genome sequencing, were submitted for HiFi sequencing. Probands were sequenced to a target depth of 30X coverage. Analyses included copy number, structural variation, single nucleotide variation, repeat expansion, and for a subset of genomes 5-methyl C detection. Clinical variants previously reported were used to assess lrGS variant detection algorithms. Additionally, sensitivity and specificity for lrGS were calculated by comparison to an Infinium Global Screening microarray. Results: As we have previously demonstrated, lrGS sensitivity and specificity for SNVs were slightly higher than short read genome sequencing (srGS), at 99%. Additionally, lrGS continued to identify ~150 novel rare variants impacting a coding gene (MAF <0.01%) compared to srGS. Increased coverage and phasing resulted in the detection of variants previously uncalled in sr sequencing, and phasing of variants in singletons, confirming molecular diagnoses. Given the previously demonstrated accuracy of SNV, we next focused analyses on more complex variation, not readily detectable by srGS. Approximately 39% of samples initially screened positive for a potential pathologic expansion (n=59 genes), with filtering criteria maximized for sensitivity. After interpretation, which includes examination of the repeat motif and structure, ~1.6% were considered to be pathogenic alleles, highlighting the importance of sequencing suspected expansions in large cohorts in addition to sizing. When SV/CNV are limited to variants at less than 5% frequency that impact a coding region (CCDS), there are 17.8 variants/genome, of these on average 4 overlap OMIM CCDS. Beyond characterization of coding impact, the nature of SV/CNV allows determination of orientation of duplications (on average 3 rare CCDS duplications per genome) as well as superior detection of infrequent inversions (one in six genomes has CCDS impacting inversion) as compared to other sequencing approaches. Direct 5-methyl-C detection (5mC-HiFi-GS) has been completed in 380 genomes and focusing on rare (< 0.5% population frequency) gene proximal (5’) hypermethylation suggestive of “promoter silencing”, we observed on average 51 such alleles per patient (13 in OMIM genes). To date, two of the OMIM promoter hypermethylation events from 5mC-HiFi-GS are linked to previously undetected pathogenic repeat expansions, but many others are proximal to novel unstable repeats and other non-coding rare variants with potential function. In parallel, the rare methylation signatures faithfully recapitulate previously known disease variant linked epigenetic pertubations (e.g. DM1). Conclusions: The implementation of lrGS in an ES/GS negative cohort resulted in an approximate 10% increase in diagnostic yield. Importantly, previously reported variants were recapitulated, indicating that lrGS could be utilized as a first-tier genome test, simplifying genetic testing algorithms and increasing efficiency. Our developing catalog of rare SVs and methylation variants are now giving new handles for unsolved disease in known and novel disease genes. Anticipated improvements in throughput and cost will enable the widespread integration of long read sequencing into clinical care.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}