
These posters have been presented at meetings in Children's Mercy and around the world. They represent research that was done at the time they were created, and may not represent medical knowledge or practice as it exists at the time viewers access these posters.
-

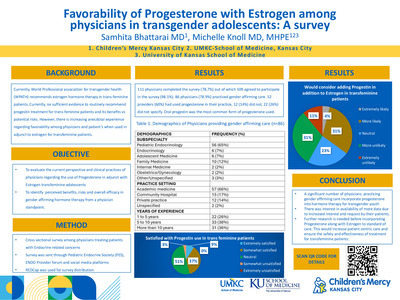
Thyrotoxicosis Presenting with Nondiabetic Ketoacidosis in a 4 Year Old Female: A Case Report
Henry S. Jeng, Michelle Knoll, and Figen Ugrasbul
Objective: To raise awareness that thyrotoxicosis should be on the differential diagnosis for ketoacidosis in the pediatric population
-

Health Literacy Challenges and Opportunities: Bringing Children’s Mercy and Kansas City Together
Jennifer A. Lyon, Angie Knackstedt, Barbra Rudder, Mamta Reddy MD, and Courtney R. Butler
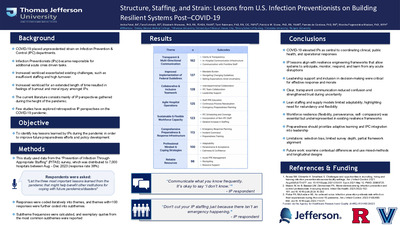
BACKGROUND: A multidisciplinary group at Children's Mercy Kansas City applied for and received the NNLM MCR's Immersive Workshop Grant in December, 2017, and used the funding to organize and host a two-day immersive, interprofessional workshop in April, 2018, that 1) brought together health literacy-invested groups and individuals within the Kansas City community to learn about health literacy including cultural, language, numeracy and digital inclusion factors; and 2) provided specialized training to targeted CM participants to improve the provision of bedside health information to patients and caregivers. Objectives included: increasing community-wide collaboration, sharing resources, encouraging participants to become change agents, and strategizing organizational initiatives. DESCRIPTION: The project team consisted of 2 librarians, a practicing physician, a child life specialist, and a nurse educator specializing in equity and diversity; all were past or present members of the institution's Health Literacy Committee. Day One, at the Public Library, was open to the community. Over 25 organizations involved with health literacy and health equity were invited to contribute speakers and participants. Dr. Ruth Parker of Emory University delivered two 'keynote' lectures. Other speakers represented an adult literacy volunteer agency, the Public Library, and an immigration support organization. Day Two was held internally, focusing on hospital employees professionally invested in promoting health literacy practices in patient care. Additional training on institution-specific resources was supplemented by interactive, hands-on practice sessions and brainstorming exercises intended to develop internal health literacy pilot projects, with encouragement to reconnect with the community organizations. CONCLUSIONS: Day One had 73 attendees (28% from the community). Day Two had 60 attendees. All participants were fully engaged throughout, including interactive brainstorming activities. All informal comments to organizers were positive and the planning team has received requests to repeat the workshop in the future. A survey was sent to all attendees (67-69% response rates). On a Likert scale from 1-5, the means on questions regarding health literacy awareness, motivation to take action, and increased knowledge of resources and collaboration opportunities ranged from 4.88-4.95 for both days. Internal projects are being developed and communication with external groups has steadily increased.
-

A NSQIP Analysis of Post-Operative Antibiotic Utilization in Uncomplicated Appendicitis
Charlene Dekonenko, Robert M. Dorman, Janelle R. Noel-Macdonnell, and Tolulope A. Oyetunji
APSA 2010 recommendations do not support antibiotic use post-operatively following appendectomy for uncomplicated appendicitis, but compliance varies by institution. This study determined the rate of post-operative antibiotic use in uncomplicated appendicitis and found that 10% of patients were discharged on antibiotics, using the NSQIP files.
-

A Review of First Year Fellow Endoscopic Skills and Time to Proficiency
Antoinette Adjowa O. Walker, Dalya El Tawil, Jennifer Colombo, Nicholas Clark, and Kimberly J. Reid
Through this quality improvement project, we have assessed the current fellows' upper endoscopy skill level during their first year and determined that the time to achieving proficiency is significantly longer than desired. The goal is to prepare new fellows for endoscopy prior to the beginning of their rotations with a curriculum that includes assigned reading materials, videos, and simulated endoscopic cases, to promote safety and increase satisfaction of patients by improving the readiness, skill level, and the confidence of first year inexperienced fellows.
-

A Unique Model for Palliative Care in a Level IV Neonatal Intensive Care Unit
Kelstan L. Ellis DO, Megan Tucker, and Jennifer Linebarger
This poster describes a review of the relationship between the Fetal Health Center and the Palliative Care team as the Palliative Care Team follows the patient family from prenatal through neonatal intensive care.
-

AV Nodal Reentrant Tachycardia in Patients with Twin AV Nodes
Christopher Mathis, Svjetlana Tisma-Dupanovic, Lindsey Malloy-Walton, and John Papagiannis
-

Dehydrated Hereditary Stomatocytosis Causing Sever Ascites Leading to Pulmonary Hypoplasia and Respiratory Insufficiency in a Neonate
Michael D. McDowell Jr and Christopher M. Oermann
Care Presentation: EM is a 32.5-week EGA infant who was born with sever congenital ascites (following repeated prenatal paracentesis) identified on prenatal ultrasound. Initial chest-abdomen imaging is shown in Figure 1. He required CPAP at delivery but was weaned of high flow nasal cannula with intermittent episodes of prolonged intubation during repeat paracentesis. Paracentesis demonstrated simple ascites rather than chylous fluid. Lymphangiograms demonstrated transient lymphatic leakage with resolution. Genetic evaluation revealed a pathogenic mutation in the PIEZO 1 gene for autosomal dominant DHS. This disorder had reduced penetrance and variable expressivity and symptoms range for absence of clinical features to lethal perinatal edema. During his first year of life EM developed severe chronic obstructive pulmonary disease with hypoxemia and a requirement for supplemental oxygen, restrictive lung disease secondary to thoracic dystrophy, and chronic lung disease of prematurity. He remained on supplemental oxygen for the first year and a half of life. Discussion: DHS is a rare form of autosomal dominant hemolytic anemia reported in 26 individuals among 7 families worldwide. Clinical presentation varies significantly and includes chronic anemia, neonatal edema and ascites, and lymphatic malformations. Symptoms may develop in utero, during the perinatal period , or later in adulthood. Pulmonary hypoplasia and respiratory insufficiency caused by pre/perinatal ascites have not been reported. DHS is caused by gain-of-function mutations in the PIEZO1 (16q24.3) gene, as was demonstrated in our patient. Mutations result in increased red cell cation membrane permeability, particularly potassium, leading to depletion, dehydration, and shortened red cell survival. Expression of PIEZO1 in lymphatics may explain pre/perinatal edema and ascites. EM developed sever prenatal ascites leading to abnormal abdominal musculature and impaired diaphragm movement and fetal breathing causing pulmonary hypoplasia with subsequent respiratory insufficiency at birth. The pathophysiology in this case is similar to that of prune belly, where abnormal abdominal musculature is known cause of impaired lung growth and development and subsequent respiratory compromise. Respiratory complications are primarily managed with supplemental oxygen and ventilatory support, if needed, until the lungs mature. Conclusion: This case highlights a previously unreported extremely rare disease, DHS, leasing to abnormal fetal breathing , marked pulmonary hypoplasia, and subsequent respiratory insufficiency.
-

Does Pediatric Palliative Care Involvement Influence Location of Death?
Joy Solano, Meghna Singh, Ashley K. Sherman, and Jennifer Linebarger
This study describes the influence of a palliative care team on location of death and location of death discussions with patients/caregivers, and determines whether location of death discussions influence location of death.
With palliative care or a location of death discussion, patients were less likely to die in the PICU and more likely to die at home. Location of death discussions were more likely to occur if a palliative care team was involved.
-

Fetal Ventricular Measurement in Determination for Intrauterine Closure of Myelomeningoceles
Paige Lundy, Emanuel Vlastos, and Paul A. Grabb
Prenatal closure of myelomeningoceles for fetuses with ventricular width of greater than 15 mm at the time of intrauterine screening (19-25 weeks) has been discouraged, but little is documented regarding the details of ventricle measurement, modality, and timing. This study concludes that ultrasound and MRI provide different results in regards to fetal ventricle size. If treatment recommendations are going to be offered or withheld based on the 15 mm "rule" the method of fetal imaging must be taken into account.
-
 Agonist Improves Hyperandrogenism in an Adolescent Female with a Novel Insulin Receptor Gene Mutation by Emily Paprocki, Romina Barral, Heidi Vanden Brink, Maria E. Lujan, and Tania S. Burgert")
Gonadotropin Releasing Hormone (GnRH) Agonist Improves Hyperandrogenism in an Adolescent Female with a Novel Insulin Receptor Gene Mutation
Emily Paprocki, Romina Barral, Heidi Vanden Brink, Maria E. Lujan, and Tania S. Burgert
We describe a case of an adolescent female with Type A insulin resistance whose severe hirsutism and hyperandrogenism were improved with leuprolide, despite extreme hyperinsulinemia. Ovarian volume decreased in association with the resolution of hyperandrogenism, consistent with ovarian size reflecting hyperandrogenism in adolescents.
This case allowed us to examine the frequently debated bidirectional relationship between insulin and hyperandrogenism, often deemed independent of gonadotropin activity.
-
 by Luke Prest, Lauren Fenstermann, and Ayman Khmour")
Improving NICU Referrals to the Missouri Early Intervention Program (First Steps)
Luke Prest, Lauren Fenstermann, and Ayman Khmour
First Steps is the statewide early intervention program in Missouri, but a review of referrals from the Truman neonatal intensive care unit revealed that only 24% of eligible patients were being referred. This poster describes efforts to increase awareness among residents and to refer all eligible patients to First Steps upon discharge.
-

Neuroblastoma in Adolescents and Children Older than 10 Years: Unusual Clinicopathologic and Biologic Features
Laura McCarthy, Katherine Chastain, Terrie Flatt, Eugenio Taboada, Robert E. Garola, John Herriges, Linda D. Cooley, and Atif Ahmed
This poster describes four cases of neuroblastoma diagnosed since 2008 in children greater than 10 years and presents their clinical, histologic and biologic features, emphasizing unusual clinicopathologic characteristics and the role of DNA microarray analysis and Next Generation Sequencing in their management.
-

Outcomes Following Dynamic Compression Bracing for Pectus Carinatum
Charlene Dekonenko, Robert M. Dorman, Amy L. Pierce, Beth A. Orrick, David Juang, Pablo Aguayo, Jason D. Fraser, Tolulope A. Oyetunji, Charles L. Snyder, Shawn D. St Peter, and G W. Holcomb III
We describe our experience with dynamic compression bracing for pectus carinatum patients and their satisfaction with bracing.
-

Pediatric PPI Use and Fractures
Nathan R. Fleishman, Troy Richardson, and Thomas M. Attard
This study compared the rate of fracture among pediatric patients exposed to proton pump inhibitors to the rate among patients without exposure, and also considered the fracture location among children exposed to proton pump inhibitors.
-

Predictive Performance of Existing Population Pharmacokinetic Models of Tacrolimus in Pediatric Kidney Transplant Recipients
Alenka Chapron and Susan M. Abdel-Rahman
With the goal of developing a clinician-driven tacrolimus (TAC) pharmacokinetic dosing tool, our initial objectives were 1) to examine whether published TAC population pharmacokinetic (popPK) models could serve as a foundation for the dosing tool, and 2) evaluate their performance predicting TAC concentrations in an independent cohort of Children's Mercy patients.
-

Prospective Evaluation of a Population Pharmacokinetic Model of Pantoprazole for Obese Children
Alenka Chapron, Susan M. Abdel-Rahman, and Valentina Shakhnovich
We previously developed a population pharmacokinetic (popPK) model of pantoprazole for obese children. Our objective was to evaluate the predictive performance of this model in an independent cohort of normal weight, overweight and obese children.
-

Quality Improvement: Implementing a Foot Exam to Improve Care for Patients with Diabetes Mellitus
Emily Paprocki, Ryan McDonough, Tiffany Musick, and Joseph Cernich
The American Diabetes Association guidelines recommend an annual foot exam in patients with type 1 and 2 diabetes who are ten years old or older and who have been diagnosed with diabetes at least five years. Quality improvement tools were used to improve the care provided to our patients by implementing an annual food exam.
-

Self-Reported Outcomes Following Cholecystectomy for Pediatric Hyperkinetic Biliary Dyskinesia
Charlene Dekonenko, Joseph A. Sujka, Robert Michael Dorman, Tolulope A. Oyetunji, and Shawn D. St Peter
The aim of this study is to determine if children with hyperkinetic biliary dyskinesia have resolution of symptoms after laparoscopic cholecystectomy at our institution.
Conclusion: Cholecystectomy for hyperkinetic biliary dyskinesia may or may not improve symptoms. Further research should focus on pathophysiology of the disease in order to create an evidence-based definition of biliary dyskinesia in children to determine who will benefit from cholecystectomy. -

The Effect of Antihypertensive Dosing on Hypertension in Children with Chronic Kidney Disease
Benjamin A. Matta, Uri S. Alon, Tarak Srivastava, Bradley A. Warady, and Darcy Weidemann
This study's objective was to determine the effect of antihypertensive dose on hypertension status in children with chronic kidney disease. This was the first quantitative analysis of antihypertensive dose expressed as a newly developed measure, cDDI, and is relationship with hypertension status in children with CKD.
-

Viral Whole Genome Sequencing for Antiviral Resistance in a Child with DOCK8 Deficiency and Recurrent HSV-1
Sean Stout, A. L. Greninger, Rangaraj Selvarangan, A. F. Freeman, Brandon D. Newell, Erin Stahl, and Dwight Yin
We present the case of a child with dedicator of cytokinesis 8 (DOCK8) deficiency and chronic, resistant HSV-1 mucocutaneous infections to illustrate the clinical utility of viral whole genome sequencing to detect active and latent HSV resistance mutations.
-

Who Codes in the NICU: An Analysis of Demographics and Factors that Place Neonates at Higher/Lower Risk of a Serious Code Event and Prognosis Post-Code
Danielle N. Gonzales, Ashley K. Sherman, Jennifer Dremann, Staci Elliott, Amelia Gute, Amber Bellinghausen, Jessica Brunkhorst, and Danielle Reed
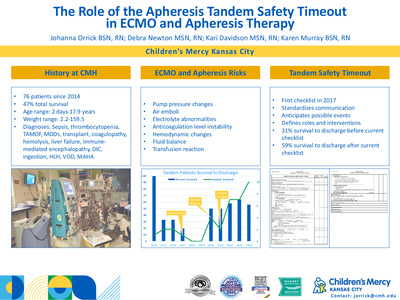
This study analyzed resuscitation events in a level IV neonatal intensive care unit from 2012-2017 to determine whether there are identifiable differences between those who have a rapid response event and those with a short or long code and determine factors post-event that may impact survival to discharge.
-

Improving Discharge Communication with Outpatient Providers on the Hospitalist Service
Nicholas Clark, Julia Simmons, Angela Etzenhouser, Troy Richardson, Patrick Brady, and Eugenia K. Pallotto
Describes a quality improvement project to increase two-way discharge communication between pediatric hospitalists and primary care providers from 7% to >80% within 18 months.
-

Practice Variations in Sedated Echocardiography and Impact on Repeat Echocardiography in Non-Refractory Kawasaki Disease
Nicholas Clark, Troy Richardson, Jennifer E. Schuster, Anitha Parthiban, and Henry T. Puls
This study discovered significant variation among children's hospitals in the use of sedated echocardiiography for children <30 months of age with non-refractory Kawasaki disease prior to the American Heart Association 2017 Kawasake disease guideline update. Consideration should be given to performing sedated echocardiography as it may reduce the need for repeat echos without impacting length of stay or total>costs.
-

The Effect of Antihypertensive Dosing on Hypertension in Children with Chronic Kidney Disease
Benjamin A. Matta, Uri S. Alon, Bradley Warady MD, Tarak Srivastava, and Darcy Weidemann
Background
Hypertension (HTN) is a highly prevalent and major risk factor for poor cardiovascular and renal outcomes in chronic kidney disease (CKD). Previous research suggests that HTN is underdiagnosed and undertreated in children with CKD. To our knowledge no studies have investigated the effect of antihypertensive (antiHTN) dose on blood pressure (BP) control in this population.
Objective
To determine the effect of antiHTN dose on HTN status in children with CKD.
Methods
Study population: 255 participants studied in the Chronic Kidney Disease in Children (CKiD) study at their 3rd visit, taking at least 1 antiHTN drug.
Cumulative Drug Dose Index (cDDI): We developed a new quantitative tool, Drug Dose Index (DDI) which is expressed as a ratio between the current dose and the maximum potential dose, accounting for age, weight and renal dose adjustments. cDDI = sum DDI for all antiHTN agents for a subject.
Primary outcome: HTN status - controlled HTN (cHTN) or uHTN (= masked HTN or ambulatory HTN).
Secondary outcome: Left ventricular hypertrophy.
Statistical analysis: Univariate analysis: Comparison of cDDI between the outcome groups. Multivariate Logistic Regression: 2 models with outcomes: uHTN and LVH.
Results/Discussion
This was the 1st quantitative analysis of antiHTN dose (cDDI), and its relationship with HTN status in children with CKD. No differences in cDDI between uHTN vs. cHTN, or LVH vs. no LVH, but higher cDDI was associated with AH on univariate analysis. RAASi and diuretic use were associated with lower odds of uHTN. Non-Caucasian race, absence of RAASi and diuretic agents, and higher number of agents were associated with uHTN. Female gender, higher BMI z-score, lower eGFR, higher number of agents and lower cDDI were associated with LVH. Further research is needed to validate the use of cDDI and the the roles of medication class and dose on BP control in children with CKD.
-

Improving bronchiolitis care across multiple care settings using a deimplementation bundle
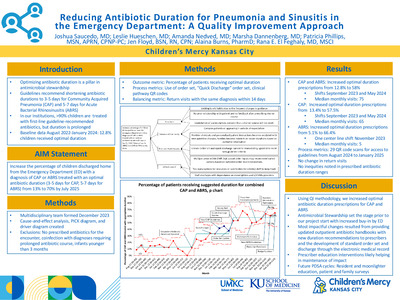
Amanda Nedved, Kathleen Berg, Troy Richardson, Amanda Montalbano, and Matthew B. Johnson
Despite the availability of a bronchiolitis CPG; variation in care practices still existed at our institution. The aim of our quality improvement (QI) project was to increase overall adherence with our institutional CPG in patients 60 days to 24 months of age diagnosed with bronchiolitis in the urgent care centers (UCC), emergency departments (ED), and general inpatient units from a baseline of 40.9% to 60% by the end of two bronchiolitis seasons.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}