
These posters have been presented at meetings in Children's Mercy and around the world. They represent research that was done at the time they were created, and may not represent medical knowledge or practice as it exists at the time viewers access these posters.
-

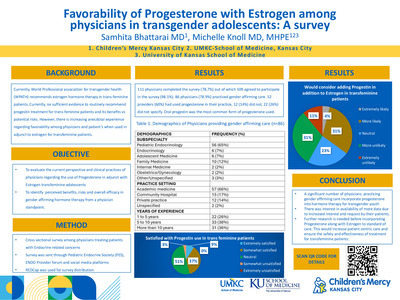
Using Standardized Scripting to Improve Antibiotic Stewardship in a National Pediatric Urgent Care Collaborative
Amanda Nedved, Melody Fung, Cindy Liu, Rana Hamdy, and Amanda Montalbano
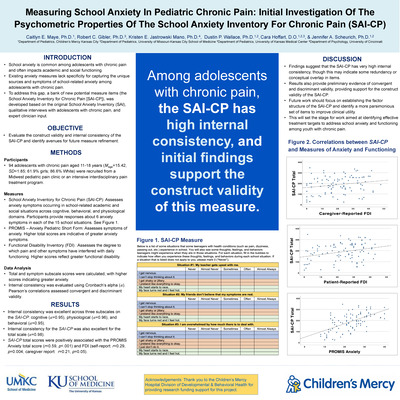
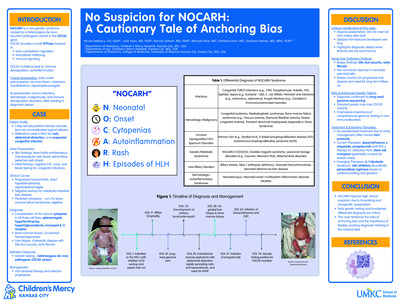
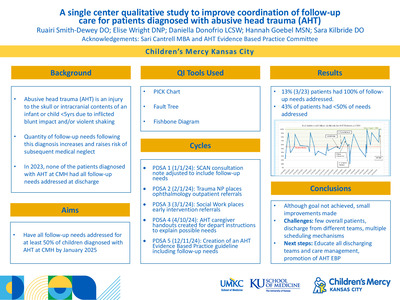
Background: A study using administrative data reported urgent care providers as having the highest rates of inappropriate antibiotic use for upper respiratory illnesses. In a national survey, pediatric urgent care providers reported family expectations as a primary driver for prescribing inappropriate antibiotics. Standardized scripting has been effective at reducing unnecessary antibiotics while increasing family satisfaction.
Objective: To reduce inappropriate prescribing for upper respiratory infections (acute otitis media (AOM), otitis media with effusion (OME), and pharyngitis) in pediatric urgent cares by 20% by December 1, 2020 through use of standardized scripting in Year 2 of a national pediatric urgent care quality improvement collaborative.
Design/Methods: Participants were recruited via email, newsletters, and webinars from pediatric urgent care national societies. Each site committed at least 3 providers who each submitted data from 10 encounters per month. Antibiotic prescribing was defined as appropriate based on consensus guidelines. Previously published antibiotic stewardship scripting for viral upper respiratory infections was adapted for use with the three target diagnoses. Patient and family advisors reviewed all scripting and their feedback was incorporated into the revised standardized scripting. Clinical examples for each diagnosis using the standardized scripting were provided to the collaborative by use of digital cartoon videos, written framework, and templated discharge instructions. Data from clinical encounters were submitted via a REDCap form, analyzed for inappropriateness, and reported back to participating sites via run charts during monthly webinars.
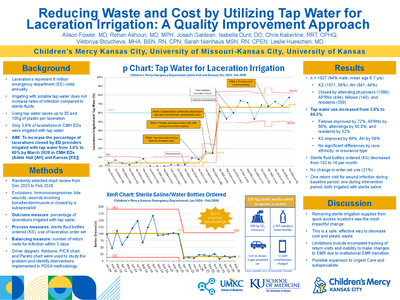
Results: The 104 participants from 10 institutions submitted 1,150 encounters for analysis in the intervention cycles (May-December 2020). Overall inappropriate antibiotics decreased from 26.4% to 16.6% (p=0.13). Inappropriate antibiotic use decreased in AOM (38.6% to 26.5%; p=0.12) and pharyngitis (14.5% to 8.8%; p=0.26). OME increased from 30.8% to 46.7% (p=0.18) (Figure 1). During the study immediate antibiotic prescriptions for OME decreased; however, delayed prescribing increased (Figure 2).
Conclusion(s): In its second year, this national collaborative developed standardized scripting to overcome the barrier of perceived family expectations to decreases inappropriate antibiotic prescriptions in pediatric urgent care for AOM and pharyngitis. Future interventions will target the inappropriate use of delayed prescribing in OME.Presented at the 2021 PAS Virtual Conference
-

Utilization of Enteral Tranexamic Acid To Stabilize Gastrointestinal Hemorrhage in Pediatric Patients on ECMO
Gina Patel, Jenna Miller, Thomas M. Attard, and Asdis Finnsdottir Wagner
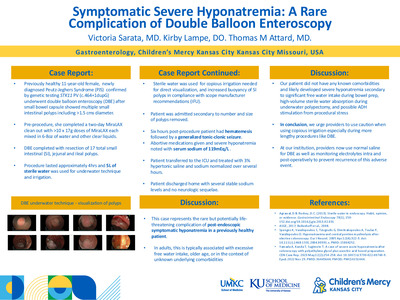
Hemorrhagic and thrombotic complications on Extracorporeal Membrane Oxygenation (ECMO) support are associated with significant morbidity and mortality. There is a paucity of literature describing the incidence and management of Gastrointestinal (GI) bleeding on ECMO. We describe the use of enteral tranexamic acid (TXA) as an alternative strategy in two pediatric patients with GI hemorrhage on ECMO. Case 1 A 5-year-old with Wilms Tumor required Veno-Venous ECMO due to respiratory failure associated with pulmonary hemorrhage and air-leak syndrome. Her course was complicated by severe GI hemorrhage refractory to IV proton pump inhibitor (PPI), IV TXA and octreotide infusions. Concomitant IV TXA and cessation of systemic anticoagulation coincided with emergent transition to Veno-Arterial (VA) ECMO after cannula thrombosis. Procedural interventions included esophagogastroduodenoscopies (EGD) revealing gastric ulcers, two endovascular embolization procedures, and a third arteriogram due to continued bleeding that did not identify a source. Enteral TXA (20 mg/kg q 8 hours) was then begun with resolution of GI bleeding, reduction in blood product transfusion and no further emergency circuit changes. She survived to hospital discharge. Case 2 A 3-year-old with a burn injury required VA ECMO due to cardiopulmonary collapse. Her course was complicated by GI hemorrhage. She received a PPI, octreotide infusion and was started on IV and enteral TXA (10 mg/kg q 8 hours). An EGD did not identify a bleeding source. There was no interruption in circuit anticoagulation or integrity. She remained on enteral TXA for 48 hours until GI bleeding resolved. She survived to ECMO decannulation. Patients supported by ECMO require systemic anticoagulation thus making GI bleeding difficult to manage. We report the use of enteral TXA to provide anti-fibrinolysis. This was associated with cessation of bleeding but not associated with further circuit thrombosis. Enteral TXA can be an additional tool used for GI bleeding on ECMO.
-

Virtual Child Neurology Education During COVID-19 and Beyond
Jennifer J. Dilts and Rose N. Gelineau-Morel
Background: Even prior to the Coronavirus Disease 2019 (COVID-19) pandemic, Children’s Mercy Kansas City’s large neurology division struggled to engage learners in educational conferences. With 113 division members across 5 locations, attending conferences was challenging. While some conferences were live-streamed, we offered no recorded lectures, and most conferences were attended solely by trainees and 3-4 select faculty. COVID-19 eliminated in-person group learning opportunities.
Objective: We aimed to rapidly develop and implement a comprehensive and inclusive virtual child neurology curriculum and assess its impact.
Design/Methods: We created a neurology education “team” using Microsoft® Teams. Within 1 week of beginning social distancing, we offered an average of 4 live virtual lectures per week, increased from 2 weekly lectures prior to COVID-19. Lectures covered diverse topics (e.g. quality improvement, empathy, leadership) in addition to clinical neurology. We recorded and stored all lectures and supplementary materials in Microsoft® Teams. We distributed a survey after the third and fourth weeks of virtual education, and again after 3 months.
Results: Survey response rate was 92% (104/113) for week 3, 84% (95/113) for week 4, and 55% (62/113) at 3 months. Percentage of learners attending at least 1 lecture per week increased from 28% (pre-COVID-19) to 74% (week 3), and this gain was sustained at 3 months (88%) (Figure 1). Attendance was well-distributed amongst all types of learners (Figure 2), averaging 22 participants per lecture (SD 9.2). Mean learner satisfaction increased from 5.7 out of 10 (pre-COVID-19, SD 2.3) to 8.5 out of 10 (3 months, SD 1.25, 2-tailed paired t-test p<0.001) (Figure 3). Learners appreciated easy access to educational materials, including viewing recorded lectures. At 3 months, 88% of respondents wished to continue virtual education, and 60% of clinical staff planned to change their work practice based on information they learned. Sixty-seven percent of trainees “agreed” or “strongly agreed” that the virtual curriculum improved how prepared they felt for upcoming examinations. Rapport across the division increased, with 85% of respondents feeling more connected to colleagues.
Conclusion(s): COVID-19 was a disruptive innovation, catalyzing the rapid formation of a virtual neurology curriculum. Our curriculum increased learner satisfaction, engagement, and rapport. Nine months into the pandemic, we continue to offer several virtual neurology lectures each week.Presented at the 2021 PAS Virtual Conference
-

Where are they now? Spanish utilization and career direction of graduates of a pediatric bilingual continuity clinic
Jodi Dickmeyer, Katie McAnany, Sarah Stone, and John Cowden
Background: The Clínica Hispana de Cuidados de Salud (CHiCoS) Program was created in 2009 to prepare bilingual (English-Spanish) pediatric residents to independently give safe, effective care to Spanish-speaking families. By providing 1:1 support from a culture and language coach over three years of residency, CHiCoS has improved residents’ cultural and linguistic skills and families' perceptions of care. The effects of such training on residents’ future careers have not been formally studied.
Objective: To describe the careers of former CHiCoS residents, the impact of culture and language training on their practice, and opportunities for post-CHiCoS cultural and language training.
Design/Methods: In this descriptive, cross-sectional study, we created and sent a digital survey (26-44 questions depending on branching logic) to former CHiCoS residents including details of their current and previous practice, Spanish utilization with patients/families, maintenance of Spanish proficiency, impact of CHiCoS on career satisfaction, and desire for ongoing culture and language training. All CHiCoS residents graduating from 2011-2019 were included, except those who did not complete the program or who were authors of this study.
Results: Twenty-four of 33 CHiCoS graduates (73%) completed the survey. A majority worked in academic (14/24) and urban (14/24) settings. Almost all who were qualified bilingual staff upon CHiCoS graduation (N=18) worked in settings with Spanish-speaking patients/families (94%) and used their Spanish skills in greater than half of their visits (89%). Among graduates seeing >20% Spanish speaking patients (N=9), all but one felt they maintained or improved their Spanish skills. Most of those with <20% Spanish-speaking patients (10/13) reported maintaining their proficiency level, while those with no Spanish-speaking patients (N=2) felt their skills had eroded. CHiCoS training had a moderate to large impact on career satisfaction for 83% of graduates (Table, Figure), and 71% reported a desire for further support in cultural and linguistic skill development, including post-CHiCoS culture and language coaching.
Conclusion(s): Culture and language coaching for bilingual residents leads to careers serving culturally and linguistically diverse patients and families. Language skills developed in residency can be maintained through ongoing use in future practice, but most graduates would like to continue formal culture and language training, even after reaching a professional level of proficiency.Presented at the 2021 PAS Virtual Conference
-

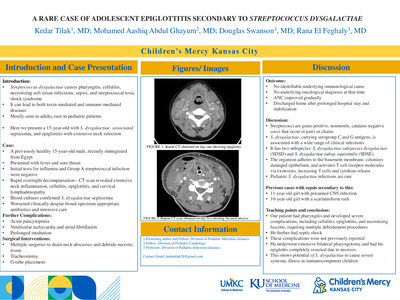
Subacute thromboembolic pulmonary hypertension with acute clinical worsening but improving CT findings - a case reporrt
Doaa Aly, Alvin Singh, Pamela Finn, Kate Carp, and Brian Birnbaum
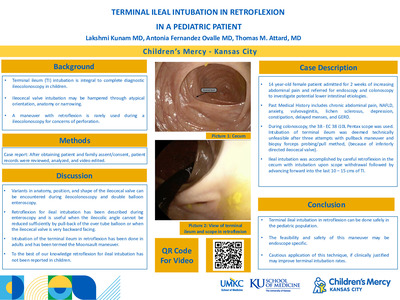
ackground: • Subacute massive pulmonary embolism (PE) is associated with high mortality. • The subacute presentation makes it difficult to diagnose and older clots are less amenable to systemic thrombolysis. • This can result into increased likelihood of recurrence and thromboembolic pulmonary hypertension Case description: • 17-year-old, previously healthy male presented with a month of exertional dyspnea, initially misdiagnosed with asthma. • CT demonstrated diffuse PE on repeat presentation (Fig1). • Echocardiography demonstrated moderate to severe RV dilation and systolic dysfunction and suggested an RV systolic pressure of 73mmHg + RAP. • He was subsequently admitted to the ICU and received a day of r-TPA therapy. • Repeat echocardiogram showed improved RVSP and RV function, and he was started on rivaroxaban. • 3 months later he had increased dyspnea with NYHA Class III symptoms • An echocardiogram demonstrated worsened RV function and pressure, although repeat CT suggested improved PE burden (Fig. 2). • Cardiac catheterization revealed a cardiac index of 1.75 L/min/m2 and PVR of 23 Wood Units * m2 (Fig 3). • He arrested during catheterization and was placed on ECMO. • Alteplase, angioplasty and stenting were attempted, and he was referred for pulmonary endarterectomy at another institution. • He developed acute renal and hepatic failure and ultimately succumbed to his death. Conclusion: Thromboembolic pulmonary hypertension can develop subacutely yet progress rapidly. It is often diagnosed late and has a high mortality rate; therefore, high index of clinical suspicion and prompt treatment is imperative. Disclosure: The authors of this case report have no financial disclosures. Fig 1: CT at initial presentation demonstrating widespread PE with multiple filling defects seen throughout the segmental pulmonary arteries to all lobes of both lungs Fig 2: CT 3 months later, significant obstruction of the distal pulmonary vasculature bilaterally and pruning, giving a false impression of improved clot burden Fig 3: (a) Cath angiography on the first day of readmission (3 month post initial presentation, showing significant obstruction of the right lobar arteries and severely attenuated peripheral pulmonary vasculature. (b) cath angiography on the following day showing rapid progression with almost absent peripheral vascular flow.
-

“ECMO IN A BAG”: Successful Adaptation and Implementation of a Novel Conference Idea
Johanna I. Orrick, Debra E. Newton, Kari L. Davidson, Jenna Miller, and Alyssa Stoner
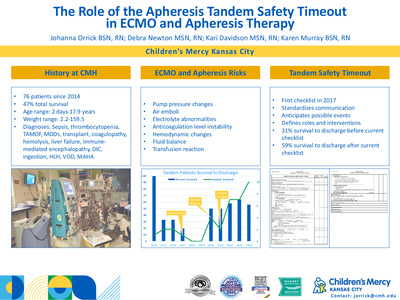
INTRODUCTION: Extracorporeal Membrane Oxygenation (ECMO) is an ever-evolving technical landscape that requires an advanced level of education. At our institution, a 367-bed pediatric teaching and research facility, learners include registered nurses, registered respiratory therapists, advanced practice registered nurses, resident physicians, pediatric and neonatal intensive care physicians. A certification class followed by an advanced course covers ECMO diagnoses, complications, equipment, and management prior to providing care for ECMO patients in our institution. Educational strategies include high and low fidelity simulations, didactic learning, and clinical hours at the bedside. A desire to increase the experiential learning opportunities was identified as an ECMO leadership goal. In 2018, a team member attended a conference and returned with a low fidelity simulation concept “ECMO in a Bag” from The Hospital for Sick Children in Toronto, Canada. This novel educational concept was subsequently adapted into a dynamic experiential teaching tool that met the interactive learning needs of the Children’s Mercy ECMO educational curriculum. METHODS: The “ECMO in a Bag” concept was first observed in May 2018 at the International Pediatric Simulation Society Workshop. The first version for our hospital was established with laminated equipment photographs and labels in September 2018 and was expanded upon in November 2018 to include non-sterile tubing to connect the photographs together schematically. The tubing, photos, and labels were intended to be used as an assessment for early ECMO learners. Introduction of “ECMO in a Bag” occurred in the August 2019 ECMO certification course. Modifications were implemented to develop an “Introductory ECMO in a Bag” after observations of the novice course participants deemed the task too difficult. In February 2020, the Advanced ECMO course utilized “ECMO in a Bag” in its original version for advanced learners. The class was divided into two teams and then competed against each other to correctly “assemble” an ECMO pump. All participants completed post surveys for each educational experience. RESULTS: When the original “ECMO in a Bag” was applied to 10 novice ECMO learners in August 2019 it was regarded as too difficult by the coordinators. The strategy was modified in the moment, using the laminated equipment names matched to an already assembled nonsterile ECMO pump along with definitions. The revised “Introductory ECMO in a Bag” has since been repeated in the ECMO certification course of 15 learners in August 2020. One hundred percent of the novice learners in both the 2019 and 2020 introductory class surveyed stated the hands-on sessions including “ECMO in a Bag” were effective and engaging. Quotes from the post class surveys included “I really enjoyed the breakout session looking at the circuit. Great to start understanding all of the circuit components,” “Hands on visualization was great, allowed for putting information together”. Additional positive feedback was gleaned from the application of the original “ECMO in a Bag” during the Advanced ECMO courses. One hundred percent of the transitional learners surveyed scored the hands-on portion of ECMO learning as beneficial. Comments included “Enjoy breaking up the talks with hands on activities,” and “I enjoy the games! It really breaks up the day.” DISCUSSION: The evolution of the experiential concept of “ECMO in a Bag” has been well received and is ongoing. It has been adapted for two different levels of ECMO learners in our hospital.. It is now used with resident physicians as well during shadowing experiences with the ECMO team. ECMO coordinators also use “ECMO in a Bag” to teach new critical care bedside nurse
-

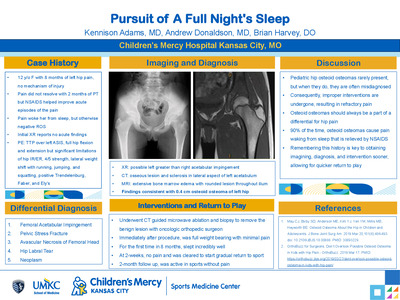
A unique cause of elbow pain and loss of range of motion in a 13-year-old
Thomas Munro and Brian S. Harvey
A 13-year-old right hand dominant young lady presented to a pediatric sports medicine clinic for evaluation of decreased ROM and pain in her left elbow with an associated locking sensation that had been occurring for over a year. Two weeks prior to presentation, these symptoms had been acutely worsening as she was practicing for over 10 hours per day for an upcoming dance competition. The patient’s pain is described as a “tightness” and is localized to her antecubital fossa medial to her biceps tendon. The feeling of tightness occurs most prominently with end extension and flexion of the elbow. She has had no associated fever, chills, fatigue, weight loss, swelling, bruising, numbness, tingling, previous reported injury in her elbow, or other pain or mechanical symptoms in any other joint. On exam the patient lacked 5-10° of full extension of the elbow on the left while exhibiting 5° of hyperextension on the right. She is tender to palpation (TTP) over the proximal ulna, flexor tendon mass, capitellum, and biceps tendon as it crosses the antecubital fossa. She is not TTP over the medial epicondyle, lateral epicondyle, olecranon, distal ulna, or on any region of the radius. Initial differential remained broad and included biceps tendinopathy, osteochondritis dissecans, subluxation, dislocation, occult fracture, osteochondroma, osteoarthritis, inflammatory arthritis, and heterotrophic ossification, among other possible etiologies. Frontal, oblique and lateral views of the left elbow showed multiple small heterogeneous calcifications in the antecubital space (the largest measuring approximately 1 cm in greatest diameter). No joint effusion, fracture, or dislocation were present. Soft tissue calcifications are caused by a wide range of pathologies, which can be grouped broadly into dystrophic, iatrogenic, metabolic, connective tissue disease, metastatic, and idiopathic causes. To further elucidate these calcifications an MRI with and without contrast of the left elbow was obtained. The MRI showed a Venous Malformation (VM) with associated phleboliths located anterior to the distal humeral diaphysis, in the region of the posterior aspect of the brachialis muscle, with an associated small intraosseous component in the humerus. VMs are present at birth and grow proportionately as the child develops. They are typically cutaneous, subcutaneous, or mucosal but can be located anywhere throughout the body. VM symptom presentation is highly variable and will often become symptomatic later in life. Treatment is controversial and options include symptomatic support (compression or NSAIDS), surgery, sclerotherapy, and possibly targeted therapy with sirolimus. In this instance the patient was referred to orthopedic surgery and vascular malformation clinic for further management. This case showed Venous Malformation to be a rare cause of elbow pain with associated decreased ROM and a locking sensation in a 13-year-old female patient.
-

Development and Interim Analysis of a Cystic Fibrosis-Specific Antibiogram
Claire Elson, Ellen Meier, Douglas Swanson, Rangaraj Selvarangan, Megan Gripka, and Christopher M. Oermann
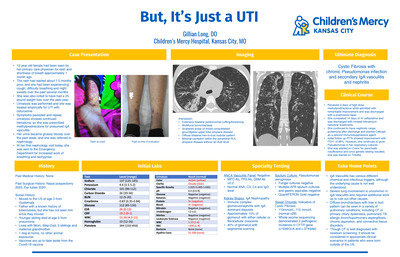
Antimicrobial therapy is essential to treat cystic fibrosis (CF) lung infections. Empiric antimicrobial selection is generally based on previous culture information and, if available, an institution-specific antibiogram (ABGM). Most institutions antibiograms exclude cultures from individuals with cystic fibrosis, imposing challenges with empiric antimicrobial selection and monitoring susceptibility patterns over time. A cystic fibrosis-specific antibiogram may help drive population-specific antimicrobial selection and improve antimicrobial stewardship.
-

Development of Drive-Through and Mail-In Systems for Obtaining Surveillance Respiratory Specimens in a Pediatric Cystic Fibrosis Center
Ellen Meier, Paula Capel, and Christopher M. Oermann
Routine surveillance cultures are an essential part of health maintenance for people with cystic fibrosis (CF). The Cystic Fibrosis Foundations (CFF) recommends that respiratory cultures be obtained every three months. The CF Care Center at Children’s Mercy Kansas City (CMKC) also obtains respiratory cultures when there is an acute change in respiratory symptoms. The COVID-29 pandemic resulted in ambulatory clinic closures and an inability to obtain surveillance respiratory cultures. A creative solution for obtaining respiratory cultures was needed during the pandemic.
-

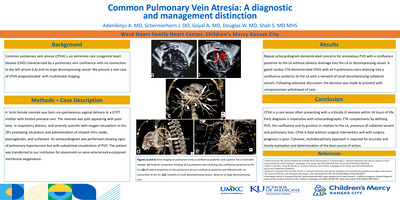
Incidental Diagnosis of Dual Arterial Supply of the Right Lower Lobe
Christopher Mathis, Jay Crockett, and Maria Kiaffas
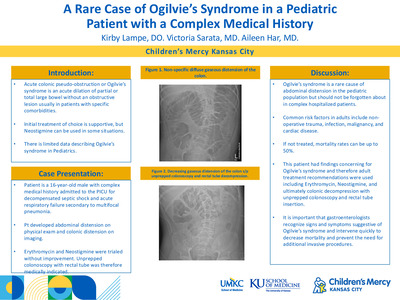
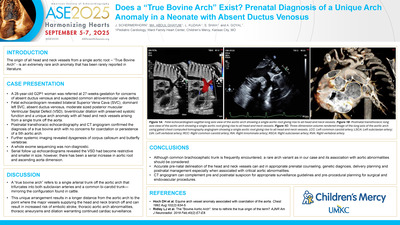
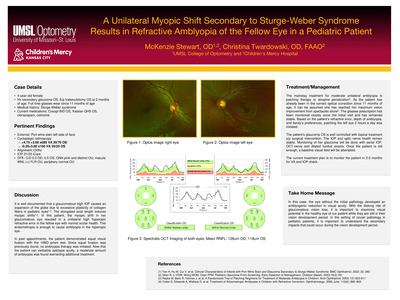
Description of Clinical Presentation: A 15 year old male with a 2 week history of fever and abdominal pain had an abdominal/pelvic MRI demonstrating osteomyelitis of his right hip. Incidentally an anomalous vessel arising from the abdominal aorta and coursing to the vasculature of the lower right lung lobe was identified and he was referred to cardiology for further evaluation. He is an athlete with no history of cardiac or respiratory symptoms and his cardiac physical examination was within normal limits. Diagnostic Techniques and Their Most Important Findings: An echocardiogram was initially obtained; imaging was difficult due to suboptimal acoustic windows and revealed normal intracardiac anatomy and normal ventricular size and systolic function. Detailed profile of the right pulmonary venous connections was not feasible and an abnormal flow close to the inferior vena directed towards the thoracic cavity was seen. The suspicion of an anomaly involving the right lung vasculature was raised and a cardiac MRI (CMRI) was obtained in order to better assess cardiovascular anatomy and calculate Qp:Qs. CMRI revealed an anomalous systemic arterial supply of a small portion of the right lower lobe without pulmonary sequestration. The artery originated from the celiac trunk with proximal narrowing of the vessel close to its origin and post-stenotic dilation. There was normal right pulmonary artery arborization and supply to this segment, indicating dual arterial supply. Qp:Qs was normal (1.03) with normal atrial and ventricular volumes indicating minimal extracardiac shunt. Learning Points from this Case: Incidental MR imaging findings are not uncommon and further imaging work-up as well as management should be individualized. In this case a systemic arterial supply to the right lower lung was inadvertently identified and further imaging revealed no hemodynamic burden associated with it. Various case reports address similar incidental discoveries, usually associated with work-up for hemoptysis, congenital heart disease and often associated with lung sequestration. Ligation or embolization of the systemic feeding vessel to the lung due to risk of hemoptysis is often undertaken. In the case of our patient, the morphology of the feeding vessel in combination with normal lung appearance, normal Qp:Qs, and lack of symptoms led to a consensus to not intervene but to observe with regular follow-up.
-

An Unexpected Global Health Experience in Manila
Susan McAnany
Describes her experience in the NICU of the Fabella Memorial Hospital in Manila, Philippines.
-
: Maseru, Lesotho by Whitney J. Cameron")
Baylor International Pediatric AIDS Initiative (BIPAI): Maseru, Lesotho
Whitney J. Cameron
Describes her experience working in Maseru, Lesotho.
-

FIT Clinical Decision-Making: Brain abscess in a nonfenestrated Fontan patient
Bethany Runkel, Natalie Shwaish, Geetha Raghuveer, and William Drake
-

FIT Clinical Decision-Making: Isolated polymorphic ventricular tachycardia in a pediatric patient: an unusual presentation of acute mycocarditis
Natalie S. Shwaish, Bethany Runkel, and Lindsey Malloy-Walton
-

FIT Clinical Decision-Making: Uhl's anomaly: an uncommon cause of fetal cardiomegaly
Bethany Runkel, Atif Ahmed, Tara Swanson, and Maria Kiaffas
-

FIT Clinical Decision-Making Unusual echocardiographic findings of myocarditis mimicking an aortic runoff lesion
Sarah Studyvin, Christine Symes, Barbara A. Pahud, and Nitin Madan
-

Global Health Elective in Santiago Atitlan, Guatemala
Sarah Greenberg
Describes her experience working in Hospitalito Atitlan in Santiago Atitlan, Guatemala.
-

Global Health Immersive Elective in the Philippines
Lisa Godfrey
Describes her experiences working at Fabella Memorial NICU and the Philippines General Hospital.
-

Medicine and Culture Abroad: Lago de Atitlan, Guatemala
Micah Helton
Describes her experience working alongside a Guatemalan General Practice Physician in Lago de Atitlan, Guatemala.
-

Philippines: An Int-ERUPTED Experience
Susamita Kesh
Describes her experience working in the NICU of the Fabella Memorial Hospital in Philippines.
-

Two Months of Global Health in Maseru, Lesotho
Rachel Hildebrand
Describes her experience working with infants and children at the Center of Excellence and Adolescents at Queen Mamohato Memorial Hospital in Maseru, Lesotho.
-

How to use Peanut IgE Levels to Predict Challenge Outcomes in the Pediatric Population
Nalin U.G., Jay Portnoy, Jodi Shroba, and Salman Aljubran
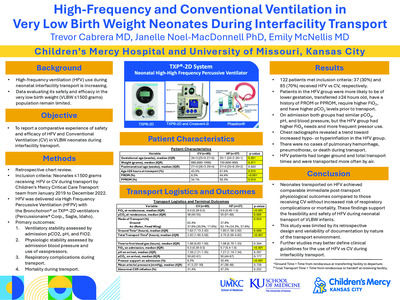
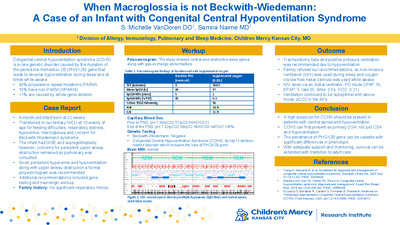
Introduction: The accepted clinical practice is to consider oral challenge when peanut IgE levels are 2.0 kUA/L or less in patients with a history of a major reaction or less than 5.0 kUA/L in patients with only sensitization. Certain populations are predisposed to having increased IgE levels, and these patients are often not offered challenges due to elevated numbers.
Methods: We reviewed unidentified patients information from January 2017 to July 2019 on peanut IgE levels and oral challenge outcomes through REDCap database. A ROC using SPSS from IBM was used and the points from the ROC curve were used to make an exponential regression curve. Since the likelihood ratio is the derivative of the ROC, the derivate of the graph was obtained.
Results: There were 106 peanut challenges (56 passed and 47 failed). The ROC points created an exponential regression of 0.417x ˇ 2 + 0.2943x + 0.0083 with an r value of 0.9072. The area under the curve was 0.702 (CI 0.601-0.803). The derivative was 0.834x+0.2943, which represents the likelihood ratio. Thus, solving the equation IgE ¼ (likelihood ratio-0.2943)/0.834.
Conclusion: It is important to remember that every patient is different, and the risk associated with oral challenge varies based on the clinical history. Using the likelihood ratio as opposed to a set threshold IgE level could enable us to better predict the possibility of a reaction with a more dynamic IgE cutoff. By using the patientspecific likelihood ratio, we were able to find an equation to allow us to calculate more meaningful IgE cutoff.
-

Standardizing Aminoglycoside Induced Ototoxicity Monitoring
Claire Elson, Christopher M. Oermann, Stephanie Duehlmeyer, and Ellen Meier
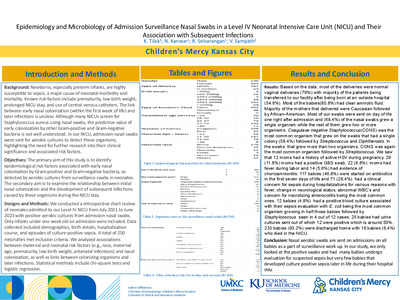
Aminoglycoside (AG) antibiotics are essential for the treatment of cystic fibrosis (CF) lung infections. Pseudomonas aeruginosa. Nontuberculous mycobacteria. Monitoring is critical secondary to potential nephrotoxicity and ototoxicity. Children’s Mercy Kansas City (CMKC), standardized nephrotoxicity monitoring in 2016. Observed variable ototoxicity monitoring practices. Prevalence of ototoxicity, 2016 CFF Patient Registry, 1.1% in pediatric patients (less than or equal to 18 years). 2.2% in pediatric and adult population. National Institute of Deafness and Other Communication Disorders, 13% in US population equal to or less than 12 years old. A standardized AG induced ototoxicity monitoring algorithm (AIOA) was developed and implemented at CMKC in 2017.
-

Teaching Skills for Self Sufficiency: Health Management for Patients with Disabilities and Chronic Health Conditions
Teresa M. Hickam and Kathy Smith
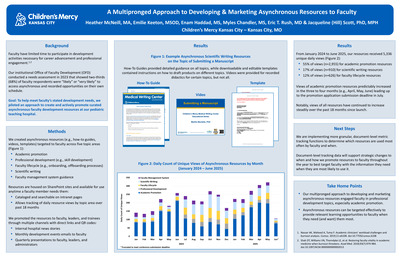
Research shows patients who develop self-health management skills are able to translate these skills in other life domains such as higher education, social interaction and employment. Persons with chronic health conditions or disabilities often face challenges securing employment which in turn impacts self sufficiency and long-term health. The poster focuses on two programs at Children's Mercy serving as key building blocks for adolescents to manage their lives.
-

6 Hall Team Norms: It's Our Patient
Mallory Rittel, Markeyta Brown, Ron Chenoweth, Marcy Page, Chelsi Peterzalek, and Amanda Woldruff
Aim Statement
6 Hall will increase NDNQI RN-RN interaction scores from 5.06 to 5.45 to meet the 2019 National Magnet Facilities benchmark b August 1, 2019.
6 Hall Team Norms
- We strive for excellence: our work is complex, mistakes will happen.
- We provide timely (<1>week) feedback, which includes positive, learning and interpersonal feedback.
- We celebrate as a team and our environment feels like every individual matters.
- When trust is broken, we ask ourselves: how did I contribute? What can I do to make it better? We are careful in not making assumptions.
- Our behaviors are supportive and display respect.
- We create a work environment that feels consistently awesome.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}