
These posters have been presented at meetings in Children's Mercy and around the world. They represent research that was done at the time they were created, and may not represent medical knowledge or practice as it exists at the time viewers access these posters.
-
 is associated with culture positive sepsis and with increased need of escalation in respiratory support in very low birth weight infants more than seven days of life undergoing sepsis workup secondary to vitals instability in the form of multiple episodes of true apneas or bradycardia and desaturations associated with apnea by Kedar Tilak, Aashka Patel, and Anna Zylak")
Increased Red Cell Distribution Width (RDW) is associated with culture positive sepsis and with increased need of escalation in respiratory support in very low birth weight infants more than seven days of life undergoing sepsis workup secondary to vitals instability in the form of multiple episodes of true apneas or bradycardia and desaturations associated with apnea
Kedar Tilak, Aashka Patel, and Anna Zylak
Background Apnea of prematurity is nearly universal among very low birth weight infants (VLBW). In VLBW infants, changes in clinical status usually occur due to sepsis or non-infectious causes and it is challenging to differentiate between the two. We as clinicians use irregularities in vital signs as an early warning sign of sepsis to facilitate early treatment and improve patient outcomes. Adults have used RDW as a marker of worsening respiratory status and mortality from acute respiratory distress syndrome (ARDS). In this study, we seek to investigate elevations in Red Cell Distribution Width (RDW) as markers for culture positive sepsis and need for escalation of respiratory support in VLBW neonates. Methods We did a retrospective chart review using the Electronic Medical Records (EMR) of VLBW infants (< 1500g) admitted to the Neonatal Intensive Care Unit (NICU) of a community hospital over 3 years. We included all babies who had True apnea (apnea > 20 seconds) or apnea with bradycardia and desaturations, after day seven of life and had CBC tests sent and were being managed for presumed late onset sepsis secondary to this vital sign instability. Other demographic data was gathered and tabulated. The data was analyzed to check for association between increased red cell distribution width (RDW) and need for escalation of respiratory support. Escalation in respiratory support included an increased need of assisted ventilation to support breathing. We also looked at positive blood / urine cultures and RDW values. Results 50 babies matched our inclusion criteria. 31 babies had a positive blood /urine culture. 21 of the 31 had elevated RDW which was statistically significant at p< 0.05 (Table1), hence showing that positive culture late onset sepsis had elevated RDW. Also, we saw increased need for escalation in respiratory support amongst culture positive babies with an elevated RDW at p < 0.05 (Table 2). Conclusion We conclude from this, that elevations in RDW is a marker for VLBW babies needing escalation in respiratory support. Elevations were also seen in culture positive sepsis. More studies need to be done as most of the available data is in adults. We can look more associations in babies with RDS (respiratory distress syndrome) and predict respiratory distress and for early interventions and better outcomes.
-

Intraoperative Status Asthmaticus in a Morbidly Obese Preteen Undergoing Concomitant Vertical Sleeve Gastrectomy and Orthotopic Liver Transplant
Abigail Pint, Neal Campbell, and Preethi Tumati
10-year-old morbidly obese male with cirrhotic ESLD secondary to vertically transmitted Hepatitis C presented for liver transplantation and concomitant vertical sleeve gastrectomy. Other history included moderate persistent asthma, OSA, and presumed HPS with baseline SpO2 of 94%. Induction was smooth; intubation with an armored ETT was easy. During invasive monitor placement, bronchospasm worsened SpO2. Continuous albuterol nebulization provided reasonable reversal, and all stakeholders agreed to proceed. Postoperative course was complicated by status asthmaticus and dramatic extubation on POD3 when patient bit and kinked armored ETT. To date, patient has good graft function and a 16% reduction from his peak BMI.
-

Variables affecting neurodevelopmental outcome in infants with critical congenital heart disease
Elizabeth Loughman, Marcie G. Files, and Julie Weiner
Background: The mortality of cardiac conditions in infancy is improving with advances in surgical planning and medical management. Neurologic morbidity remains significant. Clinically correlating an infant with their neurologic exam, MRI/EEG, and subsequent developmental testing remains a challenge. Counseling regarding neurologic outcomes after cardiac intervention is difficult due to the wide range of findings that can sometimes be clinically irrelevant. Purpose: The goal of this study is to identify factors associated with poor neurodevelopmental outcomes in infants with critical congenital heart defects (CCHD) as assessed by the Bayley Scales of Infant and Toddler Development Edition IV (Bayley). Methods: This is a retrospective single site study performed at a freestanding children’s hospital with delivery services. Neonates were inborn or admitted to the neonatal/cardiac intensive care units following diagnosis of CCHD over a 5-year period who required cardiac surgical procedures during their initial hospital stay. Patients were sampled from databases in the heart center and the Children’s Hospital Neonatal Consortium. Neonates were stratified by single vs biventricular repair and Norman category of heart defect (A, B, or C). Primary outcomes included neurologic exam, MRI, and EEG at discharge and 12- and 24-month Bayleys. Results: 383 neonates were included in analysis. 57.2% were male with an average gestational age of 39 weeks and average birthweight of 3.2kg. The average length of stay was 36 days. Of the entire sample, 36.3% had Bayleys performed at 12 months and 25.8% at 24 months. 38% of the entire sample underwent a single ventricle repair. 39% were classified as Norman A, 41% Norman B, and 19% Norman C. 40% of Bayleys were abnormal, with highest impairment in gross motor skills and expressive language. Of the 145 infants with EEGs, 17% showed seizures or focal slowing. Of these abnormal EEGs, approximately 45% had an abnormal Bayley. Of the 146 infants with MRIs, 58% showed ischemia, infarct, atrophy, stroke, or hemorrhage. The odds in favor of an abnormal Bayley at 12 months was 3.11 times higher among infants with abnormal MRIs (95% CI 1.22-7.94, d= 0.63). 6.5% had an abnormal neurologic exam, most commonly hypotonia. Of these abnormal neurologic exams, 73% had abnormal 12-month Bayleys and 87.5% had abnormal 24-month Bayleys. Conclusion: Abnormal neurologic exams, MRI, and EEG at discharge can be associated with abnormal Bayleys in childhood. This helps in counseling families and providing long term neurodevelopmental follow up.
-

A Genomics Driven Human Induced Pluripotent Stem Cell Model of Infant ALL – Updates on Hematopoietic Differentiation
Meagan Vacek, Jacqelyn Nemechek, Irina Pushel, Priyanka Kumar, Bradley Thornton, Molly Leyda, Midhat Farooqi, Erin Guest, Jay L. Vivian, and John M. Perry
Acute lymphoblastic leukemia in infants (iALL) is a high-risk subtype of childhood leukemia, with poor survival outcomes despite intensive therapies. Rearrangement of KMT2A (KMT2A-r) occurs in 70% of cases and is associated with chemotherapy resistance, early relapse, and rapid leukemic progression, all of which contribute to poor survival outcomes. The most common KMT2A-r in iALL is KMT2A::AFF1 (MLL::AF4), derived from t(4;11)(q21;23). This KMT2A-r generates a driver fusion oncogene which leads to epigenetic dysregulation of target gene transcription. Infant ALL’s cell of origin is thought to be a very early hematopoietic precursor, with transcriptomic studies of iALL blasts showing similarities to hematopoietic stem and progenitor cells (HSPCs), multipotent progenitors and early lymphoid progenitors (ELPs). Unfortunately, research into this devastating disease has been hampered by the lack of a representative model of iALL Attempts at creation of an iALL models have led to a variety of results including myeloid neoplasms, lymphomas, myeloid/lymphoid hyperplasia or leukemia, mature B cell neoplasias, or in one instance, a B-lymphoblastic leukemia with prolonged latency. Because of these failures, much remains unknown regarding how KMT2A::AFF1 transforms early hematopoiesis or how it alters the severity of the disease. To understand the developmental state of the cell of origin and progression of iALL, we have created a highly controlled human inducible pluripotent stem (iPS) cell model of KMT2A::AFF1 iALL. Specifically, we engineered human iPS cell lines with doxycycline regulatable expression of KMT2A::AFF1 fusion and have confirmed expression of the KMT2A::AFF1 transcript. Through directed differentiation we have also produced functional HSPCs from iPS cells with multilineage differentiation capacity, as evidenced by differentiated cells being transcriptionally similar to erythrocytes, megakaryocytes, and monocytes. The iPS cells are currently being guided through lymphocyte differentiation. This model has allowed us to recapitulate hematopoietic ontogeny with the ability to control iALL induction at specific developmental stages. We are using single cell genomics to investigate transcriptomic changes during hematopoietic differentiation of our KMT2A:AFF1 iPS cell line. Through this research we expect to discover the genomic and epigenetic landscape and cellular evolution of iALL with the long-term goal to uncover targets specific to iALL for the development of new therapies.
-

"Ghosts in This Country": Pediatric Caregiver Perspectives on Immigration Status in the Healthcare Setting
Anik Patel, Ali Fowler, Juan Farias Torres, Ana Contreras, Claudia Zepeda, Estefania Bazan, John Cowden, Frances Turcotte Benedict, Jennifer Watts, and Kimberly A Randell
Background: There are approximately 11.4 million undocumented immigrants (UI) in the United States. Immigration status (IS) is a unique social determinant of health that directly and indirectly impacts health and healthcare access. There are gaps in our understanding about how IS impacts health, particularly because it is not frequently discussed in the healthcare setting. This study expands our understanding of immigrant caregiver perceptions about discussing IS in the healthcare setting and provides insight into specific needs that we may not be currently addressing. Methods: Setting: ED or Spanish-speaking majority pediatric clinic at Children's Mercy Inclusion criteria: Caregivers who are 18+, identify as Latin/Hispanic, are Spanish-speaking, and do not have a social security number Exclusion criteria (determined by study team): Caregivers of critically ill patients or patients undergoing sensitive exam, caregivers with developmental delays Recruitment: Potential participants identified by Spanish preference on clinic schedule/ED tracking board. Confidentiality was stressed and a private setting was offered for interviews after screening/enrollment Data Collection: Demographic data was collected using a REDCap-based survey. 20 interviews were conducted from April 7, 2023 to February 28, 2024. The interview guide was developed by iterative repetition by a diverse author group. All interviews were conducted in-person with bilingual individuals. Remuneration: $50 gift card and list of resources in Spanish/English Data Analysis: Interviews were recorded using an audio recorder and then transcribed into Spanish/English. 3 independent coders analyzed de-identified transcripts using an inductive approach. Results: Theme 1: UIS negatively impacts multiple aspects of health, but many people do not connect UIS with health. Theme 2: There are many perceived barriers to disclosure of UIS, but varied perspectives on whether providers should discuss IS in the healthcare setting. Theme 3: There are many barriers to resource utilization for UI. Theme 4: There are a variety of needs in the community and many UIS seek these resources from varied places, but many also don’t know where to go for information. Theme 5: There are things that medical teams can do to facilitate resource utilization and discussion about IS in the healthcare setting, but one size does not fit all. Conclusion: Caregivers offered perspectives on the impact of UIS on health and identified barriers to and facilitators of discussing immigration status while in healthcare settings. Universal provision of resource information may more effectively support families with caregivers who are undocumented immigrants
-

System-based integrated comprehensive simulation program in pediatric residency education: our institutional experience
Mahmoud Jaara, Jenn M. Zimmerman, Jean Ann Hutton, Nancy Joseph, and Maritza Plaza-Verduin
Background: Simulation provides the opportunity for learners to bridge the gap between evidence-based theoretical knowledge and clinical practice experience. Residency programs often utilize simulation to expose the learners to various patients who are presenting in extremis in a safe environment. This empowers the trainee by providing them with tools and experiences to enhance their pediatric education. Simulation is also utilized to practice non-technical skills like team dynamics and communication in a psychologically safe setting. Despite the widespread use of simulation in pediatric residency programs, there remains a gap in standardization. In response to this gap, we sought to create a comprehensive, system-based curriculum (clinical skills and clinical scenarios) that integrated simulation and system-based traditional didactic learning. Methods: Our methodology embraced a comprehensive approach, emphasizing essential topics and clinical skills pertinent to each system through didactic lectures during our academic half-day sessions. Starting with an 18-month calendar outlining didactics, we meticulously planned a corresponding simulation calendar. This calendar included a 3-4-hour session in the simulation center every six weeks. During that session, residents would participate in clinical simulation scenarios (both emergency and non-emergency) and clinical procedures skills stations. Along with these half-day sessions, we incorporated monthly in situ simulations during day and night shifts involving multi-disciplinary team members, including nurses and respiratory therapists. A dedicated Simulation Task Force comprising faculty and fellows was convened. Simulations were meticulously aligned with the content outline provided by the American Board of Pediatrics (ABP) and ensured adherence to Accreditation Council for Graduate Medical Education (ACGME) task lists. Evaluation of simulation activities was conducted through post-surveys gauging participants' comfort levels across various clinical scenarios. Each clinical Simulation scenario has to cover vital components: medical critical actions and team dynamics and communications skills, acquired skills, and pattern recognition at the end of the sim. Results: Our review of resident simulations conducted over the past year yielded insightful findings. In our post-surveys, 100% of the respondents stated that the integrated simulations reinforced their knowledge or allowed them to gain new knowledge or skills and that the experience improved their confidence in their own knowledge or skills. Over 50% of the participants indicated that they felt the skills they practiced would apply to their jobs and help them provide safer patient care. Conclusion: By integrating simulation within a system-based curriculum, our approach offers a structured pathway to enhance pediatric residency education, fostering a more standardized and effective learning experience. Reviewers comment(s) regarding your abstract: This abstract describes the integration of simulation to didactic learning during academic half day sessions, which should allow residents the ability to apply what was learned in a safe, simulated environment. While it is helpful to recognize that residents reported that the simulations allowed application and would create a safer environment, were other higher level metrics collected? Perhaps metrics related to resident performance in the simulations or safety related data before and after the restructuring of the curriculum? The abstract was confusing as I was unable to tell why this study was performed (no needs assessment), who performed the simulations, what simulations were performed, and why the simulations were done. In the future, abstract would benefit from more clarity or for a graph/image to describe the intervention further.
-

Association Between Neighborhood Opportunity and Youth Mental Health Emergency Department Visits
Shelby Chesbro, Matt Hall, Adrienne DePorre, Molly Krager, Laura Plencner, Shayla Sullivant, and Henry T. Puls
-

Variables affecting neurodevelopmental outcomes in infants with critical congenital heart disease
Elizabeth Loughman, Marcie G. Files, and Julie Weiner
Background: The mortality of cardiac conditions in infancy is improving with advances in surgical planning and medical management. Neurologic morbidity remains significant, and clinically correlating an infant with their neurologic exam, MRI/EEG, and subsequent developmental testing remains a challenge. Counseling parents regarding neurologic outcomes after cardiac intervention is difficult due to the wide range of findings that can sometimes prove to be clinically irrelevant. Purpose: The goal of this study is to identify factors associated with poor neurodevelopmental outcomes in infants with critical congenital heart defects (CCHD) as assessed by the Bayley Scales of Infant and Toddler Development Edition IV (Bayley). Methods: This is a retrospective single site study performed at a freestanding children’s hospital with delivery services. Neonates were either inborn or admitted to the neonatal or cardiac intensive care units following diagnosis of CCHD over a 5-year period who required cardiac surgical procedures during their initial hospital stay. Patients were sampled from databases in the heart center and the Children’s Hospital Neonatal Consortium. Neonates were stratified by single vs biventricular repair and Norman category of heart defect (A, B, or C). Primary outcomes included neurologic exam, MRI, and EEG at discharge as well as 12- and 24-month Bayleys. Results: 383 neonates were included in analysis. 57.2% were male with an average gestational age of 39 weeks and average birthweight of 3.2kg. The average length of stay was 36 days. Of the entire sample, 36.3% had Bayleys performed at 12 months and 25.8% at 24 months. 38% of the entire sample underwent a single ventricle repair. 39% were classified as Norman A, 41% Norman B, and 19% Norman C. Approximately 40% of Bayleys were abnormal, with highest impairment in gross motor skills and expressive language. Of the 145 infants with EEGs, 17% showed seizures or focal slowing. Of these abnormal EEGs, approximately 45% had an abnormal Bayley. Of the 146 infants with MRIs, 58% showed ischemia, infarct, atrophy, stroke, or hemorrhage. The odds in favor of an abnormal Bayley at 12 months was 3.11 times higher among infants with abnormal MRIs (95% CI 1.22-7.94, d= 0.63). 6.5% had an abnormal neurologic exam, most commonly hypotonia. Of these abnormal neurologic exams, 73% had abnormal 12-month Bayleys and 87.5% had abnormal 24-month Bayleys. Conclusion: Abnormal neurologic exams, MRI, and EEG at discharge can be associated with abnormal Bayleys in childhood. This study helps delineate risk factors in infants with congenital heart defects that could aid in predicting long-term neurodevelopmental outcomes.
-

3D Bioprinting the Tumor Microenvironment for Immunotherapy Development
Molly Leyda, Tykeem Manor, John Szarejko, Douglas Myers, and John M. Perry
The tumor microenvironment (TME) is a complex system that plays a crucial role in tumor progression, immune evasion, and therapy resistance. The TME is composed of various cell types, including tumor cells, stromal cells, and immune cells such as macrophages. Macrophages are versatile myeloid cells which can exhibit both pro-tumoral and anti-tumoral functions, depending on their phenotype and the TME context. M1 macrophages have demonstrated promising pro-inflammatory and anti-tumor effects, while tumor associated M2 macrophages (TAMs) play an anti-inflammatory role and promote tumor immune escape. Understanding the complex interactions between TAMs and the TME is, therefore, essential for developing effective anti-cancer immunotherapies. The pre-clinical development of immunotherapies necessitates using both in vitro and in vivo tumor models. Classical 2D in vitro models are relatively fast and inexpensive but lack the spatial complexity and heterogeneity of the TME. In vivo mouse models provide a more physiologically relevant system for evaluating therapies; however, they are time consuming, expensive, and deficient in several immune cell types, so they fail to accurately recreate the TME. 3D bioprinting technology offers a novel approach for creating complex in vitro models of the TME, allowing for the rapid and cost-effective creation of tissue constructs that mimic the composition of native tissues. Our research is focused on using this technology to recreate the TME by incorporating myeloid, stromal, and tumor cells into 3D bioprinted structures. Utilizing these models, we are investigating the cellular interactions which drive the formation of the TME to gain insights into the enigmatic functions of TAMs. Additionally, these models will aid in the development of novel anti-cancer immunotherapies able to evade or repolarize the immunosuppressive TME. Our creation of 3D bioprinted tumor models will facilitate collaborative efforts to screen a wide range of innovative therapies and support translation from bench to bedside
-

Post-Operative Diagnosis of Anomalous Left Coronary Artery From The Right Pulmonary Artery via Transthoracic Echocardiogram
Lavina Desai, Sanket Shah, Edo Bedzra, and Christopher Mathis
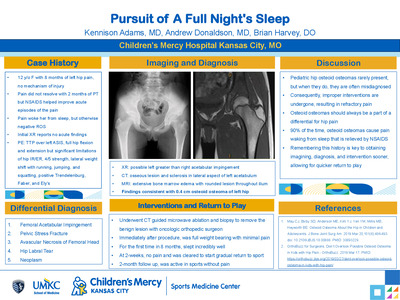
A term infant female was diagnosed with a ventricular septal defect (VSD) and aortic coarctation. Preoperative echocardiography and computed tomography angiography (CTA) showed a normal right coronary artery origin, but inconclusive left coronary artery (LCA) origin. There was a normal flow profile in the LCA by echocardiography. She underwent repair with extended end-to-end anastomosis and VSD closure during which surgical inspection revealed a usual appearing, retro pulmonary path of the LCA towards the left sinus of Valsalva. Postoperative echocardiogram revealed mild global dysfunction but no regional wall motion abnormalities. Repeat echocardiogram revealed severe dysfunction most prominent in the anterolateral and posterolateral segments from base to apex. There was new, bidirectional flow in the LCA and abnormal diastolic flow in the posterior right pulmonary artery (RPA) raising suspicion for anomalous origin of the LCA from the RPA (ALCARPA). Cardiac catheterization confirmed the diagnosis. Echocardiography plays a vital role in detection of ALCARPA. However, the usual clues of flow reversal in the LCA, abnormal diastolic flow in the pulmonary artery and sequelae of left ventricular ischemia vary with age and pulmonary artery pressure. CTA is valuable in diagnosis but may suffer from improper contrast timing and motion artifact. When the LCA originates from the RPA, the origin appears normal due to its proximity to the left sinus of Valsalva, even by visual inspection. Meticulous coronary imaging and clinical suspicion are required for timely detection. Invasive angiography is the gold standard for diagnosis. There are few cases associating ALCARPA with aortic coarctation. Presence of a coarctation and VSD lead to sufficient pulmonary hypertension for antegrade LCA flow which hinders the preoperative diagnosis. This case is unique because the coronary anatomy was interrogated before surgery, but ALCARPA was not demonstrated due to a low index of suspicion for this rare anatomy and associated pulmonary hypertension. This case highlights the diagnostic challenge of this association of defects and reiterates the importance of definitive coronary imaging preoperatively. Persistent myocardial dysfunction following coarctation and VSD repair should prompt careful evaluation for ALCARPA.
-

Rhabdomyolysis As a cause of PTH independent hypocalcemia in a child with acute influenza infection
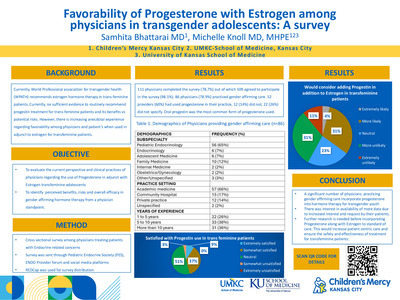
Samhita Bhattarai and Kelsee Halpin
INTRODUCTION Hypocalcemia is characterized by abnormally low level of calcium in the blood. Normal reference range for calcium for children between 12- 19-year-old is 8.5-10.6 mg/dl . Severe hypocalcemia is considered as serum calcium level of <7 mg>/dl and can present with tetany, seizures, and life-threatening cardiac arrhythmias. Etiology of hypocalcemia varies but hypoparathyroidism, pseudohypoparathyroidism and Vitamin D deficiency are some of the most common causes encountered by pediatrician endocrinologists. Association of rhabdomyolysis with hypocalcemia and elevated PTH is a rare presentation that should be considered, particularly for those children presenting with acute viral illness. We present a rare case of rhabdomyolysis associated with hypocalcemia not related to hypoparathyroidism. CASE A 12-year-old female presented to the emergency department with body ache, decreased oral intake and vomiting. She was found to be influenza positive. Electrolytes showed hypocalcemia (4.8 mg/dl). She subsequently had an undetectable 25-OH vitamin D level (<5 ng>/ml) and elevated iPTH level (609 pg/ml). We discussed the possibility of her etiology of hypocalcemia to be Vitamin D deficiency although her presentation was atypical at an older age with a negative imaging for rickets, hyperphosphatemia (6.0 mg/dl), and normal alkaline phosphatase (334 unit/L). She also did not have any phenotypic features of Albright’s hereditary osteodystrophy and renal function was within normal limits. She was identified to have elevated creatinine kinase (4829 U/L) supporting rhabdomyolysis secondary to acute influenza as a cause of her hypocalcemia. Rhabdomyolysis, a known complication of influenza infection, causes cell membrane destruction which impairs the normal function of Na-K-ATPase channel. This leads to increase in intracellular sodium activating Na/Ca exchanger which in turn causes influx of calcium intracellularly causing hypocalcemia. Additionally, any injury or infection leads to high phosphorus release from cells due to cell lysis. High phosphorus is also caused by reduced oxidative metabolism in muscles impairing phosphate use. This excess of phosphate then combines with calcium and causes calcium-phosphate complex in soft tissues. Hyperphosphatemia also additionally inhibits 1 alpha hydroxylase limiting formation of calcitriol leading to hypocalcemia. CONCLUSION Our patient had severe hypocalcemia due to influenza-related rhabdomyolysis. Rhabdomyolysis is an important consideration as a cause of hypocalcemia in children, especially with acute viral illness. Accordingly, it is also important to obtain serum electrolytes in patients presenting with rhabdomyolysis as hypocalcemia may lead to complications like seizures and cardiac arrhythmia if not appropriately recognized and treated.
-

Children's Mercy: Dedicated to All Children, Everywhere
Heather Steel, Katie Dayani, Julia McBride, Keri Swaggart, and Kim Weir
Children’s Mercy Kansas City was founded in 1897 by sisters Drs. Alice Graham and Katharine Richardson. Their primary objective was to create a hospital where the children of Kansas City and surrounding areas could be treated regardless of their religion, race, or ability to pay. By the early 1920’s segregation became a huddle to accomplishing this dream. To circumvent this problem Dr. Katharine Richardson partnered with Dr. John E. Perry and the staff at Wheatley Provident Hospital, the first private Black hospital in Kansas City, MO, to establish the Mercy Model Ward. This ward provided pediatric care for the Black children in Kansas City and was the first of its kind in the nation. Dr. Richardson was fully committed to providing care to all children, everywhere and this model ward provided the means for her to truly realize her goal.
-

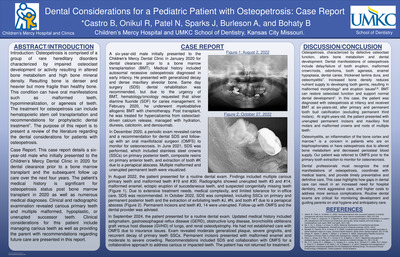
Dental Manifestations and Management of a Pediatric Patient with Hypophosphatasia: Case Report and Literature Review
Dev Patel, Robin Onikul, Amy Burleson, Brenda S Bohaty, Jenna Sparks, and Neena Patel
Hypophosphatasia is a rare autosomal recessive disorder affecting the ALPL gene, which is involved in mineralization of bones and teeth. Given the importance of mineralization on proper tooth development, patients with hypophosphatasia present with numerous dental manifestations and require careful, coordinated care to maintain function and esthetics. This case report details a 9-year-old patient presenting to Children’s Mercy Kansas City Dental Clinic with complex medical history including hypophosphatasia, hypophosphatemic rickets, and developmental delay. The case report will include the patient’s clinical and radiographic presentation and will detail the patient’s treatment history. The presentation will also review the relevant scientific literature regarding hypophosphatasia and the clinical expectations for overall care.
-

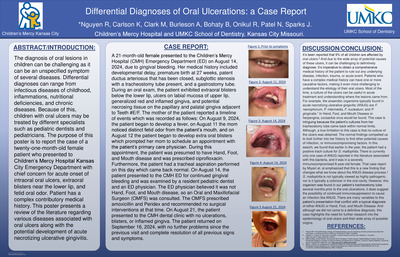
Dental Manifestations of a 4-year old Male Patient with Congenital Vitamin D Rickets: Review of the Literature and Report of a Case
Richard Nguyen, Robin Onikul, Brenda S. Bohaty, Neena Patel, Jenna Sparks, and Amy Burleson
Patients that present with Vitamin D-resistant rickets may have abnormal tooth morphology, such as enlarged pulp horns that may extend into the dentino-enamel junction. As a result of this communication, there may be an increased chance of pulpal infection, resulting in spontaneous dental abscesses occurring without evident caries or history of trauma. The purpose of this poster is to report the case of a four-year-old patient who presented to Children’s Mercy Kansas City Dental clinic with chief concern for swelling of the face with unknown causes. The patient’s medical history was significant for congenital Vitamin D-resistant rickets. The poster presents a review of the literature regarding various dental treatment considerations for patients with Vitamin D-resistant Rickets and discusses the dental and medical implications of Vitamin D-resistant Rickets for future care.
-

Differential Diagnosis of a 12-year-old Presenting with a Nodular-Sessile Lesion on the Hard Palate: Review of literature and report of a case.
Meredith Clark, Robin Onikul, Amy Burleson, Brenda S. Bohaty, Jenna Sparks, Neena Patel, and A Naidu
Soft-tissue lesions in children present with a wide range of etiologies, including those related to normal development, underlying systemic illness and/or those associated with benign or malignant tumors1 . In children and adolescents, the most common soft tissue lesions include, aphthae, fibromas, papillomas, pyogenic granulomas and traumatic lesions all of which may present on the hard palate.2 This case report details a 12-year-old female presenting to Children’s Mercy Dental Clinic with a chief complaint of a flesh-colored nodular sessile lesion visualized on the anterior hard palate, directly posterior to teeth #8 and #9. The patient’s medical history is non-contributory, and she has no known allergies. The purpose of this report is to present the relevant patient findings noted in this case including the clinical and radiographic exam, differential diagnosis, and referral for definitive treatment. A literature review of intra-oral soft tissue lesions in pediatric patients will also be presented.
-

February in Santiago Atitlan, Guatemala
Grace Milburn
Describes her experience working in Santiago Atitlan, Guatemala.
-

Space Loss After Removal of a Band and Loop Space Maintainer: A Case Report and Review of the Literature.
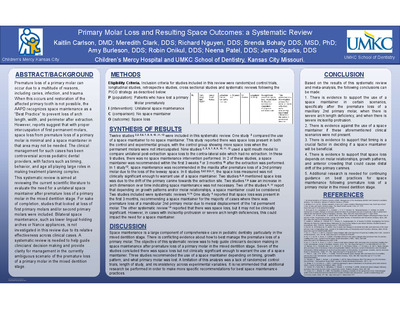
Kaitlin Carlson, Robin Onikul, Amy Burleson, Jenna Sparks, Neena Patel, and Brenda S. Bohaty
Premature loss of a first primary molar can occur due to a multitude of reasons, including caries and infection. When this occurs and restoration of the affected primary tooth is not possible, the AAPD recognizes space maintenance as a “Best Practice” to prevent loss of arch length, width, and perimeter after extraction. However, reports suggest that with proper intercuspation of first permanent molars, space loss from premature loss of a first primary molar is minimal and space maintainers in that area may not be needed. This case report details an 8-year-old female who had significant space loss between the mandibular primary canine and mandibular second primary molar after removal of her band-and-loop space maintainer post-eruption of tooth #19. Patient’s medical history is non-contributory, and she has no known allergies. This report reviews the pertinent literature regarding space management in the mixed dentition and outlines factors to be considered in making clinical decisions regarding such management.
-

The Impact of Health-Related Social Needs on Health Outcomes among Youth Presenting to a Midwest Pediatric Diabetes Clinic Network
Jasmine Roghair, Emily DeWit, Katelyn Evans, Mitchell Barnes, Heather Feingold, Samantha Jacob, Courtney M. Winterer, Jeffrey D. Colvin, Mark A. Clements, Shilpi Relan, and Kelsee Halpin
Objective: Screening for health-related social needs (HRSNs) is recommended as part of routine diabetes care given the strong impact of social factors on health outcomes. Our objective was to compare diabetes-related health outcomes among youth presenting to a tertiary diabetes center based on whether they screened positive or negative for HRSNs at a routine clinic visit. Methods: Baseline data were collected from patients whose parent/guardian completed a HRSN screen as part of their child’s diabetes clinic intake from 9/1/21 to 8/30/22. The screen is a 6-item questionnaire adapted from the Accountable Health Communities HRSNs Screening Tool. Longitudinal data were analyzed from the time of first screen through 8/30/23. Comparisons were made using chi-square or t-test. Results: Among 1880 unique respondents, 14% were positive for at least one HRSN. The most common HRSN was food insecurity (72%). A positive HRSN screen was more likely in non-white minorities (22% vs. 11% non-Hispanic white youth), publicly insured (22% vs. 8% privately insured), youth with a type 2 diabetes diagnosis (32% vs. 12% with type 1 diabetes), all p<0.001. Those with a positive vs. negative HRSN screen at baseline were more likely to have any A1c > 10% (32% vs. 19%), any A1c >13% (9% vs. 4%), at least one no-showed appointment (41% vs. 26%), a positive PHQ4 screen for anxiety/depression (22% vs. 11%), and a second positive HRSN screen (29% vs. 5%), all p<0.001, during the follow up period (mean 14.8 =/- 2.0 months). They were more likely to have an ED visit (17% vs. 12%, p 0.025), though DKA admissions were not significantly different between the groups (6% vs. 4%, p=0.15). Insulin pumps (58% vs. 75%) and continuous glucose monitors (CGMs) (58% vs. 76%) were also less utilized throughout the study period in those screening positive for a HRSN at baseline, p<0.001. Conclusion: Youth with positive HRSN screenings during diabetes clinic appointments experience suboptimal diabetes-related outcomes, including higher A1c levels, increased rates of missed appointments, anxiety/depression, ED visits, and less utilization of diabetes technologies. This highlights the importance of addressing social risk factors when treating youth with diabetes to enhance equity in delivery of care and improve health outcomes.
-

The Role of Adverse Childhood Events on the Progression of Chronic Kidney Disease in Children: A CKiD Study
Ana Cortez, Matthew Matheson, John Cowden, Bradley Warady, and Darcy K. Weidemann
There is a paucity of research on the relationship between adverse childhood events (ACEs) and chronic kidney disease. The effect of ACEs on the long-term health outcomes of cardiovascular disease, cancer, and chronic lung disease first emerged in a paper published in 1998. The National Institutes of Health sponsored the ACE Study, which Kaiser Permanente carried out in California. The study used a 17-question survey addressing seven exposures: psychological, physical, contact-sexual abuse, substance abuse, mental illness, mother being treated violently, and criminal behavior in the household. The results revealed a strong relationship between childhood exposure to ACEs and health outcomes. When individuals experienced four or more such exposures, the odds ratio ranged from 1.6 to 3.9 for ischemic heart disease, cancer, stroke, chronic bronchitis or emphysema, and diabetes (Vincent et al., 1998). This monumental analysis remains a focal point in research more than twenty years after the initial publication of its results. Since then, numerous studies have investigated how childhood exposures can increase disease risk. Surprisingly, chronic kidney disease (CKD) has received little attention in terms of the influence of ACEs in the pediatric and adult populations. Objective Specific Aim #1: Characterize the prevalence of ACEs in the CKiD cohort. Specific Aim #2: Characterize disease progression among those who experienced ACEs compared to those who have not.
-

Thyroid Dysfunction in Patients Receiving Immune Checkpoint Inhibitors
Emily Metzinger, Jennifer Boyd, Julia Broussard, and Christopher Klockau
Objectives: The use of immune checkpoint inhibitors (ICIs) in cancer treatment is increasing. Literature about endocrinopathies associated with ICIs in children is limited. This study investigates ICIs and thyroid dysfunction in pediatric patients at one institution.
Methods: Retrospective chart review of patients ages 1 to 19 was completed who received any of the following ICIs between January 2000 and November 2023: PD-1 inhibitors (nivolumab or pembrolizumab), PD-L1 inhibitors (durvalumab or atezolizumab), and CTLA-4 inhibitors (ipilimumab or tremelimumab). Patients were excluded if thyroid function tests (TFTs) were not available to review or if patients passed away within 30 days of ICI initiation. TFTs were considered abnormal if they were outside the reference range for age.
Results: Data analysis included nineteen patients. Of these, thirteen patients received nivolumab and three patients received multiple ICIs. Average age at time of ICI initiation was 14.9 years. Baseline TFTs were obtained in fourteen patients at ICI initiation and ten of these patients also had TFTs checked after initiation. Abnormal TFTs were seen in five patients after starting ICI therapy; four of these patients received nivolumab and one received pembrolizumab. Average time to thyroid dysfunction from ICI initiation was 3.3 months. Levothyroxine (LT4) was started in three patients for persistent abnormal TFTs (one patient had central hypothyroidism and two patients had primary hypothyroidism). Average time to LT4 treatment was 4.2 months. Two patients developed hypothyroidism prior to starting ICI therapy. Of these, one patient developed hyperthyroidism 2.9 weeks after ICI initiation. Hyperthyroidism resolved with temporary LT4 discontinuation, followed by restarting LT4. Six patients had baseline abnormal TFTs with ICI initiation of which two patients required levothyroxine.
Conclusions: Thyroid dysfunction can be seen within several months of ICI initiation, particularly PD-1 inhibitors. Hypothyroidism and hyperthyroidism were seen, though hypothyroidism was more common. This study supports monitoring TFTs (both TSH and free T4 levels) at baseline and during therapy with ICI. Limitations to our study include small patient population. Future studies should look at development of other endocrinopathies in children such as diabetes mellitus or adrenal insufficiency.
-

Understanding Inpatient Diagnostic Imaging Use in Children’s Hospitals to Prioritize Stewardship Efforts
Megan Collins, Matt Hall, John R. Stephens, and Jessica Markham
Background: Healthcare waste, including overuse of treatments or testing such as unnecessary diagnostic imaging, has estimated annual costs of over $760 billion in the United States. The most prevalent and costly imaging studies among hospitalized children are not known. Objective: To describe diagnostic imaging studies among hospitalized children with the highest prevalence, cost, rates of repetition, and hospital variation to help inform de-implementation efforts. Design/Methods: We performed a retrospective cohort study of children <18 years of age hospitalized from 1>/1/2021 to 12/31/2022 across 45 hospitals in the Pediatric Health Information System. We identified all radiologic imaging for inpatient and observation encounters using billing codes. We grouped images by modality and body location, and excluded images classified as other/unspecified body location. The intraclass correlation coefficient was used to measure variation across hospitals in imaging use after adjusting for age and severity. Higher numbers indicate a higher degree of variation. Results: We identified 1,523,343 encounters; 59.1% had diagnostic imaging (Table 1). The most prevalent diagnostic imaging studies were chest x-ray (XR), abdominal XR, and echocardiogram. The images most frequently repeated were chest XR, echocardiogram, and abdominal XR. The costliest individual diagnostic imaging studies were echocardiogram, chest XR, and head/brain MRI (Table 2). Although chest XR was among the least expensive imaging modalities per unit cost, given the high prevalence of use and repeat use it was one of the costliest tests overall. Head US, interventional XR, and abdominal US had the highest variability of use between hospitals (Table 2, Figure). Conclusion(s): Chest XR and echocardiograms were among the most prevalent, costly, and frequently repeated imaging studies. Abdominal XR, abdominal ultrasound, bone/joint XR, head/brain CT, and head/brain MRI were high in both prevalence and cost among hospitalized children. Five of the 10 most commonly used imaging techniques and four of the 10 most commonly repeated imaging techniques expose children to ionizing radiation. These results could help identify areas that should be targeted to reduce radiation exposure, improve care, and decrease costs for hospitalized children.
-

Anesthetic and Multidisciplinary Management of a 2-staged Liver Transplant
Kasey Brooks, Lisa Conley, and Brandon Layton
We present a case of a 2 staged liver transplant on a 12-month-old 8kg male with newly diagnosed mitochondrial depletion syndrome causing acute liver failure, refractory lactic acidosis, and cardiopulmonary collapse requiring ECMO. The patient’s past medical history at the time of presentation included history of prematurity at 32 weeks, developmental delay, and a brother with an undiagnosed pancreatic disorder. The patient was brought in by parents to the emergency department with a cough, minimal PO intake for 5 days, and increased fatigue who was found to be URI positive. Initial labs were concerning for anemia, elevated bilirubin, elevated AST/ALT, hyponatremia, coagulopathy, and metabolic acidosis secondary to an elevated lactate of 11.5 mmol/L. An ultrasound of the liver showed hepatocellular inflammation with small perihepatic and pericholecystic fluid. He was admitted to the floor for observation and continued testing. 4 days after admission he had an acute decompensation due to fulminant liver failure and persistent severe lactic acidosis requiring intubation, resuscitation, and VA ECMO support. The leading diagnosis was that he had an inborn error of metabolism causing liver necrosis. Whole exome sequencing was performed to better delineate the cause of his persistent lactic acidosis and liver failure. Due to the dire nature of the patient's medical course, a multidisciplinary meeting was held and he was listed status 1A for a liver transplant due to a necrotic liver. The operative plan was for the transplant surgery team to perform a hepatectomy with return to the ICU post operatively to allow improvement in his physiology and for his lactic acidosis to correct itself and then receive a whole liver transplant the following day. The patient remained intubated and sedated and was taken to the operating room with the OR nursing staff, PICU team, ECMO staff, CRRT nurse, anesthesia team, and surgical team. He was then terminally extubated 2 months after his initial presentation.
-

An Increased Failure Rate of Asparaginase Desensitization with Calaspargase Pegol
Jillian Fry, Erin M. Guest, and Keith J. August
Background: In late 2022, pegaspargase (SS-PEG) became unavailable to patients younger than 22 years in the United States, leaving calaspargase pegol (SC-PEG) as the only available long-acting asparaginase formulation. SC-PEG has been compared to SS-PEG in two randomized, pediatric clinical trials and found to have similar rates of adverse events with comparable rates of event-free survival. Our institution uses a desensitization protocol for patients who experience a hypersensitivity reaction to asparaginase. Here we review our experience with desensitization since the transition to SC-PEG from SS-PEG. Objectives: To compare the rate of hypersensitivity reactions, success of desensitization protocols, and need for alternative asparaginase preparations between patients receiving SC-PEG and SS-PEG at our institution. Design/Method: This is a retrospective, single center study of pediatric patients who received at least 2 doses of SC-PEG between November 2022 and December 2023. Results: We report on 26 patients with acute lymphoblastic leukemia and lymphoblastic lymphoma who received at least two doses of SC-PEG. The frequency of a grade 2 or higher clinical hypersensitivity reaction in those who received SC-PEG was 42.3% (n=11). Silent inactivation, defined as serum asparaginase activity (SAA) <0.1 IU/mL measured seven days following dosing, occurred in an additional 7.8% (n=2). Ten patients underwent SC-PEG desensitization using a protocol that was identical to our previously published protocol using SS-PEG (August, et al., Ped Blood Cancer, 2020). In the desensitization protocol, patients were premedicated with prednisone, cetirizine, famotidine, and montelukast. SC-PEG 2500 IU/m2 was divided into three fractions of 1:100, 1:10, and 1:1 dilution. Each fraction was infused over approximately 60 minutes, increasing the rate every 15 minutes. Desensitization was tolerated with appropriate SAA levels (0.1 IU/mL) in 30% (n=3) of patients, 60% tolerated the infusion but had inappropriately low AA levels (n=6), and one patient did not complete the infusion due to an adverse event. Six patients received Rylaze following SC-PEG hypersensitivity, silent inactivation, or unsuccessful desensitization. Compared to our prior experience with SS-PEG desensitization where 17 out of 21 attempts were successful with appropriate SAA levels (August, et al., ASH, 2022), our success rate using SC-PEG (7 failures out of 10 attempts) is significantly less (p=0.013), leading to an increase in the use of an alternative asparaginase preparation. Conclusion: Our single institution experience with SC-PEG shows a high rate of hypersensitivity reactions, a high likelihood of failure of asparaginase desensitization compared to our historical experience, and the frequent need to switch to an alternative asparaginase preparation.
-

Congenital Heart Defects and Autism: Understanding the Breakdown of Associated Risk Factors In A Clinically Referred Sample
Elizabeth Raines, Amanda Strasser, Amanda Manderfeld, Paul Glasier, and Elizabeth J. Willen
Background: Children with Congenital Heart Disease (CHD) have higher odds of developing social difficulties and/or an Autism Spectrum Disorder (AuSD) than the general population (i.e., ~10% vs. ~1%). However, there is a paucity of nuanced understanding of specific drivers of the increased rates of AuSD in extant literature. The purpose of this study is to identify the rates of co-occurring cardiac, neurological, and genetic conditions to better understand associated risk factors in a patient sample from a medium-size children’s hospital. Methods: Our population includes a clinically referred sample of children (i.e., medical history of CHD and neurodevelopmental risk) under 18 who received a diagnosis of AuSD through neuropsychological evaluation at Children’s Mercy Kansas City (CMKC) between 01/2021 and 12/2022 (N = 356 total sample; N = 50 AuSD). Results: Analyses explored rates of co-occurring cardiac, neurological, and genetic conditions among children with AuSD (10.39% of the overall CHD sample). In this sample of children with CHD and AuSD, the following prevalence rates represent the largest categories of cardiac, neurological, and genetic comorbidities, respectively: 1) Ventral Septal Defect (VSD) (24%), 2) abnormal imaging/ECMO (12%), and 3) genetic variant of unknown significance and 22q11.2 deletion (both 4%). Additional rates of AuSD and specific co-occurring conditions will be presented in detail. Conclusion: Increased recognition of the higher risk of AuSD in the CHD population is emerging. Understanding the rates of different types of co-occurring cardiac, neurological, and genetic conditions will further improve patient centered care. It is imperative that providers include regular AuSD screening in clinics to ensure appropriate access to evaluation, treatment, and family support.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}