
These posters have been presented at meetings in Children's Mercy and around the world. They represent research that was done at the time they were created, and may not represent medical knowledge or practice as it exists at the time viewers access these posters.
-

A Multifaceted Approach to Improve Quarterly Visit Rates at a Pediatric Cystic Fibrosis Care Center
Paula Capel, Jessica Banks, Micaela McKenna, Ashley Andrews, and Christopher M. Oermann
Standard quality improvement methodology was used to improve quarterly visit rates among cystic fibrosis patients at Children's Mercy Kansas City Cystic Fibrosis Center.
- A family-centered, team-based approach was adopted
- A change in culture led to sustained improvement
Improved quarterly visit rates should drive improvement in outcomes including pulmonary function and nutritional status.
-

Assessment and Improvement of Data Collection Errors Through Inter-departmental Collaboration
Charlott Williams, Kelli L. Behr, Mary Moffatt, and Rangaraj Selvarangan
Specific Aims:
- To maintain the ED team's high rate of accuracy in data collection
- To begin team participation in corrective action planning
- To improve interdepartmental problem solving
Conclusion
Open communication about errors among all collaborating departments, combing with a shared approach to solving them:
- improved morale and perception of error tracking by the team
- led to a decrease in errors overall, and
- increased interdepartmental collaboration
When all members of the interdepartmental team work together with a positive approach to corrective action, improvement in error rates is a natural outcome of the solutions derived.
-

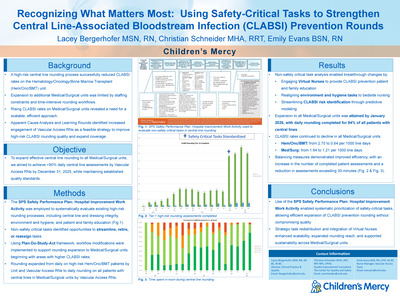
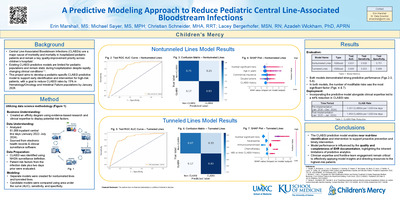
CLABSI Prevention through Prevention Huddles and CLABSI Risk Assessment and Prevention Form in Electronic Medical Record
Tara Benton, Barb Haney, Lacey Bergerhofer, Yolanda Ballam, and Kaitlyn Hoch
Our aim is to increase the awareness of high risks for central line associated bloodstream infection (CLABSI) and decrease the CLABSI rate with the implementation of CLABSI prevention huddles and an electronic medical record (EMR) "CLABSI Risk Assessment and Prevention" form.
-

Collaboration Between Rheumatology Clinic and Specialty Pharmacy to Positively Impact Patient Experience and Hospital Stewardship
Alaina Linafelter, Julia G. Harris, Robert Herr, Stephanie Quinn, and Ashley M. Cooper
Biologic medications are commonly utilized to treat pediatric rheumatic diseases. Being high-cost, most third-party payers require dispensing through a specialty pharmacy. Children's Mercy Hospital Specialty Pharmacy (CMH SP) started acceting patients in March 2015.
The number of patients benefited by the superior service of CMH SP has risen steadily, leading to high patient satisfaction and financial benefits for the hospital.
-

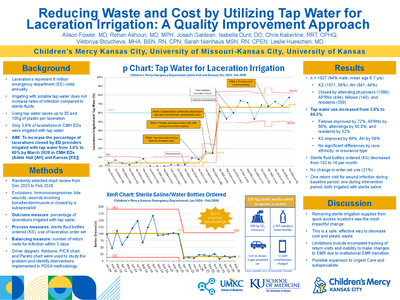
Decreasing Length of Stay in Pediatric Urgent Care with Electronic Discharge Instructions
Jennifer Wooster, Aimy Patel, Brian R. Lee, and Amanda Nedved
Time spent waiting in the urgent care clinic is dissatisfying for patient and staff. This "wasted time" accounted for more than 52% of the urgent care visit at our urgent care.
The aim of our project is to decrease length of stay by 10 minutes by April 30, 2019 for all patients discharged from Blue Valley Urgent Care by offering patients a paperless depart process. To be eligible for discharge without paper families must be enrolled in the online patient portal.
Electronic discharge instructions significantly decrease length of stay and is associated with improved patient experience scores. Patients who received hardcopy discharge instructions also had short median LOS, likely due to overall improved urgent care workflow with the use of the portal.
-

Development and Implementation of an Evidence-Based Process for Scarce Resource Allocation
Richard K. Ogden Jr., Daniel L. Millspaugh, and Brian O'Neal
Background: Intravenous immune globulin (IVIG) is a plasma-derived product from pooled donors. It has six FDA approved indications. It is also considered standard of care for a few other conditions in specific populations. Additionally, there is growing non-evidence-based use. Due to a global shortage, IVIG has become increasing difficult to obtain.
. . . .
Conclusions: Development, implementation, and promotion of adherence to an evidence-based criterion allowed our scarce IVIG supply to be sustained. Further refinement of the criteria for use is ongoing, as is an evaluation of IVIG utilization by indication, pre- and post-implementation. This process can be applied to other situations of scarce resources
-

Implementing Treat to Target Approach in the Care of Children with Juvenile Idiopathic Arthritis
Julia G. Harris, Jamie Holland, Emily Fox, Leslie Favier, and Ashley M. Cooper
Juvenile idiopathic arthritis (JIA) is the most common chronic inflammatory disease seen in pediatric rheumatology. Despite advances in biologic therapy, many children with JIA will experience morbidity. Treat to Target is a treatment paradigm that involves setting a target of disease activity, using shared decision making, and incorporating clinical decision support. Our clinic aimed to set a treatment target on 50% of eligible JIA patients by December 31, 2019.
-
 Projects by Beckie Palmer, Sarah Carboneau, Ashley Domsch, Barb Haney, Brandy Huitt, Ashley Lewis, Ashley Mirabile, Allison Ronco, and Dianne Wilderson")
Improving Bedside Nurse Engagement in Quality Improvement (QI) Projects
Beckie Palmer, Sarah Carboneau, Ashley Domsch, Barb Haney, Brandy Huitt, Ashley Lewis, Ashley Mirabile, Allison Ronco, and Dianne Wilderson
Project Aims:
- Improve nursing engagement in QI as evidenced by increasing nurse involvement to 40% of overall staff by December 2018, with a continual increase to >50% by June 2019.
- Decrease the % of nurses who express "my opinion doesn't matter" as a reason they do not participate in QI by 30% by June 2019.
-

Improving Care of the Small Baby
Beckie Palmer, Abdebayo Oshodi, Brandy Huitt, Kaylee Hurt, Pamela Kliethermes, Trudy Koons, Patricia Lanzer, Ashley Mirabile, Allyson Owen, Christian Anthony Schneider, Betsi Anderson, and Steven Olsen
Hierarchy of Aims:
- Global Aim: Create a Small Baby Unit for infants admitted to our NICU that arebirth, in which 90% of our patients are admitted to F pod on day of admission, by March 2019
- Interim Aim: Staff 80% of our micropremie patients with a Small Baby Team nurse from admission until >32 weeks by May 2019.
- Sub Aim: Increase rates of developmentally appropriate care (2 person cares, kangaroo care compliance) by 50% by August 2019.
-

Improving End Stage Renal Disease Quality Incentive Payment Total Performance Scores
Shelly Guyer, Gina Gregg, and Bradley Warady
The End Stage Rena Disease (ESRD) Quality Incentive Program (QIP) promotes high quality, transparent, cost-efficient care in outpatient dialysis facilities by establishing performance standards that are linked to payment.
The development of a subject matter expert and the sharing of ESRD QIP knowledge resulted in buy-in from dialysis staff and physicians leading to a higher total performance score and the avoidance of payment reduction.
-

Improving Malnutrition Identification in the Outpatient Setting
Kristi Thaete and Karen Stephens
Identification of Pediatric Malnutrition in Outpatient Clinics is the First Step to Allowing Registered Dietitian (RD) Involvement in the Improvement of Patient Care.
-

Improving Pneumococcal Vaccination Rates in High Risk Patients Across Multiple Specialty Divisions
Rachel Moran, Julia G. Harris, Claire Olsen, Rana El Feghaly, Liset Olarte, Douglas Blowey, and Luke A. Harris
Pediatric patients with deficient immune systems or certain chronic medical conditions have an increased risk of acquiring invasive pneumococcal disease.
The 23-valent pneumococcal (PPSV23) vaccine provides protection against 23 pneumococcal serotypes and is recommended for patients aged 2 years or older who are high-risk for invasive pneumococcal disease.
Unfortunately, many high-risk patients are not properly vaccinated due to lack of provider knowledge or understanding of accountability between primary care and specialty providers.
The goal of this project was to improve PPSV23 vaccination rates by 10-20% across multiple Children's Mercy Kansas City specialty divisions.
-

Improving Women, Infants, and Children Participation Using Quality Improvement Methodology
Samuel Little, Sarah Stone, Jeffrey D. Colvin, Sidney Smith, Brenda Hilboldt, Laura Williams, Patricia Marein, Keith Mann, and Kristi Williams
Food insecurity, when a household is unable to acquire food for one or more of its members due to insufficient resources, has recently been on the decline in the United States, according to official 2017 USDA reports.
Unfortunately, this decline has not been observed to the same extent in the demographic of households with children.
WIC is a federal assistance program that works to alleviate the poor health outcomes associated with food insecurity in this demographic by providing eligible, enrolled families with nutritional aid and education.
The specific aim of the project is to increase the percentage of maximum potential WIC appointments that are attended to 85% within 9 months, thus improving nutritional health for eligible individuals within the community.
-

Increasing Kangaroo Care in a New Small Baby Unit
Dianne Wilderson; Barb Haney; Ashley Mirabile; Beckie Palmer; Jenny Heltzer; Erin Keith-Chancy BSN,CCRN; Brooke Smith; Christian Anthony Schneider; and Abdebayo Oshodi
Project Aim: Increase the percent of eligible patients receiving kangaroo care from 19% to 30% by September 2019.
Results:
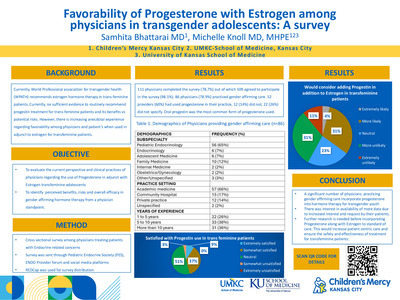
113 staff completed education
OT consults completed on all SBU patients
20 kangaroo wraps purchased
Kangaroo care rate in NICU increased from 19% (prior to SBU) to 36% (Post SBU opening).
Conclusion: Due to increased multidisciplinary awareness of importance of kangaroo care in the SBU more parents are completing kangaroo care.
-
 Discharge: An Improvement Project in a Midwest Level IV NICU by Kathleen Hortenstine, Teresa Fulk, Stephanie Callis, Kyla Galate, and Beckie Palmer")
Increasing Rates of Breastmilk Use at Time of Neonatal Intensive Care Unit (NICU) Discharge: An Improvement Project in a Midwest Level IV NICU
Kathleen Hortenstine, Teresa Fulk, Stephanie Callis, Kyla Galate, and Beckie Palmer
- Breast milk is the preferred food for all infants.
- The rate of breast milk use at time of discharge was below the goal of the institution.
- A gap was identified in bedside nursing education, limiting their ability to provide resources and education to mothers. Nursing involvement ensures skilled, comprehensive, and accessible breastfeeding support.
- The aim of this project is to increase breast milk rates at time of NICU discharge to 95% of eligible patients by December of 2019.
-

Lighting the Way to Ensure Safe Transition Home
Barb Haney, Ashley Mirabile, Dianne Wilderson, Beckie Palmer, Ashley Lewis, Cris Mills, and Eugenia K. Pallotto
All aspects of discharge (education, screenings, appointments, plans and home services" must be completed and appropriately communicated prior to discharge to ensure safe transition to home.
Goal: Standardize all aspects of discharge in a large, busy 84-bed Level IV NICU with >1000 admissions/year and >300 nurses, >60 NNPs, and >25 neonatologists.
- 95% of patients with lengths of stay >3 days have all discharge planning completed prior to discharge/Parent Care Unit overnight stay
-

Making the Management of Acute Otitis Media a SNAP
Cassandra Newell, Donna Wyly, Tanis Stewart, Alaina N. Burns, Brian R. Lee, and Rana El Feghaly
AIM:
To improve Watchful Waiting or Safety Net Antibiotic Prescription (WW/SNAP) in children >6 months old diagnosed with acute otitis media by Advanced Practice Nurses in the Emergency Department by May 2020.
-

Optimizing Antibiotic Management of Pediatric Acute Otitis Media in an Emergency Department
Alicia Daggett, Alaina N. Burns, Brian R. Lee, Nirav Shastri, Patricia Phillips, and Rana E. El Feghaly
Problem
Children diagnosed with acute otitis media (AOM) at the Children's Mercy Hospital Kansas Emergency Department routinely get antibiotic prescriptions. There is rarely discussion with families about watchful waiting (defined as discussion of observation with parents and providing a safety-net antibiotic prescription that parents can ill if the patient is not improving or is worsening over the next 48 hours).
The aim of this quality improvement project is to increase watchful waiting for AOM at the CMK ED by 20% by March 2020, with an overall goal of decreasing antibiotic use for AOM.
-

Pediatric Surgery Opioid Prescription Follow-up
Gadison Quick, Nathaniel Aviles, Gabriel Melgarejo, Hunjung Choi, and Elizabeth Edmundson
This quality improvement project is assisting general and orthopedic surgeons in gaining greater clarity when prescribing opioids for specific surgical procedures. Additional surgical services are being added to the project fall of 2019. Opioid prescribing patterns are, and will continue to be, key to all prescribing providers within our organization.
-

Safe Sleep in the NICU
Ashley Mirabile, Barb Haney, Dianne Wilderson, Beckie Palmer, Ashley Domsch, and Eugenia K. Pallotto
Goal: To evaluate a staff education program on approach to improve in the rate of eligible NICU infants in safe sleep in a busy 84-bed level IV NICU.
Outcome Measures; Improve safe sleep compliance for eligible patients to 90% or greater by December 2019.
Process Measures: Audits from bedside RNs showing compliance with safe sleep.
Planned Intervention: In December of 2018 a multidisciplinary work group brainstormed and implemented best practice safe sleep education for staff and parents. September 2019 a Safe Sleep Educational Toolkit was made available for staff.
Results: Safe Sleep compliance has gone from 53% to 90% in September of 2019 after the initiation of a safe sleep toolkit.
-
 Van Noy, Molly Kruse, Megan English, Hannah Culbertson, Brianne Truitt, Ziryan Salihparkhy, Jenny McKee, and Brecklyn Findley")
Safe to Sleep in the ICN
Megan Kelly, Alexandra (Lexi) Van Noy, Molly Kruse, Megan English, Hannah Culbertson, Brianne Truitt, Ziryan Salihparkhy, Jenny McKee, and Brecklyn Findley
The CDC states that 1,545 infants passed away from SIDS in 2014. Safe sleep includes supine, in a crib, head of bed flat, firm sleep surface, tightly fitted sheet, no loose blankets, no toys or supplies in crib with infant. It is important for nurses to model safe sleep practices in the hospital setting. Current compliance with safe sleep in the Intensive Care Nursery is 50%.
AIM Statement:
By August 1, 2019 we want to increase the compliance of modeling safe sleep behaviors for patients who qualify for safe sleep from 50% to 90% in the Intensive Care Nursery.
-

The Kanga-Croo: Nurse Resident Champions Creating Momentum for Improvement
Brett Butler, Jacob Burden, Carly Creekmore, Blair Griffin, Taylor Godemann, Taylor Hagen, Theresa Koelling, Mary Anne Kucera, Halle Magid, Makenna Miller, Monica Page, Mary Riffel, Madison Stebbins, Sarah Stokes, and Skylar Suppes
Topic Summary:
Kangaroo Care (skin to skin care) is a parent-led, evidence-based intervention which improves outcomes in neonatal patients including: decreased apnea, increased weight gain, increased parent satisfaction and decreased length of stay.
Results:
Nurse resident team interventions to support parent engagement and remove barriers to Kangaroo Care (KC) through iterative PDSA cycles from January 2018 to July 2019 yielded positive results within a subset of ICN patients.
-

Trauma Informed Care: Improving Staff Morale on 6 Henson
Kara Humphreys, Katherine Karstens, Kortney Neiderhauser, Briana Pina, Payton Tallent, Stephanie Assad, and Madison Dexter
Six Henson staff reported feeings of burnout and compassion fatigue.
Aim Statements:
Decrease percentage of 6 Henson staff feeling sometimes or often "worn out because of [their] work as a helper" from 86% to 50% by August 1, 2019.
Increase the number of KUDOS cards submitted by 6 Henson staff from 2-3 per week to 10 per week by August 3, 2019.
Both aim statements were met and exceeded.
-
 to Improve Communication Between Pediatric Urgent Care and Inpatient Providers by Amanda Nedved, Kathleen Berg, and Amanda Montalbano")
Using a Standardized Admission Handoff (I-PASS) to Improve Communication Between Pediatric Urgent Care and Inpatient Providers
Amanda Nedved, Kathleen Berg, and Amanda Montalbano
Ineffective hand-off communication is recognized as a critical patient safety problem in health care. A pre-interventions survey of pediatric urgent care providers and pediatric hospitalists demonstrated an opportunity for improvement of communication during admission handoffs.
Standardized handoffs improve communication without impeding provider workflow. We learned that subjective terms for illness severity ("stable," "watcher," and "unstable") did not translate well from urgent care to inpatient. We are planning on implementing an objective standardized tool (PEWS) to improve the communication of illness severity. We have also updated the I-PASS visual aid based on feedback.
-

"Will Using Telemedicine with Medical Command during Situational Awareness Escalation Add Value to Patient Care?"
Kathy Farrell, Bradley Bishop, Lisa Carney, Matthew B. Johnson, Natalie Masters, Lisa Pruitt, Sherry McCool, and Laura Fitzmaurice



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}