
These posters have been presented at meetings in Children's Mercy and around the world. They represent research that was done at the time they were created, and may not represent medical knowledge or practice as it exists at the time viewers access these posters.
-

Implementing the Summer Food Service Program within the Healthcare Setting
Laura M. Plencner, Margo Quiriconi, Sarah Sentmore, and Molly Krager
The Summer Food Service Program was established to ensure that children continue to receive adequate nutrition while school is out. This poster describes how the program was implemented in the Children's Mercy Kansas City healthcare system from 2016-2018.
-

Panama: Exploration of Multiple Health Care Settings and Spanish Immersion
Danielle Gonzales
Details how the urban and rural settings of Panama offer an unique opportunity for Spanish immersion and disease pathology learning experiences.
-

Pediatria en Panama: A Spanish International Health Experience
Vickie Blanco
Reports learning experiences while working with several pediatric care facilities in Panama.
-

Philippine Children's Medical Center and Dr. Jose Fabella Memorial Hospital
Adam Grumke
Describes medical learning experiences of pediatric resident while working in two Philippine medical facilities.
-

Sawubona from Swaziland! A Global Health View of the HIV/AIDS Epidemic in Swaziland
Abby Hardin
Describes a global health learning experience with Baylor International Pediatric AIDS Initiative in Swaziland.
-

"Sterile Cockpit": How Utilizing Aviation Regulations Can Reduce Errors in ECMO Procedures
Sarah P. Jimenez, Johanna I. Orrick, Kari L. Davidson, and Debra E. Newton
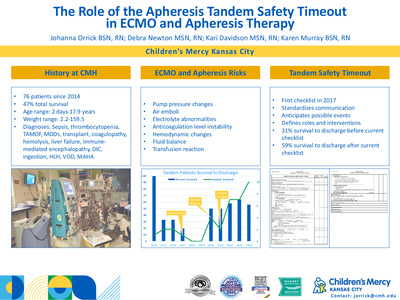
The "Sterile Cockpit Rule," developed in 1981 as an aviation regulation, was adapted by the ECMO core team to promote a distraction-free environment during critical ECMO procedures. Upon review of the data including tracking of interruptions, errors, and staff experience, it is evident that the concept of Sterile Cockpit has streamlined procedure efficiency, as well as safety.
-

The Lake Clinic Cambodia, A MedPeds Experience . . .
Jeremy Jennings and Jennifer Watts
Describes global health learning experience providing ambulatory care in Cambodia.
-

Utility of Point-of-Care Beta-hydroxybutyrate Testing for Predicting Diabetic Ketoacidosis in the Pediatric Emergency Department
Michelle Knoll, Kelsee Halpin, and Ryan McDonough
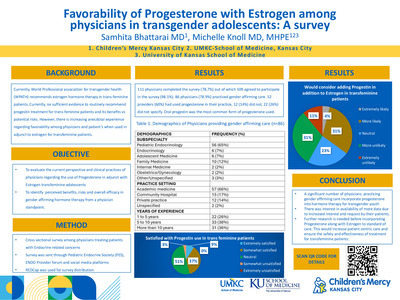
The objective of our investigation was to describe the diagnostic characteristics of point-of-care capillary beta-hydroxybutyrate (BOHB) testing to predict diabetic ketoacidosis among pediatric patients presenting with hyperglycemia in the pediatric emergency department.
-

Save the Pharmacy Piggy Bank: Managing Mega High-Cost Drugs
Richard K. Ogden Jr., Jerame Hill, and Sam Abdelghany
-

Early Identification of Depression in Patients with Pediatric Epilepsy
Erin Fecske, Paul Glasier, Lines Vargas Collado, and Elizabeth Rende
Describes the use of the Neurological Disorders Depression Inventory-Epilepsy-Youth (NDDI-E-Y) in adolescent patients in a comprehensive epilepsy center to identify patients who need referral for mental health care.
-
 by Grace Winningham, Cy Nadler, Sarah Nyp, Eugenia K. Pallotto, and Ashley Sherman")
Developmental Intervention Patters in a Level IV Neonatal Intensive Care Unit (NICU)
Grace Winningham, Cy Nadler, Sarah Nyp, Eugenia K. Pallotto, and Ashley Sherman
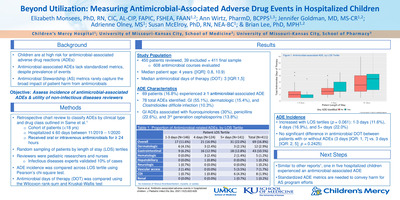
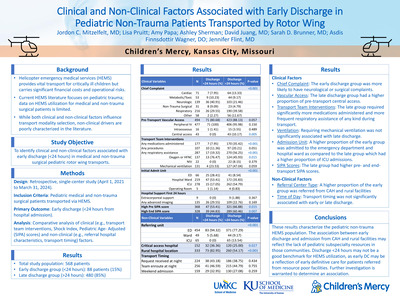
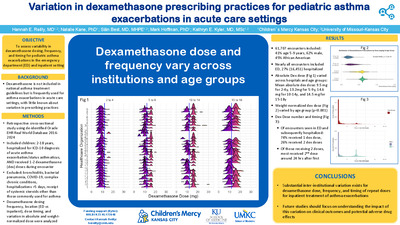
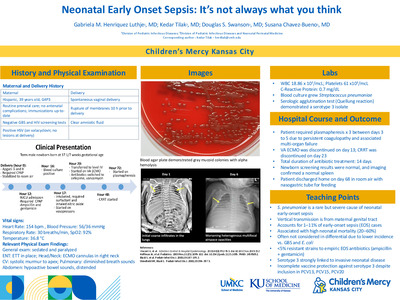
Background: There are no evidence-based standards for if/when developmental interventions should be initiated while an infant is in the neonatal intensive care unit (NICU), or these services yield incremental benefit. To support future prospective studies evaluating the neurodevelopmental benefits of NICU-based services as well as standardizing protocols for developmental interventions in the NICU, a thorough descriptive investigation of current developmental intervention practices is necessary. Objective: To describe trends in the delivery of developmental interventions [physical therapy (PT), occupational therapy (OT), speech-language therapy (ST), child life (CL), and music therapy (MT)] in high-risk infants in a large level-IV NICU. Methods: Electronic records of infants discharged over a 30 month period were manually reviewed to extract demographic variables and therapy patterns. Results: Records for 449 extreme and very preterm infants (23 0/7 to 31 6/7 weeks gestation) were reviewed. Birth weights ranged from 0.340 kg to 2.570 kg. Overall, ST had the lowest rate (6.7%) and child life had the highest rate (73.3%); ST was started at the oldest postmenstrual age at 53 0/7 ± 8.4 weeks. Eight percent of the infants had a tracheostomy, 18.0% had a gastrostomy-tube. Infants with a tracheostomy or gastrostomy-tube were more likely to receive all of the interventions (p < 0.05). The tracheostomy infants receiving ST had a higher birth weight and a longer hospital stay (p’s < 0.05), irrespective of gestational age. For each developmental intervention, infants receiving the therapy had a longer hospital stay (p < 0.0001). There were no significant differences in use of any of the therapy types related to gender, race, or language. Conclusions: This study reveals varying rates of developmental interventions in < 32 week gestation infants, with longer hospital stays associated with higher rates of interventions. ST was the least utilized modality and initiated on average at the oldest postmenstrual age, possibly reflecting low provider familiarity with potential ST benefits. More trends on NICU-based services is needed to support prospective studies investigating the benefits.
-

Integration of a Pharmacist in a Pediatric Medical Home for Children with Medical Complexity
Alannah K. Yoder, Richard K. Ogden Jr., Ingrid A. Larson, and Emily J. Goodwin
Background/Objectives
Children with medical complexity require unique care, specialized attention, and a dedicated team to meet the needs of the patient & caregivers. Drug-therapy related problems in complex, chronic conditions influence financial, institutional, and patient outcomes. The addition of a pharmacist allows for collaboration and delivery of comprehensive medication management in order to provide value-added medication services to optimize complex therapeutic regimens and patient outcomes through evidence-based practice, medication adherence, medication use coordination, and medication safety processes.
Description
Our program provides a pediatric medical home for hundreds of children with medical complexity. Families are cared for by a comprehensive medical team, including a clinical pharmacist. The pharmacist is available for all appointments and meets with patients and caregivers at the beginning of clinic visits. The pharmacist’s initiative to improve patient care is provided through multiple services which include: (1) comprehensive medication reconciliation through history provided by caregiver, outpatient pharmacy review, and chart review of specialty teams; (2) adverse drug assessment; (3) systemic drug-utilization review of each medication (drug-disease contraindication, drug-drug interaction, drug-patient precaution, dosing, duration of drug treatment, over and/or underutilization, drug dosage for modification, adherence concerns, and determination if additional monitoring is warranted); (4) patient education and development of personal, family-friendly medication lists; and (5) coordination of care between inpatient admissions, specialty/consulting services, home healthcare, and prior authorization needs.
Significance
The integration of a pharmacist in a pediatric medical home for children with medical complexity and childhood-onset disabilities allows for innovation and interdisciplinary collaboration to provide comprehensive medication management. Incorporation of family education and tangible medication plans promotes safe and consistent medication practices. Further studies describing the qualitative and quantitative impact on patient outcomes will be conducted at our institution.
-

Oxcarbazepine Overdose in a Polysubstance Related Suicide
Melissa Beals, Robert J. Krumsick, C. Clinton Frazee III, Lindsey J. Haldiman, and Uttam Garg
Introduction
Oxcarbazepine is a derivative of carbamazepine that is used primarily in the treatment of epilepsy, and experimentally as a mood-stabilizer in adjunctive therapy for the treatment of bipolar disorder. Oxcarbazepine is converted through oxidation to its pharmacologically active metabolite 10-OH-Carbazepine, which is thought to be responsible for most of the anticonvulsant action of the drug. Adverse effects of oxcarbazepine are generally dose-dependent and may include fatigue, somnolence, dizziness, diplopia, nystagmus, and ataxia. Additive sedative effects have been noted when oxcarbazepine is used in combination with other CNS depressionproducing medications. Furthermore, oxcarbazepine and 10-OH-Carbazepine are powerful CYP2C19 inhibitors, potentially increasing the plasma concentration and pharmacological response of CYP2C19 substrates such as diazepam. The therapeutic range for oxcarbazepine is based on the metabolite and extends from 6-35 μg/mL. Toxicity has been reported with 10-OH-Carbazepine levels as low as 65 μg/mL, and one fatality has been documented with a 10-OH-Carbazepine concentration of 92 μg/mL. Hydrocodone is a narcotic analgesic that undergoes demethylation and reduction to produce several pharmacologically active metabolites, including hydromorphone, norhydrocodone, and dihydrocodeine (6-α-hydrocodol), which contribute to its efficacy. Hydrocodone toxicity may be characterized by respiratory depression, drowsiness, and coma. Therapeutic blood and plasma concentrations of hydrocodone typically range from 10-50 ng/mL, while levels greater than 100 ng/mL are considered toxic, and concentrations exceeding 200 ng/mL can be potentially fatal. Diazepam is a benzodiazepine known for its efficacy and rapid onset. Therapeutic ranges of diazepam and its metabolite nordiazepam in blood and plasma measure between 200-2500 ng/mL. Diazepam toxicity may result in drowsiness, weakness, ataxia, and coma; however, serious and fatal effects are uncommon with diazepam if used singularly. Most terminal adverse events associated with diazepam are the result of interaction or combination with other drugs, especially CNS depressants.Objective
To present a case of a polysubstance related suicide involving the synergistic effect of toxic concentrations of oxcarbazepine and hydrocodone in combination with the presence of diazepam. To report the highest blood concentration of 10-OH-Carbazepine found in literature for a drug-related death investigation.Case History
Presented in this case is a 67-year-old female with a history of depression, psychiatric hospitalization, and previous suicide attempts. The decedent was found lying supine in bed with a bottle of hydrocodone in one hand and a can of soda in the other, next to a suicide note. Several other prescription medications, including oxcarbazepine, gabapentin, diazepam, quetiapine, tizanidine, and lorazepam were found at the scene.Methods
Postmortem heart blood, femoral blood, urine, vitreous fluid, gastric contents, and liver and brain tissue were submitted for toxicological analysis. Routine screening of heart blood was performed using Enzyme Multiplied Immunoassay Technique (EMIT) and liquid-liquid alkaline extraction followed by gas chromatography/mass spectrometry (GC/MS) analysis. 10-OH-Carbazepine as well as hydrocodone and its metabolites were quantified in femoral blood by an external laboratory using liquid chromatography/tandem mass spectrometry (LC-MS/MS). Diazepam and nordiazepam quantitation was performed on heart blood using high performance liquid chromatography (HPLC).Conclusion
The most significant finding in this case is the 10-OH-Carbazepine concentration of 180 μg/mL, which is greater than the highest known fatal level of 92 μg/mL. The cause of death in this case was ruled oxcarbazepine and hydrocodone intoxication with diazepam use, -
 by Grace Winningham, Cy Nadler, Sarah Nyp, Eugenia K. Pallotto, and Ashley Sherman")
Developmental intervention patterns in a level IV neonatal intensive care unit (NICU)
Grace Winningham, Cy Nadler, Sarah Nyp, Eugenia K. Pallotto, and Ashley Sherman
Background: There are no evidence-based standards for if/when developmental interventions should be initiated while an infant is in the neonatal intensive care unit (NICU), or these services yield incremental benefit. To support future prospective studies evaluating the neurodevelopmental benefits of NICU-based services as well as standardizing protocols for developmental interventions in the NICU, a thorough descriptive investigation of current developmental intervention practices is necessary. Objective: To describe trends in the delivery of developmental interventions [physical therapy (PT), occupational therapy (OT), speech-language therapy (ST), child life (CL), and music therapy (MT)] in high-risk infants in a large level-IV NICU. Methods: Electronic records of infants discharged over a 30 month period were manually reviewed to extract demographic variables and therapy patterns. Results: Records for 449 extreme and very preterm infants (23 0/7 to 31 6/7 weeks gestation) were reviewed. Birth weights ranged from 0.340 kg to 2.570 kg. Overall, ST had the lowest rate (6.7%) and child life had the highest rate (73.3%); ST was started at the oldest postmenstrual age at 53 0/7 ± 8.4 weeks. Eight percent of the infants had a tracheostomy, 18.0% had a gastrostomy-tube. Infants with a tracheostomy or gastrostomy-tube were more likely to receive all of the interventions (p < 0.05). The tracheostomy infants receiving ST had a higher birth weight and a longer hospital stay (p’s < 0.05), irrespective of gestational age. For each developmental intervention, infants receiving the therapy had a longer hospital stay (p < 0.0001). There were no significant differences in use of any of the therapy types related to gender, race, or language. Conclusions: This study reveals varying rates of developmental interventions in < 32 week gestation infants, with longer hospital stays associated with higher rates of interventions. ST was the least utilized modality and initiated on average at the oldest postmenstrual age, possibly reflecting low provider familiarity with potential ST benefits. More trends on NICU-based services is needed to support prospective studies investigating the benefits.
-

Social Work Triage in a School District for the School Year 2017-2018
Libby Milkovich, Briana A. Woods-Jaeger, and Allison Zoromski PhD
Purpose: One in 7 children ages 2-8 have a behavioral, mental or developmental diagnosis. The prevalence of mental health disorders increases in adolescence to over 20%. Only 36% of youth who have a mental health disorder in their lifetime receive treatment. School-based services can address barriers to care. The purpose of this study was to determine the frequency and indication of referrals for students to 19 hospital-employed clinical social workers placed within a school district during one academic year (2017- 2018) and how the indication varies with level of schooling.
Methods: Students were referred to social workers by self, classmates or school personnel. The student’s school name, age, indication for assessment and place of referral were collected. The entries were analyzed if a school was listed with the entry. District demographics were collected from publicly accessible sources. Descriptive analysis was performed.
Results: For the 2017-2018 school year, enrollment for K-12 students was over 20,000. Race of the students were primarily Caucasian (74%). All schools had less than 10% receiving free/reduced lunches. Indications for triage totaled 1643, 43% from high school (HS), 26% from middle school (MS), 30% from elementary school (ES). Behavioral problems were most frequent (23%), followed by anxiety (22%). Average age for behavioral problems was 10.6(SD 3.5); with 16% HS, 27% MS, and 69% ES. Average age for anxiety was 13.3(SD 3.3); with 41% HS, 27% MS, and 32% ES. Suicide ideation/attempt had a frequency of 10% with an average age of 14.5(SD 3.0); with 62% HS, 13% MS, and 26% ES. Depression had a frequency of 5% with an average age of 14.0(SD 2.656) and 46% HS, 33% MS, and 21% ES. ADHD had a frequency of 3% with 28% HS, 17% MS, and 55% ES.
Conclusions: Internalizing disorders were the most frequent indications. The indications varied by level of schooling. School mental health professionals like social workers are able to provide triage and community mental health referrals to some. An innovative approach is needed within the schools. Currently, we are conducting a multimodal (survey, focus group, interviews) needs assessment within the school district to inform an innovative approach.
-

Review of Karyotypic Data from Low Grade Glial Brain Tumors, Specifically Pilocytic Astrocytomas, and Correlation of Genetic Aberrations with Tumor Recurrence.
Linda D. Cooley, Scott C. Smith, Lisa Warren, Melissa Gener, Kevin Ginn, and John Herriges
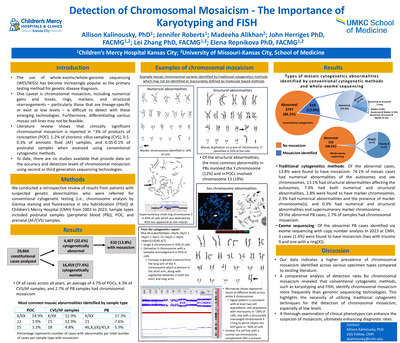
Abstract: Brain tumors are the most common solid tumor of childhood. Approximately 50% of pediatric CNS tumors are low grade gliomas (WHO grade I or II) and Pilocytic astrocytoma (PA) is the most common accounting for 33% of all gliomas in children 0-14 years and ~18% of all childhood brain tumors. Prognosis with this slow-growing tumor is excellent; 10 year overall survival of ~95%. However, event free survival averages ~50%. Patient age and extent of tumor resection are key prognostic factors; tumor location and size impact resection and outcome. Histopathological features indicate PA is a benign tumor and rarely are anaplastic features of malignancy present. This study sought to determine if chromosomal aberrations correlate with increased risk of tumor recurrence. Observation shows that while the majority of PA have a normal karyotype, a portion have highly abnormal karyotypes; the clinical significance of which is unclear. Methods: Pathology archives were queried for PA between mid-2008 and mid- 2017. Review included chromosome, FISH, microarray, molecular results, cytogenetic methods, histopathology, tumor location, patient age, extent of surgical resection, chemotherapy, radiotherapy, and outcome. Karyotypes were defined as “aberrant” if there were multiple bizarre chromosome abnormalities, multiple telomeric association (tas) figures or translocations, or multiple dicentric chromosomes. Routine cell culture methods were used with mechanical +/- enzymatic disaggregation, alpha-MEM medium, and monolayer coverslip cultures with harvest as soon as feasible to capture metaphase cells. Results: Of 64 cultured PA, 4 failed to grow. Karyotypes were normal (n=32), simple (n=3), hyperdiploid (n=12), or aberrant (n=13). Four patients had a second tumor resection; 2 had aberrant and 2 had normal karyotypes on the initial and repeat studies. Of the 13 patient tumors with aberrant karyotypes, 6 tumors (CMH cases 1-5) demonstrated tas, dicentrics, subclones, etc., and two (CMH cases 6, 7) had multiple cells with an excess of aberrant chromosomes. Four tumors (CMH cases 8-13 – not shown) had a normal karyotype with one or two highly aberrant cells; of these, one patient with two resections (CMH cases 11 & 12) showed two highly aberrant cells on both the initial and second study. Discussion: Highly aberrant karyotypes are unexpected in benign tumors. PA, is a histologically benign tumor with ~95% 10 year overall survival. Repeatedly finding highly aberrant karyotypes in some of these tumors begs the question of clinical significance. How should these karyotypes be interpreted? Finding the abnormalities in tumors resected twice suggests an ongoing cellular/biologic process specific to that tumor tissue. The repeat finding of tas and dicentrics suggests a role for telomere dysfunction in these tumors. This is consistent with up-regulation of TRF1 and TRF2 (TTAGGG repeat-binding factors) occurring in the early stages of LGG carcinogenesis, which is characterized by short telomeres, genomic instability, low proliferative rate and prolonged life span (1). Limitations of the study: Data are limited – few patients, inconsistent FISH, microarray and molecular studies were done; no sequence analysis. Multiple factors play a role in patient outcome including tumor location and resectability. Conclusions: Additional cases, additional follow-up, additional genomic analyses are needed. Next step: WES of rearranged cases is planned.
-

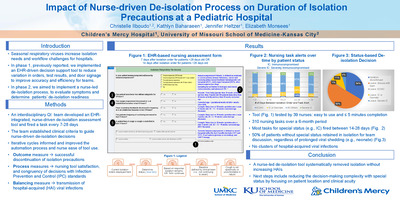
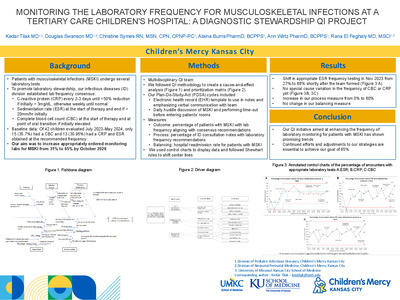
Facilitating the everyday steward: Impact of mandatory antimicrobial indication/duration and a 48 hour time out
Ann L. Wirtz, Alaina N. Burns, Brian R. Lee, Tammy Frank, Laura Fitzmaurice, Richard Ogden, Brian O'Neal, and Jennifer Goldman
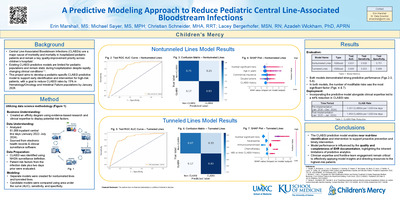
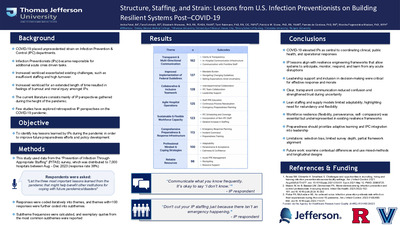
Introduction: Required indication, duration, and a 48-hour antimicrobial timeout are an integral part of antimicrobial stewardship standards; however, limited data are available to demonstrate an effect on antimicrobial utilization and antimicrobial stewardship practice. Therefore, we evaluated the impact of mandatory declared indication/duration along with a pharmacy-driven 48-hour timeout on antimicrobial utilization and antimicrobial stewardship interventions.
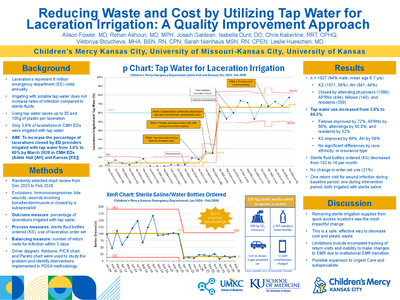
Methods: We performed a retrospective evaluation of ASP interventions and antimicrobial use following implementation of mandatory antimicrobial indication/duration at the point of computerized physician order entry (CPOE). A pharmacist-driven 48-hour antimicrobial timeout was introduced on the same date. This study was conducted at Children’s Mercy Kansas City, a 367-bed freestanding pediatric hospital servicing the Kansas City Metro Area and beyond. Data were collected from February 1, 2016 to January 31, 2018. A pre and post comparison was performed; interventions were implemented hospital-wide on February 14, 2017. ASP intervention rates were measured. Days of therapy (DOT) per 1000 patient days of antibiotics were also evaluated. Poisson models were utilized to compare DOT rates pre- and post-implementation, and seasonal decomposition analyses were performed to account for seasonal variability.
Results: A significant decrease in DOT rates was observed in non-ASP monitored antibiotics post-implementation, including cefazolin (39.7 to 36.9; p
Conclusions: Implementation of additional stewardship practices, including mandatory antimicrobial indication/ duration and a pharmacist-driven 48-hour timeout, resulted in a decrease in the use of antimicrobials, including those not monitored by our ASP. These efforts augmented, but did not replace existing stewardship efforts. These results support initiatives highlighted by national organizations to minimize unnecessary antimicrobial use through ASP.
-

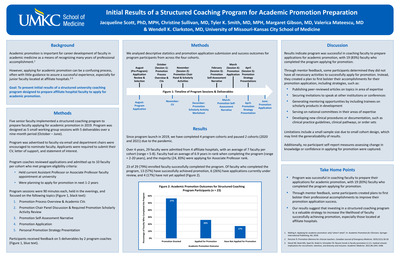
Code LITE: Developing Pediatric Residents’ Resuscitation Knowledge and Skills Using a Guided Mentoring Approach
Alyssa Stoner, Jenna Miller, Jennifer Flint, Shekinah Hensley, Brian Lee, and Kadriye O. Lewis
Background: Simulation-based learning is a popular training method in healthcare education. Literature supports multiple aspects of simulation-based training for technical skills and behavioral skills, however the effects of different pedagogies have not been investigated in this educational method.
Objective: Examine the effects of guided mentorship during simulation on pediatric residents’ learning experience.
-

Guided Mentorship: Enhancing Pediatric Resident’s Skills in Cardiopulmonary Resuscitation
Alyssa Stoner, Kadriye O. Lewis, Jennifer Flint, Shekinah Hensley, Brian Lee, and Jenna Miller
Literature supports multiple aspects ofsimulation-based training1-5to impart technical skills and behavioral skills
Effects of different pedagogies have not been investigated in simulation
Pediatric residents have minimal exposure to pediatric cardiopulmonary resuscitation (CPR) due to restrictions in work hours and increasing quality and safety initiatives6
Code LITE(Low-tech, Internal, Training Experience) is a simulation environment for our residents utilizing a guided mentorship approach, known as cognitive apprenticeship
Residents completed pre and post rotation surveys and participating residents were observed during their simulation experience Just-in-time, in-situ simulation program
10 minute specific scenario with 10 minute debriefing session
Interprofessionalteam: nurses, respiratory therapists, pharmacists, attending physicians and pediatric residents
-

Implementing Daily Management System Huddle Boards to Improve Communication Across Satellite Laboratories
Sean Tucker
Background
In a laboratory setting with fast-paced changes and heavy demands on staff, day-to-day communication across departments is challenging, yet paramount to resource sharing and real-time problem solving. Children’s Mercy Hospital Kansas City (CMH) has implemented system-wide lean practices focused on clinical and operational excellence. Our laboratory mission, or True North, is to produce clinically relevant laboratory results and information to assist in the diagnosis, treatment and prognosis of patients in a timely manner, by: �� Reducing Errors – Pre-analytical, Analytical & Post-analytical �� Making encounters with the laboratory extraordinary �� Reducing turnaround times �� Maximizing employee engagement and productivity �� Reducing waste The first phase of the CMH Daily Management System (DMS) was to implement daily huddle and metrics boards. Each individual department would align unit-level readiness and quality metrics to the institution’s True North foundational elements and report on the following daily readiness objectives: 1. MESS: Methods, Equipment, Supplies, and Staffing (displayed as green or red) 2. Situation Awareness Notifications (abnormalities that need special attention that day) 3. Recognition (employees who go above and beyond contributions from previous day) 4. Announcements (department or institutional changes taking place that day) 5. Daily Workload (reported in patient volumes and previous day test volume) 6. Quick Hits and Big Issues (problem solving: QH completed within 3 days/check-in dates for each) A multi-tiered system would include huddle boards from individual department levels (i.e. Chemistry, Microbiology, or satellite department), one overall for the lab (pictured below), and the hospital as a whole. Each tier would report up to the next tier daily at the same time. Huddles are kept to five minutes or less.
Summary
DMS allows departments to identify MESS red/green thresholds that affect patient care. All information should be displayed in a simple, clear format where any employee walking by would understand how patient care is being delivered for that day. All huddle boards are dry erase for easy documentation and use red/green magnets to identify abnormalities “at a glance.” Huddles take place at the beginning of each shift with all stakeholders present to ensure clear communication between staffing changes. Departments are required to first determine what MESS levels would be considered abnormal (red). This requires breaking down testing platforms, staffing matrices and supply and inventory par volumes to ensure continual and efficient patient care. Any downtime, critical staffing level, or backorder that can cause delays in testing should be reported red for the day. Methods are department goals that are critical for care management and can be measured as they progress. This can include mandatory education for staffing or employee vaccination compliance. Problem solving is a daily occurrence. These issues are documented as “Quick Hits” (being completed within the department in three days or less) or “Big Issues” (taking additional time, resources, and possibly external departments). Each problem is assigned to a lead and given a due date to report back. Progress is reviewed during huddles and documented using Harvey Balls showing progress. These sheets can be used to show inspectors documentation of issues resolved in the department. Every department is required to identify situations that could cause delays in patient care. This can include, but is not limited to, IT downtime, courier delays, weather concerns, construction, or surges in patient volume. This information is followed up with Announcements and Employee Recognition. Metrics provide visual content to continual improvement. Metrics are also included in daily reporting, focusing on Safety, Employees, Quality, Delivery of Services, and Stewardship or Resources. These metrics must be measurable, contribute to improved patient care, employee engagement, operational and clinical excellence. These metrics should be department specific, timely, and patient centered.
Larger health systems often have satellite facilities in different geographical locations than the main hospital. Timely communication of department readiness across a health system is vital to ensure continual patient care when distance can affect distribution of additional resources. Telecommunications allows for huddles to take place online where information can be shared in real time. This allows for administration to allocate additional resources quickly, when necessary. CMH uses Polycom RealPresence to video conference huddles at the Tier 2 Laboratory Management huddle, as well as the hospital Tier 3 level. WebEx and Skype are other options for teleconferencing.
Conclusion
The Daily Management System has allowed for improved communication between shift exchange and departments throughout the hospital. The standardized process empowers frontline employees to identify abnormalities in staffing and equipment, resolution of issues, and efficiencies in process improvement. This bottom-up approach aligns with the True North mission allowing employees to become engaged and more solution-driven. Health systems with multiple satellite locations are able to connect via telecommunication technology, allowing for real-time reporting and deployment of resources. This ensures optimal utilization of resources that can be reallocated based on volume drivers within the department. Aligning department readiness and metrics with patient outcomes daily helps build a highly reliable organization focused on continuous improvement. In this continuously changing healthcare environment, institutions must become more efficient with limited resources, focused on clinical improvement, and empowering staff to discourage burnout. DMS is an effective lean tool for organizations wanting to break down silos, improve communication between departments, and strive towards clinical and operational excellence.
-

Implementation Of A Guideline-Based Nontuberculous Mycobacteria Management Algorithm
Claire Elson, Ellen Meier, Douglas Swanson, and Christopher M. Oermann
Nontuberculous mycobacterial (NTM) disease is a challenge to manage in patients with cystic fibrosis (CF). Diagnosis of NTM pulmonary disease is complex. Effective treatment requires long term, multi-drug therapy delivered by several routes. Consensus recommendations published in 2016 were developed to guide CF providers in NTM screening, diagnosis and management. Primary Outcomes. Children’s Mercy-Kansas City (CMKC) developed an NTM working group to facilitate implementation of standardized NTM management. Methods. NTM working group: Pulmonologist (CF Center Director), Infectious Diseases specialist, nurse practitioner (CF Center Coordinator), and pharmacist. Sought expertise from the Director of Microbiology Laboratory regarding susceptibility testing. Developed NTM Management Guide from guidelines and other available literature. Diagnosis and management algorithm. Medication resource table.
-

P16-Ki67-HMB45 Immunohistochemical Profiling May Help Discriminate Between Spitzoid Melanoma and Atypical Spitz Nevi
Robert E. Garola and Vivekanand Singh
Background
When Spitz nevi have increased vertical thickness (>1.5 MM), show ulceration and deep seated mitosis, the differential diagnostic considerations of atypical Spitz nevus (ASN) or a Spitzoid melanoma (SM) enter into consideration. While expert consultation from a dermatopathologist is most often sought to resolve the differential diagnosis, it could be expensive and time consuming. Recently, the use of molecular genetic testing has also been advocated in the work group up of atypical melanocytic proliferations. On the contrary, immunohistochemistry is a more routinely used technique in most pathology centers may be more simple to apply. A single immunohistochemical marker may not be accurate enough to differentiate benign from malignant melanocytic lesions. Recently, one study (Ref. 1) employed the combination of p16, Ki-67 and HMB45 (PKH) immunohistochemistry on adult melanomas and proposed a combination of the three markers with scoring in discriminating SM and ASN in children. In this study we applied the methodology of the published study to atypical Spitzoid lesions and Spitzoid melanomas.
Methods •Institutional review board approval was obtained for this HIPAA-compliant study. •We retrospectively reviewed 10 cases (4 SM and 6 ASN) from children (age range 1.5-12 years, 6 females and 4 males). •H&E stained slides and immunohistochemical stains for PKH were independently interpreted by two pathologists. •The extent of IHC expression in the lesional cells were scored following published criteria comprised as follows:
-P16 scored as 0; >50% stained cells, 1; 11-50%, 2; 1-10%, 3; 0%
-Ki-67 scored as 0; <2%, 1; 2-5%, 2; 6-10%, 3; 11-20%, 4; >20%
-HMB45 scored as 0; gradient present, 1, doubtful/inconclusive gradient, 2; gradient absent
-The total PKH score for the combination of the 3 antibodies for any case could vary from 0 to 9.
Results • Four cases of SM had total PKH scores: 7, 6, 7 and 5. • Six cases of ASN had PKH scores of 3, 2, 3, 2, 3 and 3. •In our study all cases of SM had a total score of >4 and all ASN scored <4. • HMB45 was completely negative in one case each of SM and ASN. • Where aCGH was done, heterozygous loss of 9p correlated well with low P16 immunostain positive cell numbers in one case. Conclusions 1)Our study replicates the findings of the published study of adult melanomas and nevi that showed a total PKH score of equal/or>4 is seen in melanoma. 2) A single immunostain could be misleading as Ki-67 labeling index tended to be higher in young children (<2 years of>age) and HMB45 was occasionally negative in both ASN and SM, and P16 could be completely lost in ASN.
3) We suggest routine use of PKH immunohistochemistry in the work up of atypical Spitzoid lesions in children.
References
1) Uguen, A., et al. A p16-Ki-HMB45 immunohistochemistry scoring system as an ancillary diagnostic tool in the diagnosis of melanoma. Diag Pathol 2015; 10: 195-1005.
-

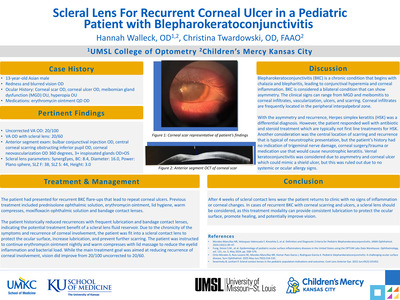
A Healthcare Improvement Initiative to Increase Multidisciplinary Pain Management Referrals of Youth with Sickle Cell Disease
Rae Ann Kingsley, Gail Robertson, Lynne Covitz, and Areli Ramphal
-

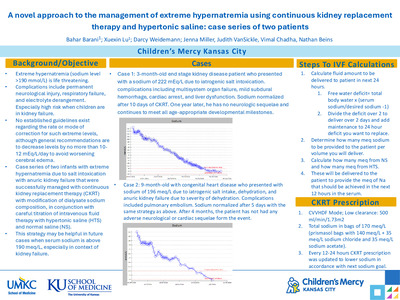
A NINJA Initiative at Children's Mercy
Richard Ogden, Bradley A. Warady, Vimal Chadha, and Wendy Hoebing




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}