
These posters have been presented at meetings in Children's Mercy and around the world. They represent research that was done at the time they were created, and may not represent medical knowledge or practice as it exists at the time viewers access these posters.
-

Total and Free Plasma Bilirubin and Clinical Outcomes in Severe Hyperbilirubinemia
Sean M. Riordan, Jean-Baptiste LePichon, Steven Shapiro, Tina Slusher, Fatima Abdullahi, Hafsat M. Suleiman, Victor C. Pam, Mamu B. Samuel, Christopher S. Yilgwan, Christian Isichei, and Idris Y. Mohammed
Acute bilirubin encephalopathy (ABE) and kernicterus spectrum disorder (KSD) have become relatively uncommon in high income countries but remain a major cause of morbidity and mortality in low- and middle-income countries. To better understand the relationship between free (Bf) and total (TB) bilirubin levels and the development of ABE and KSD we followed infants born in three large tertiary centers in northern and central Nigeria (Jos, Kano and Zaria).
-

Weighted Pathway Genetic Load Analysis of Hyperbilirubinemic Infants Indicates a Potential Genetic Component for Susceptibility to Bilirubin Neurotoxicity
Sean M. Riordan, Jean-Baptiste LePichon, Steven Shapiro, John Cowden, Monica VillaGullen, Laurence Thielemans, Dina Villanueva Garcia, and Jesus Aguirre-Hernandez
Severe kernicterus spectrum disorder (KSD) is described as motor and auditory deficits resulting from brain damage caused by hyperbilirubinemia. The severity of HB does not always predict the severity of injury. The lack of a strong monogenetic link to susceptibility suggests bilirubin-induced brain damage may be due to impaired bilirubin response pathways. This poster describes work to use a modified pathway genetic load (mPGL) score method to perform a targeted genetic analysis of whole exome data from patients with various degrees of neonatal HB, with an ultimate goal of developing a neonatal screen to susceptibiltiy to bilirubin neurotoxicity.
-

Developing Technologically Advanced Research in Low- and Middle-Income Countries
Isa Abdulkadir, Tina Slusher, Fidelia Bode-Thomas, Sean Riordan, Jean-Baptiste LePichon, Laila Hassan, Shehu Abdullahi, Akinyemi Ofakunrin, Stephen Oguche, Steven Shapiro, and William Ogala
This poster presents a collaboration between a group of scientists in Nigeria and the USA in developing a genomic research project and the solutions adopted in tackling the ethical implications and partnership equity and ownership of such a project.
-
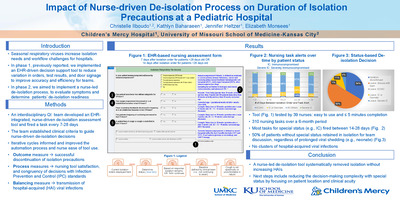
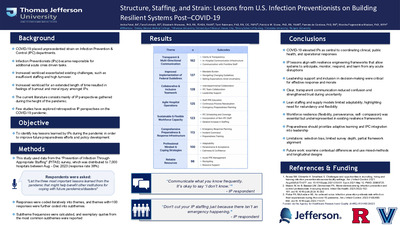
 Risk in a Single-Center Pediatric Academic Hospital by Elizabeth Monsees, Paul N. Bauer, Yolanda Ballam, and Brian R. Lee")
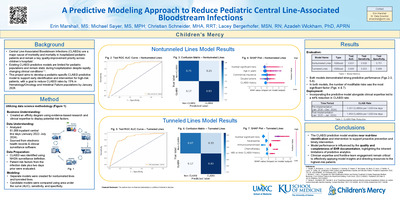
Identifying Structural Factors Associated with Central Line-Associated Bloodstream Infections (CLABSI) Risk in a Single-Center Pediatric Academic Hospital
Elizabeth Monsees, Paul N. Bauer, Yolanda Ballam, and Brian R. Lee
Objective: compare unit structure and process-related factors against unit-specific CLABSI rate.
Conclusion: CLABSI mitigation requires more than individual competence with task-related practices; the unique work ecology of each clinical area may broadly influence CLABSI as an outcome; extending analyses to consider organizational structure can inform resource allocation and recalibrate traditional prevention strategies.
-

Sepsis: Triage Triggers, Outcomes Quicker
Rylee Ainge, Mackenzie Flaws, Natalie Heim, Emily Herndon, Hayley Norris, and Amy L. Scott
-

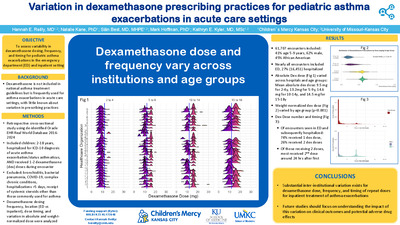
Analgesia and Sedation Medication Use in Infants with Congenital Diaphragmatic Hernia is Associated with Adverse Outcome
Mark Weems, Theresa Grover, Robert DiGeronimo, Jason Gien, Ruth Seabrook, Sarah Keene, Natalie Rintoul, Beverly Brozanski, John Daniel, Rachel Chapman, Burhan Mahmood, Yvette Johnson, Yigit Guner, Holly Hedrick, Isabella Zaniletti, and Karna Murthy
This study describes the use and variation of sedation and analgesic medications as well as short-term clinical outcomes in infants with congenital diaphragmatic hernia.
-

Association of Food Deserts and Pediatric Hospitalization Rates
Laura Plencner, Matthew Hall, Molly Krager, Henry T. Puls, Jessica L. Markham, Ellen Kerns, and Jessica L. Bettenhausen
Retrospective cross-sectional study describes differences in hospitalization rates for children based upon their residence within a food desert and describes any differences among reasons for hospitalization.
-

Burnout and Resilience Among Pediatric Residents in Stockholm, Sweden: Findings from a Mixed-Methods Study
Lauren Poull, Sanaz Skyttner-Rahmani, Andrea P. Anderson, Weston T. Powell, Jiaqi Yin, Carolyn C. Foster, and Maneesh Batra
Objective
To measure the prevalence of burnout among pediatric residents at Karolinska University Hospital (KUH).
To describe the local drivers of burnout and the protective factors that lead to resilience and workplace engagement.Conclusions
Prevalence of burnout among Swedish pediatric residents in this study was 39%, which is lower than reported in the US (50-60%).
Drivers of burnout were identified across all four domains. They included local features of the learning environment, and many are modifiable.
Protective factors include perceived control over scheduling, better mental and physical health, lower perceived stress, and being a parent.
Future work will evaluate interventions designed to modify the drivers of burnout and reinforce the drivers of resilience. -

Chenla Children's Healthcare in Kratie, Cambodia
Clayton Mowrer
Describes a global health learning experience in Kratie, Cambodia.
-

Choosing Catheter Sheath Introducers in Infants-Information You Are Not Provided but Should Have!
Christopher Mathis, Ryan Romans, and Abhay Divekar
Background: The advertised catheter sheath introducer (CSI) size, the internal diameter (ID), defines the maximum size of medical devices that can pass through it. However, the outer diameter (OD) determines the risk of vascular injury, varies considerably between manufacturers, and is not advertised. The highest risk of vascular injury is in infants less than one year of age and 3 - 6Fr CSIs are typically used.
Methods: The OD of 3, 3.3, 4, 5, and 6F CSIs (5 of each size) from different manufacturers were measured using a Mitutoyo Digital Micrometer. CSIs were measured with the dilator in place. Three authors measured the OD at the mid- and proximal portions (3 readings at each site) and were blinded to the other authors’ measurements. Continuous variables are reported as mean ± SD. Mid and proximal measurements were compared using an independent samples T test. Cronbach’s alpha and Intraclass Correlation Coefficient were used to measure the agreement for measurements between authors. Significance was set at P < .05.
Results: Based on our study there are significant differences in the OD of CSIs among manufacturers, and these are not advertised. There was no difference in the diameter of the CSI at the mid-point or proximally (P < .05). The intra-rater and inter-rater reliability were excellent (Cronbach’s Alpha 1.0 and Intraclass correlation coefficient 1.0). CSIs developed for transradial catheterization had the smallest OD when compared to traditional CSI (1F, 0.33 mm smaller). The OD of CSIs by Terumo Interventional Systems were on average 0.5F (0.17 mm) smaller than those from other manufacturers. The OD of the 4F transradial CSI by Merit Medical (Prelude IDeal, 1.610 ± 0.006 mm) is essentially the same as the OD of the 3F Elite HV Braun Interventional Systems (1.644 ± 0.016 mm), 3.3Fr PediaVascular (1.635 ± 0.005 mm) CSIs.
Conclusions: A smaller CSI does not guarantee a smaller OD. The OD of the 4F transradial CSI is the same as the OD of the 3Fr and 3.3Fr CSI. The “smaller” CSIs also require use of specially designed 3F catheters and 0.030-inch guidewire. On the other hand, the 4F CSI has the same OD but offers access to a wider assortment of well-established, commonly stocked, and cheaper 4F diagnostic and interventional tools. This is achieved without increasing the risk of vascular injury and may also help reduce catheterization laboratory inventory in the era of cost containment.
-

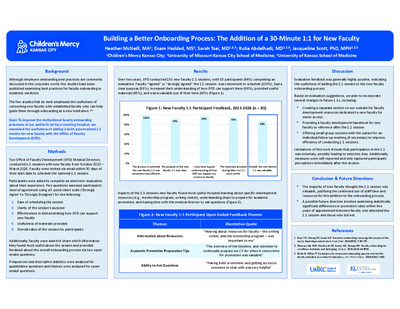
Creating Staff Engagement in Transition Planning Through the Use of Data
Teresa Hickam and Michelle Bozarth
In 2017 the Children's Mercy Kansas City Transition Program provided 14 Divisions and 28 programs with data to support their hard work. 2,160 of 3,768 patients (61%) completed readiness assessments and held transition-related discussions with their health care team.
Data reports providing timely, routine feedback on staff success and missed opportunities helps keep staff engaged, their efforts visible and transition planning on a conscious level.
-

Determining the Instructional Effectiveness of an Online Resident Vaccine Curriculum
S. Elizabeth Williams, Shannon Clark, Barbara A. Pahud, Sharon Humiston, Donald Middleton, and Kadriye O. Lewis
We developed four online modules through the Collaboration for Vaccine Education and Research (CoVER) project. The objective of this qualitative study is to determine the instructional effectiveness of the CoVER curriculum from the perspectives of medical residents.
-

Examining Nurse Resiliency & a Mindfulness-Based Stress Reduction Intervention to Prevent Nurse Burnout
Allegra Grannell
Nurses continually give of themselves at work, as well as outside of work. This results in extensive stress, physiological distress, and ultimately burnout for individuals in the nursing profession. Nurses that work in high-stress environments, such as critical care, pediatrics, and oncology, are at a significantly increased risk of manifesting physical and psychological symptoms of burnout syndrome, compassion fatigue, and post-traumatic stress disorder (PTSD). Many of these factors are leading to nurses leaving the profession prematurely, resulting in significantly high turnover rates. High burnout and turnover rates of nurses result in the lack of adequate nursing staff in hospitals, which in turn results in the inadequate ability to provide safe and effective care to patients. Resilience is a topic that has gained much discussion in recent years surrounding the significant burdens nurses are experiencing. Nurses with resilience exhibit a heightened awareness, internal stability, and flexibility that allow them to navigate high-stress situations. The goal of resilience training and education is to enable nurses to respond to clinically challenging situations in ways that will protect them against detrimental consequences. Mindfulness based stress reduction (MBSR) has gained significant headway in recent years as a valuable, evidence based intervention to increase resiliency in nurses, improve job satisfaction, and reduce burnout. The purpose of this quality improvement project was to implement a MBSR course for nursing staff to improve nurse resiliency in a mid-western freestanding Children’s hospital. This project examined nurse resiliency pre-intervention, and post-intervention utilizing the Connor-Davidson Resilience Scale, as well as compassion fatigue, compassion satisfaction, burnout, and secondary traumatic stress pre-intervention, and post-intervention using the Professional Quality of Life scale. Results of the project indicate that resilience scores improved, at a statistically significant level, from pre-intervention to post-intervention.
-

Gastroenterology Elective in the Philippines
Katie Black and Jennifer Watts
Recounts learning experiences while working at the Philippines Children's Medical Center in Manila.
-

General Philippine Hospital, Manila, Philippines
Cara Cecil
Describes her experience working in the Philippine General Hospital/University of the Philippines providing care in the pediatric ICU, neonatal ICU, and emergency department.
-

Global Health Elective in Rural Guatemala
Kendall Burns
Describes pediatric resident's experience learning to translate evidence based medicine to resource-limited areas in rural Guatemala.
-

Global Health Elective in San Pedro La Laguna, Guatemala
Page Pomo
Future outpatient general pediatrician serving bilingual populations describes working in rural Guatemala and opportunities to practice Spanish language skills.
-

Global Health Elective, Philippine Children's Medical Center
Keith J. Martin
Describes a global health learning experience working in the Philippine Children's Medical Center in Quezon City, Metro Manila, Philippines.
-

Global Health Elective: Santo Domingo, Dominican Republic
Joan Strong
Describes the experiences of a pediatric anesthesiology fellow's time working Medical Aid for Children of Latin America (MACLA) in Santo Domingo, Dominican Republic.
-

Global Health Elective: Trujillo, Peru
Naseem Nikaeen
Describes pediatric resident's learning experiences to provide better medical care in low resource environments.
-

Global Health Experience in Botswana
Sarah Bieser
Describes experience providing care at the Botswana-Baylor Children's Center of Excellence in Gabarone, Botswana and the Princess Marina Hospital.
-

Global Health Experience in Botswana
Jared Willard
Describes a global health learning experience at the Botswana Baylor Center of Excellence with emphasis on treating pediatric HIV/AIDS patients.
-

Global Health Experience in the Philippines
Nina Zanaboni
Describes experiences working in the Dr. Joe Fabella Memorial Hospital NICU and Philippine Children's Medical Center ER.
-

Global Health Experience: Laos Friends Hospital for Children
Ashley Daniel
Outlines the learning experiences of a pediatric resident working within the Laos Friends Hospital for Children.
-

Global Health Rotation Caring for Children with Medical Complexity in Russia
Irina G. Trifonova
Describes a global health learning experience in which a Russian-trained pediatrician completed a fellowship at Children's Mercy Kansas City and spent time at the City Children's Hospital #3 in Cheboksary, Russia to compare care models for children with medical complexity in Russia and the USA.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}