
These posters have been presented at meetings in Children's Mercy and around the world. They represent research that was done at the time they were created, and may not represent medical knowledge or practice as it exists at the time viewers access these posters.
-

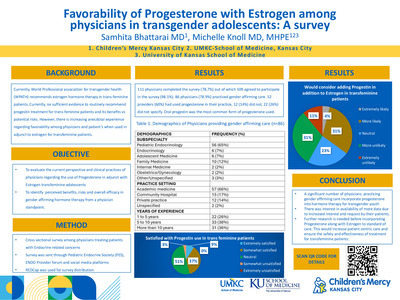
If We Know Better, Why Don’t We Do Better? A QI Project Aimed at Addressing Pain Related to Vaccinations
Haley J. Killian, Amanda D. Deacy, Elizabeth Edmundson, Lucy Raab, and Jennifer Verrill Schurman
Introduction: Evidenced-based tools have long existed to combat pain and anxiety associated with needle sticks, yet the gap between knowledge and uptake persists. Prior to COVID-19, our institution initiated a quality improvement (QI) program to improve comfort measure (CM) uptake, beginning with specific clinical areas with intent to scale up over time. When the COVID-19 vaccine was approved, mass vaccination clinics provided an opportunity to rapidly improve CM uptake across the institution. Methods: Mass vaccination clinics were staffed by nurses from across the hospital. Clinics occurred in 3 waves, based on federal approval for age groups (1: 12y+, 2: 5-11y, and 3: 6m-4y). Each wave was treated as its own PDSA cycle. Families completed a post-vaccination survey to determine what CMs were offered, how much CMs seemed to help their child, and plans for using similar CMs again. Across each wave, data on uptake were considered alongside qualitative feedback from families, nursing staff, and administrative leaders to determine targets for the next PDSA cycle. Selected interventions broadly considered the evidence base across ages, mass vaccination clinic flow, caregiver/patient understanding of available tools, and infrastructure available to support institutional change efforts. Results: Uptake of targeted CMs increased in response to PDSA waves, and generally remained stable thereafter. Across waves, families reported that CMs helped their child with pain/distress (Wave 1: 71%; 2: 88%; 3: 88%) and intended to use some or all the same CMs for future vaccinations (Wave 1: 84%; 2: 96%; 3: 97%); rates increased across both with younger patient age. Conclusions: In a fast-paced mass vaccination clinic, uptake was good to excellent across various CMs and age groups and yielded high satisfaction and interest in future use. Further, many nurses became change agents in their clinical area. Lessons learned will be discussed.
-

Objective and self-report outcomes of intensive interdisciplinary pain treatment for youth with chronic pain with and without functional neurological disorder
Kelsey Zaugg, Dustin Wallace, Kayla Friesen, and Cara M. Hoffart
Introduction: Intensive interdisciplinary pain treatment (IIPT) is effective for youth with chronic pain (CP). Many from this population also experience functional neurological disorder (FND). Treatment outcomes for patients with CP and FND during and after IIPT have not been thoroughly examined, and studies utilizing objective physical and occupational therapy measures are particularly lacking. Methods: 301 adolescents (M age=15.34 years, 84.4% girls, CP only: 187, CP and FND: 114) participated in individualized physical, occupational, psychological, and other therapies. Self-report (COPM, functioning) and objective (BOT-2, 6-minute-walk) measures were administered pre-IIPT, post-IIPT, 6-months-post, and one-year-post. Results: Overall, there were strong and statistically significant improvements from baseline to all other time points (all p’s<.01) for those with CP only and those with CP and FND. From pre-IIPT to post-IIPT, there were statistically significant group differences indicating less improvement for those with FND on coordination, strength, and agility tasks of the BOT-2 (F(1,255)=6.08, p=.014; F(1,255)=9.03, p=.003); on COPM satisfaction (F(1,258)=6.31, p=.013); and 6-minute walk test distance (F(1,217)=5.08, p=.025). Significant group differences from baseline to all follow-up timepoints indicated those with FND had less improvement on COPM performance (F(1, 258) =14.16, p <.001; F(1,150)=5.95, p=.016; F(1,96)=6.394, p=.013) and overall functional disability F(1,262)=15.43, p <.001; F(1,172)=4.250, p=.041; F(1,119)=5.44, p=.021). However, the BOT-2, 6-minute-walk and COPM satisfaction did not differ significantly at follow-ups, indicating no significant difference between those with and without FND. Conclusions: This study suggests that objective and self-report outcomes differ significantly between IIPT participants with CP and FND compared to those with only CP. However, both groups improved significantly overall, and some differences weakened in magnitude over time.
-

Prevalence of Iron Deficiency in Patients with Inherited Bleeding Disorders
Thomas Cochran, Brian Lee, and Shannon Carpenter
Background: Synthesis of hemoglobin is one of several important roles iron plays in the human body. Approximately 50% of all anemia cases may be caused by iron deficiency which is frequently caused by chronic blood loss. Patients with bleeding disorders have greater propensity for blood loss and therefore may have a higher prevalence of iron deficiency when compared to the general population. However, few studies have assessed the prevalence of iron deficiency in children with inherited bleeding disorders. Objectives: This study aims to identify the prevalence of iron deficiency in children with an inherited bleeding disorder. Methods: A retrospective analysis of children with any inherited bleeding disorder seen in Children’s Mercy Hospital’s hemophilia treatment center between 2010 and 2020 was performed. Iron deficiency was defined by recently published serum ferritin thresholds outlined by the National Health and Nutrition Examination Surveys (NHANES) [1]. Subjects were defined as iron deficient if they met these criteria at any visit. Other patient characteristics such as concomitant iron deficiency risk factors and use of iron supplementation were included in the analysis. Results: There were 507 patients with inherited bleeding disorders who were included in this analysis. Of the 177 patients who had serum ferritin collected, 103 (58%) were iron deficient. In patients who were iron deficient, 69% were female and 51% were aged 6 to 15 years. Notably, of the 68 (38%) males with serum ferritin collected, 31% were iron deficient. Of the 478 patients who had blood counts measured, 217 (45%) were anemic. Of the patients with anemia, 138 (64%) were male. The proportion of patients found to be iron deficient in each age group are displayed in figure 1. Only 4 (4%) of the patients found to be iron deficient had other iron deficiency risk factors. Furthermore, 64 (62%) of patients who were identified as iron deficient were on some form of iron supplementation. Conclusion: The results of this study suggest that iron deficiency is more prevalent in patients with inherited bleeding disorders when compared to the general population. Prior epidemiologic analysis of iron deficiency and iron deficiency anemia is mostly focused on adolescent females, but these results suggest that males with inherited bleeding disorders are at comparable risk. The actual prevalence of iron deficiency in male patients may be higher than this report suggests considering ferritin levels were not measured in 75% of males. Furthermore, the prevalence of iron deficiency is likely underreported in studies prior to the recently published NHANES physiologic ferritin thresholds. These patients represent half of the population identified for inclusion in this retrospective study.
-

Psychosocial Needs of Pediatric Patients with Cancer Predisposition Syndromes: Standardized Screening Needed
Meredith Ehrhardt, Mirae Fornander, and Rachel Moore
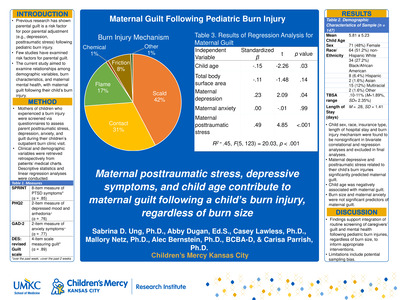
Introduction Cancer predisposition syndromes (CPS; e.g., Li-Fraumeni syndrome, Von Hippel-Lindau syndrome) require routine, standardized medical monitoring with accompanying unique, complex psychosocial needs (e.g., family medical needs). Despite limited research within pediatric populations, emerging literature has begun to support the benefit of routine psychosocial screening in this population. Very few pediatric CPS clinics with dedicated psychosocial care (i.e., psychology) exist in the U.S. and there is currently no standard of care for psychosocial support of CPS patients. This study aims to better understand the psychosocial needs of pediatric CPS patients and support the need for a standardized psychosocial screening protocol among pediatric CPS clinics. Methods Data collection in the Surveillance for Predispositions to Tumors (SPoT) Clinic was obtained from 2021-2022 via REDCap using standardized psychosocial screening battery for all patients and their parents which included demographic, academic, developmental, general health, quality of life, resilience, and genetic diagnosis reaction measures and suicidality, mood, and anxiety screeners. Results A total of 25 patients between 2 and 19 years old (M=11.80, SD=4.70) completed the standardized screening. Patients were predominately assigned female at birth (N=15, 60%) and non-Hispanic White (N=19, 76%). Most denied academic concerns (N=17, 68%). A subset of patients reported concerns for depression (N=5, 20%, M=5.64, SD=5.45; mild n=3, moderate n=2, severe n=1) or anxiety (N=4, 16%, M=5.50, SD=5.77; mild n=3, moderate n=1, severe n=1). Few patients reported a current or past therapy history (N=7, 28%). Patients reported medium to high levels of hope for their future (N=8, M=4.40, SD=1.23). Conclusions Preliminary, descriptive results suggest that CPS patients have medium to high levels of hope and few concerns for depression and anxiety compared to adult CPS patients. Importantly, this study describes a standardized psychosocial screening protocol model for CPS clinics as a first step toward identifying a standard of care for psychosocial screening.
-

Experiences of Racism among Black and African Children with Asthma
Esosa Adah, Rayanna Tucker, and Bridgette Jones
Rationale: The relationship between adverse childhood experiences, toxic stress and asthma risk has been previously described in the literature among adult and pediatric populations. Studies have identified experiences of racism as a chronic stressor associated with asthma morbidity however, most studies have focused primarily on adults or parental perspectives. We initiated a pilot study to characterize described experiences of racism among Black/African American children with persistent asthma and describe some of our initial results. Methods: Children were asked to complete the “Perceptions of Racism in Children and Youth,” a validated questionnaire, measuring perceptions of racism and discrimination. Responses were analyzed for frequency of shared responses. Results: Ten children ages 7-17 years completed the survey. 100% of participants(n=10) endorsed experiencing at least one racist or discriminatory event ranging in frequency from once to weekly. Overall, 60% of children endorsed “being called an insulting name”; 20% endorsed “being watched closely or followed around by security guard at a store/mall”; 20% endorsed “having the feeling someone was afraid of them”; 30% endorsed “someone making an insulting remark about one’s race ethnicity, or language”;10% endorsed “seeing one’s family being treated unfairly due to race, skin color, accent or culture differences.” Conclusions: Initial data from this ongoing pilot study demonstrates that children with asthma endorse a broad range of experiences of racism. Intentional efforts are needed to raise awareness of racism as a chronic, toxic stressor experienced by children with asthma and efforts should be made to mitigate the impact on asthma morbidity.
-

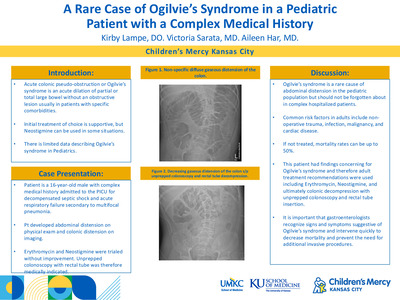
Late Onset Paradoxical Effect of Zolpidem after Anoxic Brain Injury: A Pediatric Case Report
Amanda Lindenberg and Sathya Vadivelu
Case Diagnosis Acquired brain injury (ABI) is a common cause of disability. It is defined as an insult to the brain that subsequently results in impairments of communication, cognition, sensorimotor function and behavior. Anoxic brain injuries can be particularly disabling. A common cause of a anoxic injury in children is cardiopulmonary arrest. The revised coma recovery scale (CRS-R) is a standardized assessment for level of arousal after brain injury. Case Description A 16 year old healthy boy was admitted after an unwitnessed pulseless cardiopulmonary arrest requiring 3 defibrillations and 2mg of epinephrine. His cardiac and genetic workup was negative. His brain imaging revealed diffuse ischemic injury to the temporal, parietal and occipital regions and the basal ganglia. His hospital course was complicated by dysautonomia requiring clonidine, propranolol, and lorazepam, hypertonicity and agitation requiring gabapentin and baclofen, botox injections, and serial casting, impaired sleep/wake cycles requiring melatonin and zolpidem, and decreased level of arousal. He was admitted to inpatient rehab from February 26 to April 5, 2016. He was trialed on multiple neuro-stimulants including zolpidem but did not emerge from a persistent vegetative state. Shortly after discharge, his parents reported a change in his level of alertness and command following after administration of zolpidem. During a follow up appointment, a trial of zolpidem confirmed improved CRS- R score from 6 to 14. Discussions Zolpidem is medication that stimulates the ω-1 site of a gamma aminobutyric acid (GABA)A receptor in the brain. The basal ganglia and striatum to the thalamus and motor cortices are abundant in these receptors. Moreover, it is hypothesized that the paradoxical effect of zolpidem in neurologic disorders is secondary to the agonism. There is a paucity of reports in children. Conclusions Zolpidem may have a paradoxical effect in the pediatric brain injury population after a prolonged period of medication.
-

Successful VA ECMO for a pre-B cell acute lymphoblastic leukemia patient with necrotizing faciitis from Clostridium septicum
Johanna I. Orrick, Brittany Rouchou, Cara Holton, and Jenna Miller
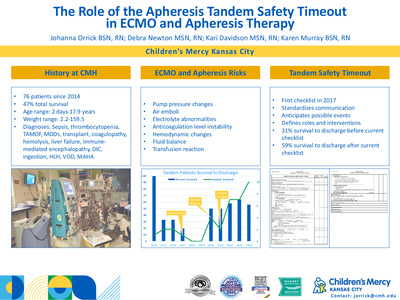
REPORT: It can be challenging to calculate the risks versus benefits of a potential Extracorporeal Membrane Oxygenation (ECMO) pediatric candidate. A patient with an oncologic comorbidity and an increased potential of needing near-future surgical interventions carries higher ECMO risks. We report a successful VA ECMO run of a newly diagnosed acute lymphoblastic leukemia (ALL) adolescent with Clostridium septicum necrotizing fasciitis. A previously healthy 16-year-old male was diagnosed with pre-B cell ALL after having an ileocolic intussusception and a Clostridium septicum blood infection. He underwent successful surgical intussusception reduction, started induction chemotherapy, and completed a ten-day course of antibiotics. On hospital day (HD) 15, he experienced significant abdominal pain and profound septic shock. His abdominal CT scan was concerning for air and fat stranding within the anterior abdominal wall. He was taken to the OR, where he was found to have necrotizing fasciitis and underwent debridement and silo placement. He returned to the Pediatric Intensive Care Unit on multiple high-dose vasoactive infusions with hemodynamic instability refractory to aggressive volume resuscitation. His instability and lactic acidosis progressed quickly in the 60 minutes after arriving from the OR, and thus, careful consideration was given to his ECMO candidacy. The prognosis for survival from ALL is 60-90% in adolescents (1,2). Repeat blood cultures had not speciated at the time of our patient’s hemodynamic decline, but necrotizing fasciitis survival in pediatrics ranges from 60-90% (3-6). Early surgical intervention increases the survival rate of myonecrosis, but future interventions would be complicated by anticoagulation on ECMO (7-9). Little more than a few case studies have been reported on the outcomes of ECMO patients with active necrotizing fasciitis (10,11). Compared to other pediatric ECMO patients, immunocompromised and oncological patients on ECMO have historically higher mortality rates. However, current survival reports have been improving (12-15). Ultimately, he was determined to be an ECMO candidate. While the team mobilized, he suffered a 16-minute bradycardic arrest but was successfully cannulated to VA-ECMO. Bivalirudin was used in anticipation of surgical procedures considering its short half-life. Chemotherapy was held, and antimicrobials were broadened. Repeat surgical debridement happened on ECMO day 2. Heparin neutralized partial thromboplastin time (PTT) measured at 69 seconds, so no anticoagulation adjustments were made for the procedure. He received alternating 1.1x plasma exchanges and granulocyte infusions during the first week of ECMO. A large volume GI bleed complicated his ECMO run, but he was able to be successfully decannulated on ECMO day 8. He was discharged home on HD 54 neurologically intact and is currently in the Interim Maintenance I stage of his pre-B ALL treatment. He has been home for six months at the time of this report. (Discharged 5/11/2022) While more centers are reporting their individual ECMO experiences in high-risk oncologic pediatric populations, the data is lacking for pediatric ECMO cases with multiple comorbidities and surgical intervention needs while on ECMO. Our approach required surgical collaboration and would be necessary for any future patients such as this. ECMO candidacy should not be ruled out for these patients, and case-by-case candidacy determinations should be undertaken. Understanding outcomes of the underlying disease and acute processes could improve with increased data collection and sharing.
-

Philippines Global Health
Thomas Rieth, Kourtney Bettinger, and Ryan Northup
Provides reflections on resident's experience working with cardiologists and neonatologists in Manila.
-

San Pedro Hospital - San Pedro La Laguna, Guatemala
Jennifer Paumen
Primary objective: to learn about the healthcare system of Guatemala including the challenges and strengths.
-

Eosinophilic Myocarditis Secondary to Hypereosinophilic Syndrome vs. Eosinophilic Granulomatosis with Polyangiitis: A Diagnostic Dilemma
Nathan LaVoy, Brian Birnbaum, Julia G. Harris, Aarti Pandya, and Allison Taber
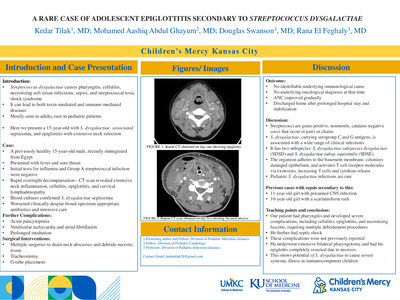
Introduction: Hypereosinophilic syndrome (HES) is a rare but detrimental diagnosis in the pediatric population. Cardiac involvement within HES can present as a diagnosis of Eosinophilic Myocarditis which can progress to irreversible damage and potentially death. This case report discusses a 16-year-old male treated for HES, although HES can have overlap with Eosinophilic Granulomatosis with Polyangiitis (EGPA) and requires a multi-disciplinary approach to patient management. Case Description: The patient was a 16-year-old male, with a history of asthma, presenting with acute onset of chest pain. He was found to have peripheral eosinophilia with an absolute eosinophil count of 11.71. He had ST segment elevations on electrocardiogram, persistently elevated troponin levels (peak of 14.8ng/mL), and increasing arrhythmia burden which consisted of multifocal premature ventricular contractions and rate dependent bundle branch block. A cardiac MRI was notable for an edematous left ventricle with moderate to severe dysfunction, moderate right ventricular dysfunction, and moderate pericardial effusion. Endomyocardial biopsy was not performed given the tenuous clinical status of the patient and he was admitted to the pediatric cardiac intensive care unit. A diagnosis of Eosinophilic Myocarditis was made based on clinical, laboratory, and imaging changes for which high dose steroids were administered. There was a dramatic decrease in peripheral eosinophilia (0.21) as well as near resolution of arrhythmia burden within twenty-four hours of steroid initiation. He successfully discharged from the hospital but continued to have eosinophilia in the outpatient setting. Given the working diagnosis of HES and possibility of EGPA, therapy with mepolizumab, an IL-5 inhibitor to prevent activation and proliferation of eosinophils and B cells, was initiated and is a treatment for both HES and EGPA. Unfortunately, he has now developed chronic left ventricular systolic dysfunction and dilation which is being managed with sacubitril/valsartan, metoprolol, and eplerenone with which he remains asymptomatic. Discussion: The etiology of the eosinophilia was most likely secondary to HES although there remains overlap with EGPA and is difficult to exclude. EGPA is rare in the pediatric population and is largely a tissue diagnosis. Given that the patient had presented on daily steroids, a tissue diagnosis would have likely been inconclusive, however, the diagnosis of EGPA is considered given the patient’s longstanding history of asthma, history of nasal polyposis with sinusitis, and sudden presentation of myocarditis with eosinophilia. Without definitive tissue biopsy and a negative ANCA, this diagnosis is largely based off presumption and will require monitoring his response to treatment. HES can present with myocarditis and is still the likely etiology, however, the patient had a normal bone marrow biopsy and did not have any gene mutations known to have an association with the disease (JAK2, V617F, and c-kit D816V). Although initial treatment may be similar, the management for refractory HES and EGPA differs and will require ongoing multi-disciplinary follow up.
-

A Rare Cause of Urticaria In An NSAID Tolerant Patient
Thao Le, Mary K. McLeod, and Laurianne Wild
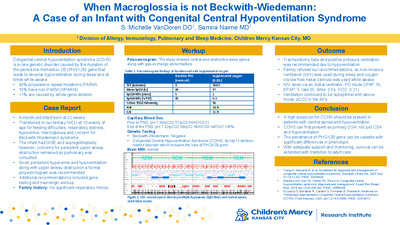
Introduction: Acetaminophen is one of the most used anti-pyretics to mitigate fever. Few cases have been reported of hypersensitivity reactions to acetaminophen without non-steroidal anti-inflammatory drug (NSAID) intolerance. It is recommended that if there is suspected drug hypersensitivity then the patient should undergo an oral drug challenge. Case Description: A 49-year-old male presented for evaluation of urticaria that occurred with acetaminophen ingestion. He reported several episodes where he developed diffuse urticaria within 15 minutes of ingestion, but no other symptoms concerning for anaphylaxis. He was unsure of the dose. He also noted urticaria with Excedrin migraine, which contains acetaminophen, aspirin, and caffeine. He tolerated NSAIDs alone. An oral drug challenge was performed. He was administered 250mg of acetaminophen, which he tolerated. After taking his second dose of 250mg, he developed pruritus and 4 urticarial lesions within 30 minutes. He did not have any other signs of anaphylaxis. He was treated with 20mg of loratadine. Upon re-evaluation, he had more diffuse urticarial lesions, but no other symptoms and he remained hemodynamically stable. He was serially monitored every 15 minutes for a total of 90 minutes, with near-resolution of his urticaria. Discussion: Pseudoallergy is an immediate systemic reaction that resembles anaphylaxis, but is non IgE-mediated. NSAIDs are a common cause of pseudoallergy. There are cases of acetaminophen hypersensitivity reactions in NSAID intolerant patients due to cross-reactivity. If a patient is NSAID tolerant and develops symptoms with acetaminophen, it is more likely to be IgE-mediated. Acetaminophen challenge should be done with caution and avoided if positive.
-

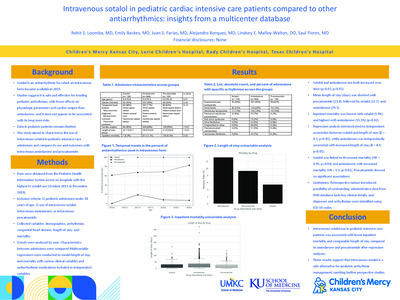
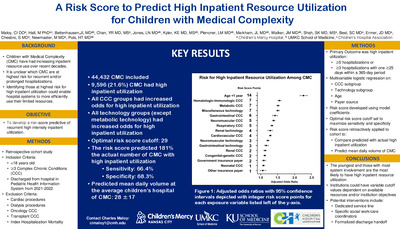
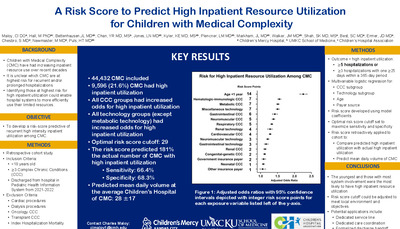
Cardiac Biomarkers in Differentiating Kawasaki Disease and Multisystem Inflammatory Syndrome in Children Associated with COVID-19
Mollie Walton, Geetha Raghuveer, K Kamakoti, N Dahdah, L Garrido, S Tierney, T Harris, M Khoury, M Hicar, E Braunlin, D Thacker, M Khare, F Dallaire, R Lowndes, I Glassmeyer, J Ballweg, G Goldenberg, S Merves, C Manlhiot, P Farid, and BW McCrindle
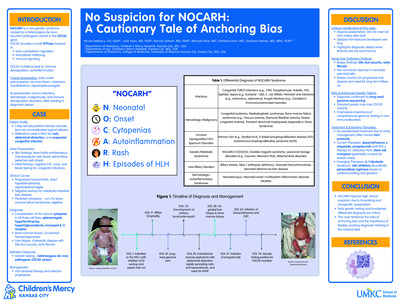
Introduction – Kawasaki disease (KD) and Multisystem Inflammatory Syndrome in Children (MIS-C) associated with COVID-19 show considerable clinical overlap making differentiation challenging, particularly in the absence of evidence of evidence of prior COVID-19. Hypothesis – Cardiac biomarkers can differentiate KD from MIS-C. Methods – The International KD Registry enrolled n=2903 contemporaneous KD, MIS-C and acute COVID-19 pediatric patients from 42 sites in 8 countries from January 2020 through July 2022. The study population was confined to 1489 MIS-C patients meeting CDC criteria with confirmed evidence of prior COVID-19 infection and 387 KD patients meeting AHA guideline criteria with confirmed evidence supporting no prior COVID-19 infection, limited to those with sufficient echocardiogram data and at least one measurement of NTproBNP or Troponin I (118 KD, 946 MIS-C). A normalizing logarithmic transformation was applied to biomarker levels and multiple imputation of missing values of factors was performed before multivariable regression analyses to determine associated factors. Regression models were adjusted for diagnosis, age and creatinine at presentation and then explored for associations of biomarkers with clinical presentation, laboratory variables and cardiac involvement. Receiver operating characteristic curves were used to determine biomarker cut points differentiating KD from MIS-C. Results – Of 118 patients with KD, 90 had NTproBNP (median 370 ng/L) and 91 had Troponin I (median < 10 ug/L) assessed at presentation, while of 946 patients with MIS-C, 580 had NTproBNP (median 1944 ng/L; p<0.001 vs KD) and 763 had Troponin I (median 35.0 ug/L; p < 0.001) assessed. Baseline NTproBNP and Troponin I were not significantly correlated (r=0.08; p=0.10). Higher Troponin I was correlated with older age (r=0.07; p=0.04) and higher creatinine (r=0.25; p < 0.001), whereas NTproBNP was only correlated with higher creatinine (r=0.29; p < 0.001). After adjusting for diagnosis, age and creatinine, both higher log(NTproBNP) and log(Troponin I) were association with shock at presentation (p <0.001, p < 0.001, respectively) and ICU admission (p=0.003, p < 0.001). Higher log(NTproBNP) but not log(Troponin I) was associated with longer length of hospital stay (p < 0.001, p=0.23). After similar adjustments, laboratory variables at presentation independently associated with cardiac biomarkers are shown in TABLE. LV ejection fraction (LVEF) was lower for MIS-C versus KD (median 56% vs 63%; p<0.001). After adjusting for diagnosis, age and creatinine, higher baseline log(NTproBNP) was associated with lower LVEF (p<0.001) and LVEF<55% (p<0.001). After similar adjustments, higher baseline log(Troponin I) was association with lower LVEF (p=0.03) and LVEF<55% (p=0.03). Maximum coronary artery Z score was greater for KD versus MIS-C (median 1.36 vs 1.23; p<0.05). After adjusting for age, creatinine and diagnosis, higher baseline log(NTproBNP) was not associated with maximum coronary artery Z score (p=0.36) but with max Z score>2 (p=0.02). After similar adjustments, baseline log(Troponin I) was not associated higher maximum coronary artery Z score (p=0.23) or max Z score > 2 (p=0.72). Baseline Troponin I > 10 ug/L (c-statistic 0.65) predicted MIS-C vs KD with a sensitivity of 58% and specificity of 77%, with > 20 ug/L 44% and 89%, respectively. Baseline NTproBNP > 500 ng/L (c-statistic 0.71) with a sensitivity of 74% and specificity of 54%, >1000 ng/L 61% and 72%, and >1 500 ng/L 56% and 77% (FIGURE). The c-statistic improved to 0.74 with both biomarkers together, and to 0.78 with both biomarkers at peak. Conclusions – Higher baseline Troponin I and NTproBNP levels are predictive of MIS-C versus KD with reasonable sensitivity and specificity, and are associated with an increased likelihood of shock and ICU admission. Lower LVEF, more common with MIS-C, is associated with higher NTproBNP and Troponin I levels, while coronary artery involvement, more comm
-

Case Report: Autoimmune anemia and thrombocytopenia following hematopoietic stem cell transplant
Thomas Cochran, Gabor Oroszi, Nancy Terwilliger, Gabe Metzler, and Lejla Music Aplenc
Background: Autoimmune cytopenias (AIC) post hematopoietic stem cell transplant (HSCT) are rare but exceptionally challenging complications. Here, we report anti E, warm autoimmune hemolytic anemia (WAIHA), cold autoantibody, polyagglutination and immune thrombocytopenia in a 5-year-old boy with a history of chronic granulomatous disease, who underwent an ABO incompatible, mismatched (9/10) unrelated HSCT. Study design: Case report. Four months after HSCT, the patient was admitted for fever, fatigue, and decreased appetite. His original blood type was O+ and donor’s blood type B+. Prior to the admission he was transfused with 2 doses of red cells and 2 doses of platelets. On admission, hematopoietic chimera evaluation demonstrated 100% donor-derived cells. Initial laboratory work-up revealed white blood count 10.07x103/uL, hemoglobin 4.2 gm/dL, platelets 137,000 x103/uL, absolute retic count 0.123 x 10(6)/mcL, total bilirubin 1.8 mg/dl (mainly indirect) and lactate dehydrogenase 1,037 unit/L. Results: Patient’s red cells and saline suspended red cells spontaneously agglutinated in all blood bank tests precluding valid ABO/Rh type and direct antiglobulin test (DAT). An eluate, prepared from the patient’s red cells washed with saline, was reactive at 22C and following 37C incubation. Antibody testing on the patient’s plasma showed the presence of anti-E antibody. Titration and thermal amplitude studies demonstrated titer <2 and no reactivity at 30C and>37C, respectively. Donath Landsteiner test was negative. DTT treatment of the eluate showed significantly weakened reactivity at 22C and weak reactivity at PEG IAT. His red blood cells demonstrated strong reaction with AB (9/10) and B plasma (4/4). Lectin studies showed red cells reacting strongly with Arachis hypogea but were non-reactive with Glycine soja, Salvia sclarea, Salvia horminum. Several months later, the patient developed thrombocytopenia with platelet count of 45,000x103/uL. HLA antibody testing was negative, but SPRCA and ELISA tests were positive revealing antibodies against GPIIb/IIIa platelet antigens. Conclusion: This is a report of a 5-year-old male post-HSCT who developed overt hemolytic anemia with laboratory testing that demonstrated evidence of WAIHA, anti-E antibody, clinically insignificant cold autoantibody and polyagglutination (T activation/polyagglutination ruled out). Several months later, hemolysis subsided but immune mediated thrombocytopenia ensued. This case demonstrates the complexity of AIC that rarely develop in patients who underwent HSCT.
-

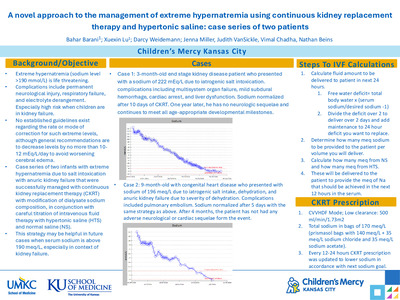
Improving fluid management of extreme premature infants by providing a restrictive fluid management algorithm in the ICN
Jacob S. Ward, Dena Hubbard, and Nicholas Clark
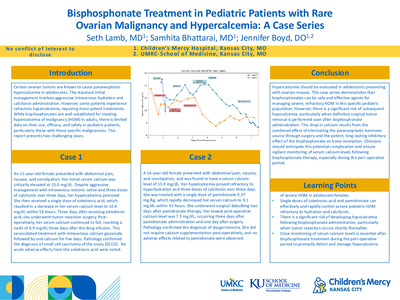
Intro: Excessive fluid intake in extremely premature infants during the first week of life is known to increase risk of adverse events such as necrotizing enterocolitis (NEC), patent ductus arteriosus (PDA), and overall mortality. There also is some correlation with the need for mechanical ventilation and development bronchopulmonary dysplasia (BPD). While fluid restriction is recommended to decrease the likelihood of adverse outcomes, at our institution we found there was a wide variability in and lack of evidence-based standards on fluid management in this vulnerable population. We aimed to improve the fluid management of the extremely premature infants by standardizing a restrictive fluid algorithm. Methods: Children’s Mercy Hospital admitted a total of 107 premature infants <28 6>/7 weeks gestation to the ICN during 2021, and 25 of these infants were admitted during the timeframe of our study. The restrictive fluid management algorithm (Fig. 1) was initiated in April of 2021. During a 6-month period we monitored clinician compliance as outcome measures and patient clinical indicators of fluid status as balancing measures (percentage of birth weight lost, time to diuresis, and time back to birth weight). Results: Of 25 patients started on the algorithm, 3 patients were excluded due to admission after 12 hours of life or death on day of life 1 and 14 patients followed algorithm on all 3 days. The infrequent number of admissions during this period lead to presenting data in g-chart format. The process measure of clinician compliance with total fluid volume algorithm showed mild improvement over time after the education, initiation, and availability of the algorithm began in our ICN with overall mean of 1.89 patients outside protocol of total fluids between those patients on protocol (Fig. 2). This was again reflected in additional outcome measure of compliance with total fluid volume algorithm plus an additional 20ml/kg/day of fluid with overall mean was 0.63 patients outside protocol between patients on protocol (Fig. 3) showing a modest sustainability. The results of following the restrictive fluid algorithm did not result in excessive weight loss, absence of diuresis, or prolonged time back to birth weight based on the balancing measures tracked during this time period (Fig. 4-6). Conclusion: The fluid algorithm for premature infants did allow for a modest improvement in standardizing fluid management as compliance with a more restrictive plan improved without resulting in concerning short term consequences, such as excessive weight loss. The next step would be to provide continued education regarding the fluid algorithm to help sustain improvement. We are currently in process of obtaining baseline data prior to onset of current algorithm to further compare past and present fluid management to better help determine if changes have improved patient outcomes thus leading to a new standard in our ICN. In the future, we would like to follow up the current patients to determine if the fluid algorithm was helpful in avoiding adverse outcomes such as BPD, NEC, or PDA.
-

Malignancy masquerading as steroid resistant hypereosinophilic syndrome
Sonya Parashar and Aarti Pandya
Introduction: Hypereosinophilia syndrome (HES) is defined as 1500 eosinophils/mL or above with evidence of end-organ damage due to the eosinophils at least 4 weeks apart. Case description: A 3-year-old male was admitted for newly found anterior mediastinal mass and left pleural effusion. About 6 weeks prior to admission, he was seen in his primary care office for difficulty breathing. Despite the appropriate treatment for his symptoms, the patient continued to have significant respiratory symptoms and a chest x-ray showed a large left pleural effusion. He was immediately transferred to a tertiary care center and a CT chest showed large left pleural effusion, possible abscess, small pericardial effusion, and concern for an anterior mediastinal mass due to mediastinal shift. He underwent a thoracentesis, which showed eosinophilia within the pleural fluid. While his peripheral eosinophils had fluctuated at the beginning of his hospitalization, the patient’s absolute eosinophil count suddenly increased from 600 to 25,048 and remained elevated above 20,000. He developed recurrent eosinophilic pericardial effusions requiring multiple pericardiocentesis. Despite high dose steroids and inpatient use of mepolizumab, his hypereosinophilia persisted. After two inconclusive fine-needle aspirations of his mediastinal mass, the patient’s family agreed to a thoracotomy with removal of the mediastinal mass. Pathology eventually revealed myeloid sarcoma, a variant of acute myeloid leukemia. Discussion: Steroid resistant HES should raise concern for underlying malignancy especially when eosinophils are above 20,000. Educational objective: After reviewing this case, participants should be able to include myeloid malignancy in their differentials when evaluating a patient with hypereosinophilia.
-

Mobile Health Software Platform Implementation to Improve Pediatric Remote Patient Monitoring Outcomes
Lori A. Erickson, Amy Ricketts, Jenny Marshall, Krista Nelson, Peter Churchill, Dawn Wolff, and Robert W. Steele
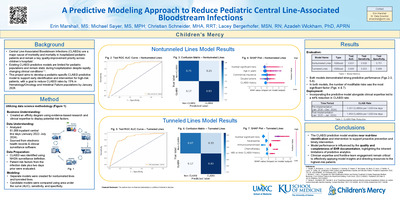
Background: Children’s High Acuity Monitoring Program (CHAMP®) is a software platform for pediatric remote patient monitoring. It is used with a proactive, personalized, pediatric care model providing a link for communication with a specialized healthcare team to patients and families in their homes. Successful implementation since 2014 includes: adoption at 12 pediatric hospitals and over 870 infants with a survival of 96.5% (down from 20% in 2012). This work led our team to engage leadership to discuss a remote patient monitoring department with new monitoring devices and expanded access to pediatric conditions.
Methods: Strategic Planning and Innovation facilitated navigation of an enterprise-wide endeavor over an 18-month period. Closed loop feedback with the administrative, clinical, information systems, and research teams ended with a well-rounded proposal for an innovative strategic initiative.
Results: Remote Health Solutions department was founded in September 2021 with a focus on integration of digital health and mobile applications, hardware, software platforms and wearable sensors to improve the healthcare team’s ability to provide personalized, proactive patient care. The team has three active feasibility studies for pediatric monitoring devices, four analyses from the Cardiac CHAMP registry, performs consults on remote monitoring facilitation with care teams, and is expanding CHAMP application use into additional clinical pediatric areas.
Conclusions: The forward movement of pediatric remote health stands at a precipice of opportunity within the landscape of mobile devices and applications in advancing pediatric medicine and outcomes. This project magnifies opportunities for evidence-based innovative pediatric care models, especially in the midst of the pandemic.
-

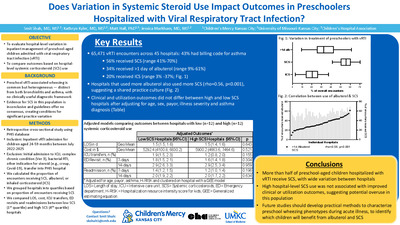
Alterations in the Metabolic Comorbidities of Youth with Overweight and Obesity during the COVID-19 Pandemic
Safa Farrukh, Erica Wee, Ashley Sherman, and Yun Yan
Background: Childhood obesity rates have continued to increase with the COVID-19 pandemic. However, data are limited on the impact of increasing obesity on associated comorbidities. Methods: We evaluated the progression of overweight- or obesity-associated comorbidities by investigating change in laboratory results pre–COVID-19 pandemic and post–COVID-19 pandemic onset in youth with overweight or obesity. Results: There was no significant BMI progression. There was progression of metabolic comorbidities. HbA1c progression and LDL progression were significantly correlated. HbA1c and LDL progression were significantly associated with older age and Hispanics respectively. Conclusion: The results indicate that despite no significant increase in BMI, youths with overweight or obesity have experienced progression of comorbidities during the COVID-19 pandemic. This study emphasizes the importance of early detection of comorbidities among a high-risk pediatric population.
-

Endoscopic Removal of Safety Pin from Appendiceal Orifice
Alex Biller, Moises Alatorre-Jimenez, Jeremy Stewart, and Ruba A. Abdelhadi
Introduction: Foreign body ingestion in children is considered a common concern in every Emergency Department worldwide. In the United States, it is estimated that foreign body ingestions cause approximately 1,500 deaths yearly (1). Safety pins ingestions are estimated to be 1% of the foreign body ingestions in children (2). In literature, ingested safety pins have been reported to be lodged mostly in the upper gastrointestinal tract, but a few cases have been reported to be lodged in the appendix (2,3,4). Objective: Recommendations for safety pin ingestions when past the second portion of the duodenum. Case: We report the case of a 5-year-old previously healthy female who presented with an accidental ingestion of an open safety pin. Following ingestion, the patient visited a local Emergency Room where an abdominal X-ray revealed an open safety pin located in the stomach. The patient was asymptomatic and had vital signs within normal limits for age with a normal exam. The patient was then transferred to a Children’s Hospital for further management and care; after traveling three hours, a follow-up X-ray on arrival to our Children’s Hospital revealed the safety pin to be located in the left upper quadrant (fig.1). As the patient continue to be asymptomatic, it was decided to continue monitoring progression with serial abdominal X-rays and initiate a bowel cleanout with GoLytely. Serial abdominal X-rays initially showed progression of the safety pin through the digestive tract and the patient remained asymptomatic. On the third day of admission, a repeat abdominal X-ray did not show progression of the safety pin and it appeared to be lodged in the right lower quadrant. At that time it was decided that the patient should undergo a colonoscopy with foreign body removal. During the procedure, the open safety pin was found in the appendiceal orifice with the head inside the Bauhin’s valve (fig.2). Careful extraction with rat-tooth forceps was performed; a pediatric surgeon was at the bedside for emergency abdominal decompression in case of appendiceal perforation. The open safety pin was successfully removed endoscopically without further damage to the patient’s colon. Conclusion: As per the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN), sharp foreign bodies should be removed immediately when located in the stomach or intestines if the patient is symptomatic (5). In asymptomatic patients with sharp foreign bodies in the stomach or small intestine, it is recommended that these be removed endoscopically within 24 hours if possible (5). Surgical intervention should be considered if there is no spontaneous clearance of the sharp object after 3 days (5). It has been reported in the literature by Gün et al., that ingested safety pins passing through the duodenum can be excreted spontaneously (6). In our case, the ingested open safety pin failed to advance on serial abdominal X-rays and appeared to be lodged in the right lower quadrant, and the safety pin was then found to be in the appendiceal orifice during colonoscopy. A metallic foreign body lodging in the appendix is a rare finding. Benizri et al. reported a case of a 29-year-old with abdominal pain who was found to have a metallic foreign body in the RLQ; serial x-ray one month later showed unchanged position (4). In this case they were unable to retrieve the foreign body by endoscopy due to inability to enter Bauhin’s valve to extract the object (4). Compared to our case, early serial x-rays and measuring progression to determine timing of extraction could prevent possible perforation or inflammation of the appendix and may lead to improved ability to remove the object endoscopically.
-

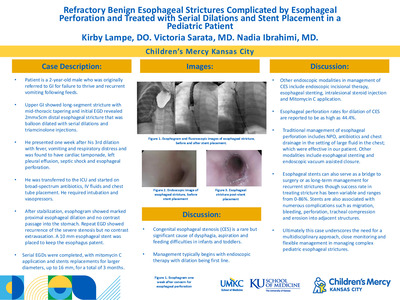
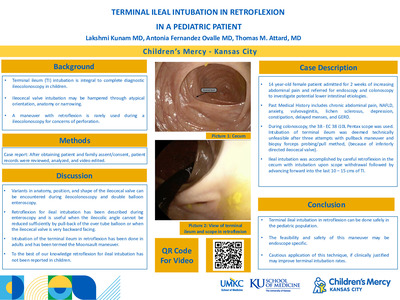
Endoscopic Retrograde Cholangiography Using A Colonoscope In A Pediatric Liver Transplant Patient With Roux-en-y Biliary Anastomosis
Nadia Ibrahimi, Thomas M. Attard, Ryan T. Fischer, Voytek Slowik, Richard J. Hendrickson, Bhargava Mullapudi, Moises Alatorre-Jimenez, and Syed Jafri
Introduction: Biliary ducal sequelae including occlusions, strictures, leaks, or necrosis frequently complicate pediatric liver transplantation. The underlying etiology includes prolonged intraoperative ischemia or postoperative arterial inflow obstruction. In adult patients the role of endoscopic retrograde cholangiography (ERC) is well established in the management of biliary complications post-liver transplantation. In contrast, in the pediatric population, due to the combination of small patient size and the complexity of Roux-en-Y anastomotic techniques, ERC has been described as difficult or virtually impossible. This limits the options available for managing biliary duct complications to percutaneous techniques Endoscopic management of biliary complications in pediatric patients with Roux-en-Y anatomy has not been previously reported in the pediatric population. Case: We present the case of an 8-yr-old patient with history of unresectable hepatoblastoma who underwent liver transplantation with Roux-en-Y anastomosis at the age of 15 months. His transplant was initially complicated by hepatic artery spasm and developing biliary strictures requiring biliary internal/external drain placement by interventional radiology (IR) twice in the first year following transplantation. He then presented at the age of 7 with recurrence of his biliary stricture at the site of choledocho-jejunal anastomosis and initial attempt for placing an internal/external biliary drain by IR was unsuccessful having not been able to pass a guidewire through the stricture. Another attempt 2 months later was successful, and an 8.5 French drain was placed then upsized to a 12 French 2 months later and removed after a total of 4 months. His biliary stricture recurred once more, and IR drain placement was unsuccessful despite multiple attempts. The patient was therefore referred for an ERC. A Pentax EC-2990Li with a 2.8mm working channel was initially used and access to the hepatic duct, through anastomosis site was successful using a standard sphincterotome and the stricture was dilated. An attempt to place a 7 Fr stent was unsuccessful as it couldn’t be passed through the scope channel, so the scope was switched to a Pentax EC-3490LK with a 3.8mm working channel and a 7Fr stent was successfully placed. Discussion: Biliary complications post liver transplantation represent a considerable cause of morbidity and mortality. Biliary complication rate has been reported as 20-38% in pediatric liver transplantation with higher rate in duct-to-duct anastomosis compared to hepato-jujenal anastomosis . The most common complications are bile leaks and biliary strictures. Endoscopic management of biliary complications remains the preferred approach, due to its safety profile, as opposed to the percutaneous route and has been extensively reported in the adult population, and has been increasingly used in patients with Roux-en-Y reconstruction. Studies have shown that endoscopic management of biliary complications can minimize the need for post-transplant biliary surgery and is generally safe and effective The ideal endoscope and technique for endoscopic management in Roux-en-Y patients remains unclear. Nabeel et al. compared using a single-balloon enteroscope with variable stiffness colonoscopes in patient with Roux-en-Y anatomy in 199 procedures and NASPGHAN 1 1 1 1 2 2 1 1 (1). (2) (4). found that rates of biliary cannulation, therapeutic success and procedural success were higher with the use of single-balloon endoscopes and lowest with the use of pediatric colonoscopes . Herein we report the first pediatric case of performing ERC in a liver transplant patient with Roux-en-Y anatomy. Conclusions: Endoscopic management of biliary complications post liver transplantations in pediatric patients with Roux-en-Y anatomy is possible and considered as a safer alternative to percutaneous management.
-

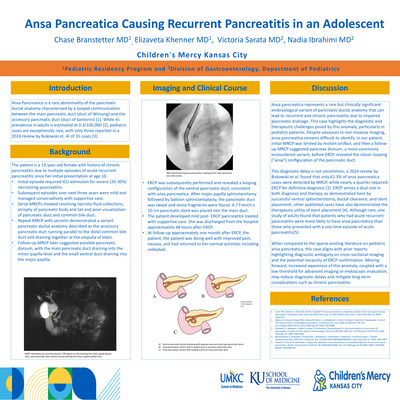
Intraductal Papillary Mucinous Neoplasm In An 18-year-old With Recurrent Pancreatitis
Nadia Ibrahimi, Thomas M. Attard, Moises Alatorre-Jimenez, Karie Robinson, and Syed Jafri
Introduction: Intraductal Papillary Mucinous Neoplasms (IPMNs) of the pancreas are premalignant, intraductal, mucin secreting cystic lesions. IPMNs are a rare entity in the pediatric population and commonly seen in men in their 6 to 7 decade. Pediatric IPMN has been previously reported in a 14-year-old and a neonate, who also had hyperinsulinism and a de novo germline SKIL gene mutation. . Kim et al. did a ten-year single centered pediatric pancreatic malignancy study discovering IPMN in one patient of 35 with pancreatic mass removals . Case: Our patient is an 18-year-old male who initially presented at the age of 15 with acute, then recurrent mild pancreatitis. His routine screening investigations including calcium, triglycerides, and IgG4 levels were normal. No mutations were detected upon pancreatitis gene panel including PRSS1, SPINK1, CFTR, CASR, CTRC, and CPA1 genes. The gallbladder was normal on abdominal ultrasonography, however Magnetic Resonance Cholangio Pancreatography (MRCP) showed focal irregular dilation of the pancreatic duct with a concern of santorinocele, which is a cystic dilation of the dorsal pancreatic duct.[ATM1] The patient underwent Endoscopic Retrograde Cholangio-Pancreatography (ERCP), and Endoscopic Ultrasound (EUS) with findings of mucin seen in the major papilla with a “fisheye” appearance (fig 1) and a cystic lesion measuring 7x22mm communicating with the pancreatic duct in the head of the pancreas (fig 2), respectively. Cytology was obtained through EUS guided fine-needle aspiration as well as aspirating mucus from the pancreatic duct during ERCP and both samples confirmed IPMN[ATM2] . Discussion: IPMN was first described in the 1980s but is increasingly recognized with the current incidence estimated as 0.48-2.04 per 100,000 . Pediatric IPMN is a premalignant lesion and typically progresses from IPMN adenoma, borderline dysplastic, carcinoma-in-situ and eventually to invasive carcinoma, usually within 5 years. IPMNs lesions are classified as main duct (MD-IPMN), branch duct (BD-IPMN) or mixed type with MTIPMN harboring a higher risk of malignant transformation. IPMNs are often diagnosed incidentally on imaging studies but can also present with abdominal pain or recurrent pancreatitis. It has been reported that patients presenting with pancreatitis are at high risk of harboring a malignancy . Worrisome Clinicopathologic features include cyst size ≥ 3 cm, thickened or enhancing cyst walls, main duct size 5–9 mm, non-enhancing mural nodules, an abrupt change in pancreatic duct caliber with distal pancreatic atrophy and lymphadenopathy. In addition, the incidence of extra-pancreatic neoplasms is higher in patients with IPMN, with reported rates of 25% to 50% Conclusion: Despite the rarity and low incidence of pediatric pancreatic tumors, especially IPMNs, the broad differential diagnosis of pediatric pancreatic lesions associated with pancreatitis has to include IPMNs especially in view of the potential malignant transformation.
-

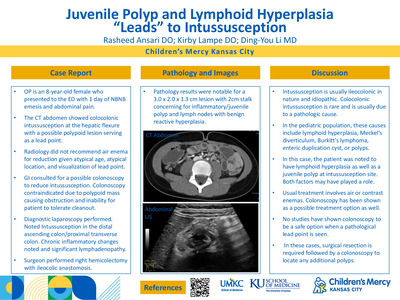
Inverted Appendix Presenting As Abdominal Pain And Lower Gastrointestinal Bleeding
Moises Alatorre-Jimenez and Thomas M. Attard
Background: Cecal polyps are challenging insofar as the region represents the highest risk of bleeding and perforation during polypectomy . In addition, polypoid lesions in the cecum may represent a morphologically abnormal ileocecal valve or an inverted appendix. Inadvertent polypectomy in those scenarios would lead to serious sequelae including perforation. Case report: Our patient is a 6-year-old male with a background history of prematurity, lactose intolerance, chronic esophagitis, gastritis, constipation, and painless rectal bleeding. He presented with a acute onset diffuse, severe abdominal pain associated with diarrhea that evolved to include hematochezia. At the time of presentation, he required aggressive resuscitation. His initial hemoglobin was 10mg/dl trending down to 7g/dl over 24 hours. His basic metabolic panel, coagulation panel, infectious stool studies, and calprotectin were negative or within normal limits. The patient stabilized following transfusion and octreotide infusion. Following a negative Meckel’s scan it decided to proceed to endoscopy. Upper endoscopy revealed normal findings whereas colonoscopy showed a pedunculated cecal polypoid lesion estimated at 3 cms diameter, with normal mucosal appearance, streaking erythema with superficial erosions (Fig1) but not actively bleeding. The lesion was recognized as likely protruding from the appendix consistent with appendiceal inversion (Type V; McSwain Classification) . Endoloop assisted appendectomy was not available and urgent surgery consult was obtained. The patient underwent uneventful laparoscopic appendectomy the next day. Histopathology report from the appendix was reported as eosinophilic infiltration with chronic active colitis consistent with presumed ischemic injury. The patient subsequently recovered uneventfully and was discharged home with no residual or recurrent symptoms at 4 month follow up. Discussion: Inversion of the appendix is a rare finding, with an estimated incidence of < 0.01% among all ages . It is theorized that inversion of the appendix may result from appendix peristalsis due to local inflammation or by appendix endometriosis . When symptomatic, inversion presents as abdominal pain, obstruction from intussusception, hematochezia, or diarrhea . Endoscopically an inverted appendix can be easily confused with polyp or neoplasia. Endoscopic removal of inverted appendix, when symptomatic can be achieved safely through endoloop ligation followed by distal (above endoloop) snare polypectomy.
-

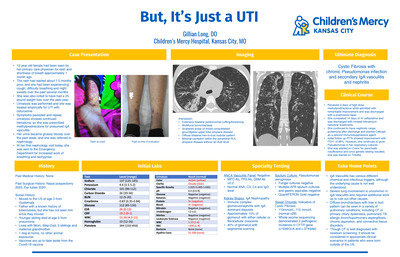
Management of Primary Spontaneous Pneumothorax: A Single Institution Protocol Analysis
Shai Stewart MD, James A. Fraser, Rebecca M. Rentea, Pablo Aguayo, David Juang, Jason D. Fraser, Charles L. Snyder, Richard J. Hendrickson, Tolulope A. Oyetunji, and Shawn D. St.Peter
Management of Primary Spontaneous Pneumothorax in Children: A Single Institution Protocol Analysis
Background: The Midwest Pediatric Surgery Consortium (MWPSC) has suggested a management algorithm to include simple aspiration of primary spontaneous pneumothorax (PSP), failing which, Video-Assisted Thoracoscopic Surgery (VATS) should be considered. We describe our outcomes in patients who have been managed with this suggested protocol.
Methods: An Institutional Review Board (IRB) approved, single institution retrospective analysis was conducted on all patients between 12 and 18 years who were diagnosed with PSP from 2016 to 2022. Initial management consisted of aspiration alone with a 12F Thal-Quick chest tube followed by clamping of the tube and chest radiograph at 6 hours. Success was defined asfailed.
Results: Fifty-nine patients were initially managed with aspiration, with a median age of 16.8 years (IQR 15.9, 17.3). Most of the patients were male (n=45, 76.2%) and white (n=50, 85%). Left sided pneumothorax was more common (n=38, 64%). Overall median LOS was 2.7 days (IQR 1, 3.5).
Aspiration was successful in 33% (20) of the patients and were subsequently discharged home, while 66% (39) required VATS. The median LOS for those with successful aspiration during the index admission was 20.4 hours (IQR 16.8, 34.8), while those who underwent VATS had a median LOS of 3.1 days (IQR 2.6, 4). In comparison, in the MWPSC study of which our site was a participant, the mean LOS for those managed with a chest tube after failed aspiration without progressing directly to VATS was 6.0 days (± 5.5).
Of those who had successful aspiration, 45% (9) had recurrent PSP, of which 1 had another successful aspiration and 8 required VATS after failed aspiration.
Of the 39 patients who initially underwent VATS after a failed aspiration, 25% (10) had recurrent PSP, of which 1 went on to have successful aspiration and 90% (9) required repeat VATS after another failed aspiration. The median time to recurrence for the successful aspiration group was shorter than that of the VATS group [66.6 days +/- 41.3 vs. 546.5 days +/- 166.5 (p=0.02)].
Conclusion: Simple aspiration is safe and effective for children with PSP as an initial managment, although most will require VATS either due to failed aspiration or recurrence of PSP. Early VATS appears to reduce overall length of stay.
-

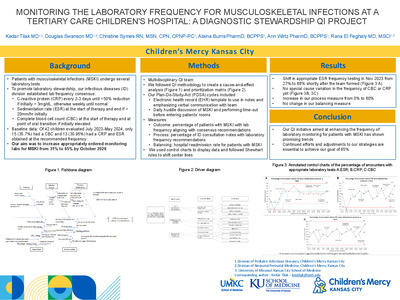
Repeat Tracheal Aspirates in Pediatric Intensive Care Patients: Frequency, Resistance and Antimicrobial Use
Edward Lyon, Jennifer Goldman, Brian Lee, Margaret Campbell, Rangaraj Selvarangan, and Elizabeth Monsees
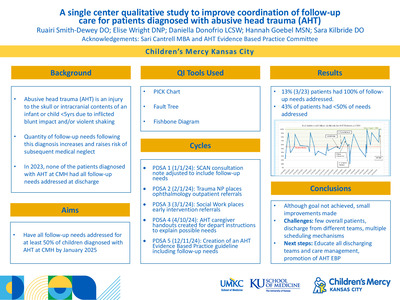
Background: Tracheal aspirates (TA) are frequently obtained in the pediatric intensive care unit (PICU); however, no data exists on the frequency or clinical management of multiple TA cultures on the same PICU patient. In this study, we describe the frequency of repeat TAs in PICU patients, the emergence of multidrug resistant organisms (MDRO), frequently cultured pathogens of TAs, and associated antibiotic prescribing patterns. Methods: We identified 70 PICU patients between 2018-2019 who met our criteria for retrospective chart review with ≥2 TAs obtained during their hospitalization. The following information was collected: patient demographics, number of TAs per patient, microbiology with susceptibilities, antibiotic use, and clinical data summarizing patient condition. Descriptive statistics established the frequency and time between initial and repeat TAs, reason for collection, antibiotic exposure, and frequency of MDRO development. Findings: Preliminary data on 15 patients showed 90 total TA cultures, with a median of 4 [IQR 2.5, 8] cultures per patient during their PICU stay (Figure 1). The median days between cultures was 10 [IQR 4, 26]. Most patients were < 5 years of age (n=14; 94%), male (n=13; 87%), and were admitted to the medical ICU service (n=8, 53%). Fever (46%) was the most common reason for TA collection followed by vital sign changes and secretion burden (34% and 32% respectively). A total of 133 organisms were isolated, with Pseudomonas aeruginosa (n=32), Methicillin-susceptible Staphylococcus aureus (n=16), and Klebsiella oxytoca (n=11) comprising the top pathogens (Figure 2). Eleven of the 15 patients (73.3%) had the same organism detected on ≥2 separate cultures. A total of 616 antibiotic days were prescribed with 149 (24%) antibiotic days prescribed for the TA result specifically. Six (40%) patients developed a MDRO after a median of 14.5 antibiotic days [IQR 11.75, 37.5]. Conclusions: Repeat TAs are performed in the PICU, often identifying the same pathogen repeatedly, likely representing colonization. Development of resistance is common and only one-fourth of TAs are directly treated with antibiotics. These data provide an opportunity to further explore clinical criteria to maximize the impact of TA cultures in the PICU.
-

Stewardship Opportunities for Cervical Lymphadenitis and Deep Neck Space Infections
Aaron Shaw, Brian R. Lee, Lauren Kazmaier, Emily Baker, Tina Dao, Sandra Arnold, and Angela Myers
Background: Cervical lymphadenitis (LAD) and deep neck space abscesses (DNSA) are common pediatric infections caused by similar bacteria. We sought to determine differences in presentation, diagnosis, and treatment between LAD and DNSA to identify antimicrobial and diagnostic stewardship opportunities. Methods: Charts were obtained using ICD9/10 codes for retropharyngeal and parapharyngeal abscessed (DNSA), and LAD between 1/1/10-12/31/20 from two pediatric centers. 1981 charts were identified. Charts were excluded if the diagnosis was not a bacterial infection (e.g. Kawasaki disease), if the LAD was not in the neck, or if caused by less common bacteria (e.g. tuberculosis). Data on presenting signs, symptoms, imaging, microbiology results, antibiotics, and surgical interventions were collected. Statistical analyses between LAD and DNSA groups were performed with Fisher’s exact and Wilcoxon rank-sum tests. Results: 1432 patients met inclusion criteria; 767 patients with LAD, 665 with DNSA. Median age and gender differed between LAD and DNSA, but no difference was seen in race between groups (Table). Presenting symptoms were different between groups (p <0.0001) (Figure). Almost all patients in the DNSA group received a CT scan, compared to 69% in the LAD group. Only 8% in the DNSA group had an ultrasound, in contrast to 50% in the LAD group. Most patients in both groups had a blood culture obtained; these were negative in ≥95% of all cases. Abscess cultures in the LAD group more commonly grew S. aureus, while S. pyogenes was more common in the DNSA group. Clindamycin was the most common antibiotic utilized; 91% of LAD, 87% of DNSA. Most patients received ≥2 antibiotics; 81% of DNSA and 63% of LAD (Table). Conclusions: These data may be used to help target diagnostic and treatment stewardship interventions for DNSA and LAD. Ultrasound alone may be sufficient for some cases of LAD, and CT reserved for DNSA when suspected based on presenting signs and symptoms. Routine blood cultures appear to be unnecessary for these patients. Multiple antibiotics are used to treat LAD when a single antibiotic may be more appropriate, given the prevalence of Gram positive organisms that would likely respond to clindamycin.
-

Two Siblings With Microvillous Inclusion Disease
Moises Alatorre-Jimenez, Brandi Weller, Meike Orlick, and William San Pablo
Introduction: Microvillous Inclusion Disease (MVID) (OMIM#251850) is a rare autosomal recessive condition caused by mutations or deletions mostly in the MYH6 gene but also STX3 and STXBP2 genes. It is characterized by protracted diarrhea with severe congenital alteration of the intestinal epithelium resulting in watery diarrhea, metabolic acidosis, failure to thrive, and permanent malabsorption that normally leads to a lifelong dependency on total parenteral nutrition (TPN) and the eventual possibility of bowel transplantation . Histological hallmarks of MVID in small intestinal biopsies are hypoplastic, atrophic, or disorganized villi without crypt hypertrophy, or immune cell infiltrate and, at the intestinal cellular level, microvillus atrophy, intracellular accumulation of brush border enzymes, and microvillus inclusions in the cytoplasm. It is caused by a dysfunction of myosin Vb protein encoded by the MYO5B gene; at least 41 different mutations have been discovered . It is thought that these mutations can cause intracellular trafficking defects causing impairment of the apical enterocytes recycling and reduced expression of the apical proteins at the brush border membrane; also, this defect can cause fusion of transport vesicles of brush border proteins in the cytoplasm causing the Microvillous inclusions . Objective: Present a case of MVID with confirmed clinical features and histology with a novel mutation in MYH6 and RYR2 genes. Case report: We report two siblings, the oldest sibling is four years old, and the youngest is two years old; both are TPN-dependent and diagnosed as neonates with MVID both of whom presented with severe congenital diarrhea. Histopathology revealed epithelial cells with poorly formed brush borders and many cells with intracytoplasmic inclusions. Electron microscopy showed microvilli-containing inclusions within the apical cytoplasm in the enterocytes. Genetic results revealed that both siblings have maternally inherited heterozygous deletion of 2.62 kb in exons 32-33 of the MYO5B gene. Conclusions: There are very few MVID cases reported in the literature. To date, 188 patients are registered in the International Microvillous Inclusion Disease Patient Registry . None of those patients were reported to have a heterozygous deletion involving exons 32-33 of the MYO5B gene.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}