
These posters have been presented at meetings in Children's Mercy and around the world. They represent research that was done at the time they were created, and may not represent medical knowledge or practice as it exists at the time viewers access these posters.
-

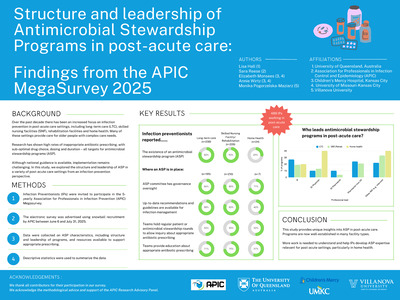
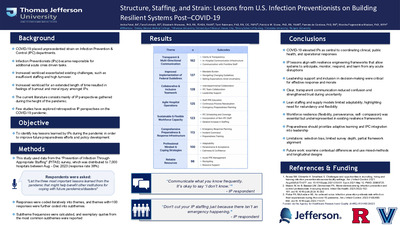
Structure, Staffing, and Strain: Lessons from U.S. Infection Preventionists on Building Resilient Systems Post–COVID-19
Anika Patel, Tara Schmidt, Elizabeth Monsees, Terri Rebmann, Patricia W. Stone, Pamela de Cordova, and Monika Pogorzelska-Maziarz
-

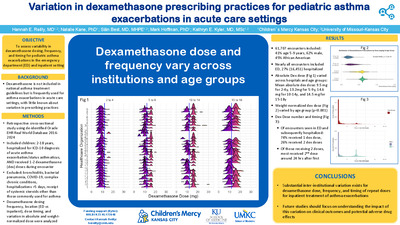
Variation in dexamethasone prescribing practices for pediatric asthma exacerbations in acute care settings
Hannah Reilly, Natalie J. Kane, Sian Best, Mark A. Hoffman, and Kathryn Kyler
-

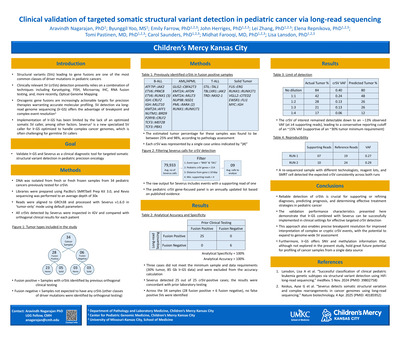
Clinical validation of targeted somatic structural variant detection in pediatric cancer via long-read sequencing
Aravindh Nagarajan, Byunggil Yoo, Emily Farrow, John Herriges, Lei Zhang, Elena Repnikova, Tomi Pastinen, Carol J. Saunders, Midhat Farooqi, and Lisa Lansdon
Introduction: Structural variants (SVs) leading to gene fusions are one of the most common classes of driver mutations in pediatric cancer. Clinical SV detection relies on a combination of techniques including karyotyping, FISH, microarray and RNA fusion testing, and, more recently, optical genome mapping. SV detection via long-read genome sequencing (lr-GS) offers the advantage of breakpoint and complex event resolution; however, its implementation has been limited by the lack of an optimized somatic SV caller, among other factors. Here we describe the clinical validation of lr-GS for targeted somatic SV detection in pediatric cancer using Severus, a newly available somatic SV caller for lr-GS. Methods: DNA was isolated from fresh or fresh frozen samples from 34 pediatric cancers (26 heme and 8 solid) previously tested clinically for SVs, 28 of which were positive for clinically relevant (i.e., oncogenic) SVs (crSVs) expected to result in a gene fusion. The estimated tumor content for these cases, per pathology review, was 25-98%. Briefly, libraries were prepared using PacBio’s SMRTbell Prep Kit 3.0, and Revio sequencing was performed to an average depth of 30x. Reads were aligned to GRCh38 and processed with Severus v1.6.0 in ‘tumor-only’ mode. Data filtering parameters included a pediatric crSV gene-focused panel , a minimum supporting read count of 4, and the location of the breakpoint relative to the nearest gene. All crSVs detected by Severus were inspected in IGV and compared with orthogonal clinical results for each patient. To establish the assay’s limit of detection, DNA from a neoplastic sample with a crSV was diluted at different ratios with DNA from the same patient’s germline sample. Assay precision was assessed by sequencing the same sample with a crSV across two different runs performed on different days. All resulting data was analyzed as above. Results: Severus detected 25 out of 25 crSV-positive cases that were above the limit of detection established for this assay (30% tumor); the results were concordant with prior laboratory testing, leading to an accuracy of 100%. In some cases, the breakpoint resolution offered by lr-GS identified additional rearrangement complexity that helped clarify orthogonal test results. Across the 34 samples (28 positive + 6 negative), no false positive SVs were identified, yielding an analytical specificity of 100%. In the dilution sample (84% tumor), the SV remained detectable down to an ∼13% observed VAF, leading to a conservative reporting cutoff at ~15% VAF (supportive of the 30% tumor minimum requirement). The assay demonstrated 100% precision, as a re-sequenced sample processed with different technologists, reagent lots, and SMRT cell detected the expected crSV consistently across both runs. Conclusion: Reliable detection of crSVs is crucial for supporting or refining diagnoses, predicting the prognosis, and determining effective treatment strategies for pediatric cancer. The validation performance characteristics presented here demonstrate that Severus can be successfully implemented in clinical settings for effective targeted crSV detection. This approach also enables precise breakpoint resolution for improved interpretation of complex or cryptic crSV events, with the potential to expand from a targeted assay to a genome-wide SV assessment tool. Furthermore, lr-GS offers the benefits of SNV and methylation information that, although not explored in the present study, hold great future potential for additional profiling of these samples from a single data source.
-

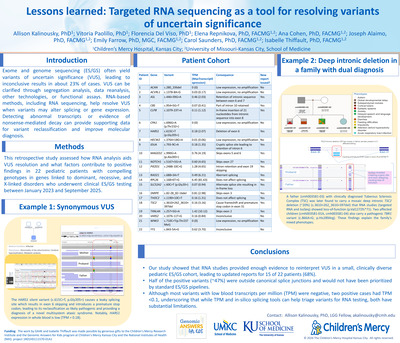
Lessons learned: Targeted RNA sequencing as a tool for resolving variants of uncertain significance
Allison Kalinousky, Vitoria Paolillo, Florencia Del Viso, Elena Repnikova, Ana S A Cohen, Joseph Alaimo, Emily Farrow, Carol J. Saunders, and Isabelle Thiffault
Our study demonstrated the utility of RNA studies in providing sufficient evidence to reinterpret VUS in a small cohort of clinically diverse pediatric patients who received ES/GS-based testing. Fifteen patients (68%) received an updated clinical report. Notably, in 59% the RNAseq data resulted in a molecular diagnosis. Moreover, ~47% of our positive variants were not located at splicing junctions, and therefore, would most likely not be flagged as a likely candidate in ES/GS analysis pipelines. While most variants with low TPM in blood failed, two positive variants had TPM less than 0.1, indicating that while TPM values can help narrow down which variants could be reflexed to targeted RNAseq, these values and in silico splicing predictions have significant limitations. As the cost of sequencing continues to decrease, findings of this diagnostic study demonstrate that the ability to perform targeted RNAseq concurrently with DNA sequencing represents an important advancement in genetic testing by improving classification of variants, therefore, improving the diagnostic yield.
-

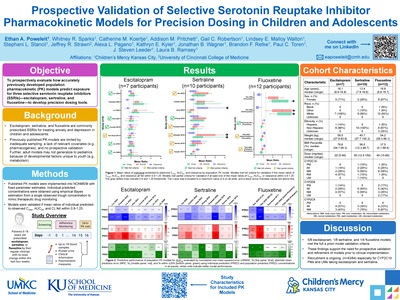
Prospective Validation Of Selective Serotonin Reuptake Inhibitor Pharmacokinetic Models For Precision Dosing In Children And Adolescents
Ethan A. Poweleit; Whitney Sparks MS; Catherine Koertje; Addison Pritchett MS; Gail Robertson; Lindsey Malloy-Walton; Stephani Stancil; Jeffrey R. Strawn; Alexa L. Pagano; Kathryn Kyler; Jonathan B. Wagner; Brandon Retke; Paul C. Toren; J Steven Leeder PharmD, PhD; and Laura B. Ramsey
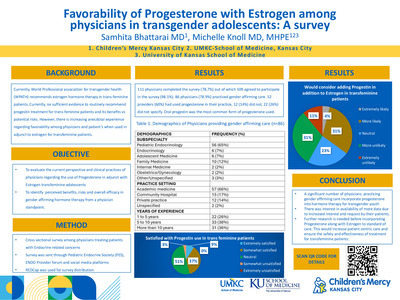
Background: Selective serotonin reuptake inhibitors (SSRIs) are commonly prescribed to children and adolescents with anxiety and depression. However, their clinical use is complicated by marked interindividual variability in exposure, which contributes to differences in treatment response and side effects. Further, SSRIs are commonly dosed using a trial-and-error approach. Model-informed precision dosing could improve treatment outcomes, yet existing SSRI population pharmacokinetic (PK) models have not been prospectively validated and may not generalize to pediatric patients. This study aims to evaluate how accurately these models predict exposure for three SSRIs—escitalopram (ESC), sertraline (SRT), and fluoxetine (FLX)—and refine them to develop tools for dose individualization. Methods: This is an open-label prospective study with dense PK sampling in participants (6-18 years old) prescribed ESC, SRT, or FLX at steady state. Following two weeks of adherence monitoring, participants complete a 24-hour PK study visit where ≤18 blood samples are collected across the dosing interval to measure SSRI plasma concentrations by liquid chromatography mass spectrometry. Published models are implemented into NONMEM to generate individual predicted concentrations from observed trough concentrations to mimic therapeutic drug monitoring. The models are considered validated if the mean ratios of predicted-to-observed Cmax, AUC24, and clearance were within 0.8-1.25. Results: A total of 8 ESC, 8 SRT, and 3 FLX/norfluoxetine (NFLX) models were included for validation. There were 4 ESC, 2 SRT, and 11 FLX/NFLX participants with measured concentrations from interim analysis. Model validation showed 5/8 (63%) of ESC, 0/8 of SRT, and 1/3 (33%) FLX/NFLX models (both parent and metabolite) met full acceptance criteria for all three endpoints, with some models meeting partial acceptance criteria (Figure). Conclusions: Prospective external validation shows several models met the a priori validation criteria for the ESC and FLX/NFLX cohorts. Additional participants in each drug cohort are needed to verify the models are fit for purpose. These findings provide a foundation for future model refinement and suggest that model-informed precision dosing could reduce trial-and-error prescribing and improve SSRI tolerability and efficacy in youth.
-

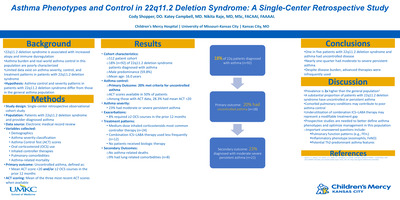
Asthma Phenotypes and Control in 22q11.2 Deletion Syndrome: A Single-Center Retrospective Study
Cody Shopper, Katey Campbell, and Nikita S. Raje
Background: Patients with 22q11.2 deletion syndrome have increased rates of atopy and immune dysregulation and may experience a higher burden of asthma; however, real-world data describing asthma control, severity, and treatment patterns in this population are limited. We hypothesized that asthma control and severity patterns in patients with 22q11.2 deletion syndrome differ from those observed in the general asthma population. Objectives/Goal: To characterize asthma control, severity, and treatment patterns among patients with 22q11.2 deletion syndrome and to compare observed patterns with those typically reported in the general asthma population. Methods/Design: We conducted a retrospective observational cohort study of patients with 22q11.2 deletion syndrome and a provider-diagnosed history of asthma at a single tertiary care center. Data was extracted from electronic medical records and included demographics, asthma severity classification, Asthma Control Test (ACT) scores, oral corticosteroid (OCS) use, inhaled controller therapies, comorbid pulmonary conditions, hospitalizations, biologic therapy use, and asthma-related mortality. The primary outcome was asthma control, defined as a mean ACT score < 20 and/or receipt of two or more OCS courses in the preceding 12 months. When available, the three most recent ACT scores were averaged from the most recent assessment. Results: Of our 512 patient cohort, 92 patients (18%) with 22q11.2 deletion syndrome were diagnosed with asthma. Overall, 20% met criteria for uncontrolled asthma at their most recent evaluation. Among the cohort, 23% had moderate or severe persistent asthma. Eight percent required two or more courses of oral corticosteroids in the prior 12 months. ACT scores were available for 50% of patients; among those with documented ACT data, 28.3% had a mean ACT score < 20. Patients were more frequently treated with medium-dose inhaled corticosteroids alone (n=24) compared with combination inhaled corticosteroid–long-acting beta agonist (ICS–LABA) therapy (n=12). No patients received biologic therapy, and there were no asthma-related deaths. Conclusions: In this single-center cohort of patients with 22q11.2 deletion syndrome, nearly one in five were diagnosed with asthma. Further, one in five individuals with asthma demonstrated uncontrolled disease, and nearly one-quarter had moderate to severe persistent asthma. Despite this, combination ICS–LABA therapy and biologic agents were infrequently utilized. These findings suggest a potential treatment gap and raise important questions regarding asthma phenotype, pulmonary comorbidities, and optimal controller strategies in this population. Future prospective studies incorporating pulmonary function testing, inflammatory biomarkers, and standardized asthma assessments are needed to better characterize disease mechanisms and improve asthma outcomes in patients with 22q11.2 deletion syndrome.
-

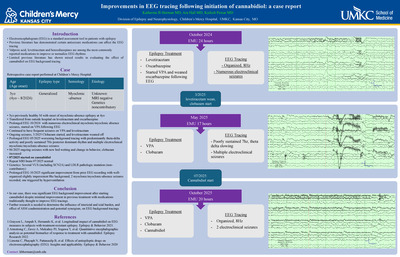
Improvements in EEG tracing following initiation of cannabidiol: a case report
Katherine Horman, Ara Hall, and Kailash Pawar
-

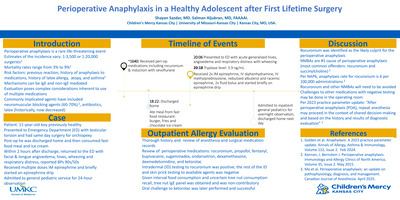
Perioperative anaphylaxis in a healthy adolescent after first lifetime surgery
Shayan Sazdar and Salman Aljubran
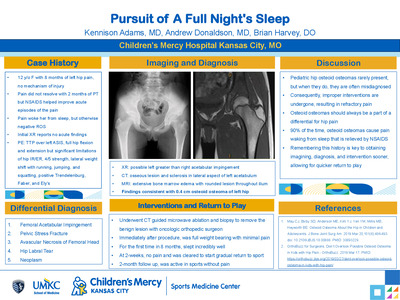
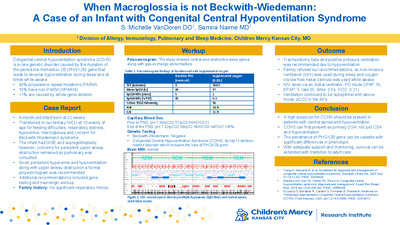
Introduction: Perioperative anaphylaxis is a rare life-threatening event. Its evaluation poses complex considerations inherent to the use of multiple medications. Patient presentation: A healthy 11-year-old boy developed anaphylaxis shortly after discharge home from first lifetime surgery for orchiopexy. Perioperative medications included rocuronium, propofol, fentanyl, bupivacaine, sugammadex, ondansetron, dexamethasone, dexmedetomidine, and ketorolac. No antibiotics. After surgery, he consumed fast food dinner and ice cream. Within 2 hours after discharge home, he returned to our Emergency Department (ED) with facial and tongue angioedema, hives, and respiratory distress. He received multiple doses of intramuscular epinephrine and briefly required epinephrine drip in the ED. Tryptase was 3.9. He was admitted to the general pediatric service for 24-hour observation. Due to uncertain recall of general tree nut consumption, tree nut panel was obtained which was non-contributory. He had skin prick and intradermal (ID) testing to all suspected medications used intraoperatively except for ketorolac and dexmedetomidine. ID testing was positive for rocuronium, otherwise negative. Since his event, he tolerated ibuprofen, acetaminophen, methylprednisolone and ondansetron. Additionally, he passed in clinic challenge to oral ketorolac. Discussion: In perioperative anaphylaxis, the most common offending agents are antibiotics and neuromuscular blocking agents (NMBAs). With positive intradermal testing, rocuronium is the most suspected agent for this patient and will need to be avoided along with other NMBAs. Challenges to other medications with negative testing were recommended to be done in the operating room. Patient outcomes: This case highlights the importance of careful review of history and appropriate medication skin testing in evaluating perioperative anaphylaxis.
-

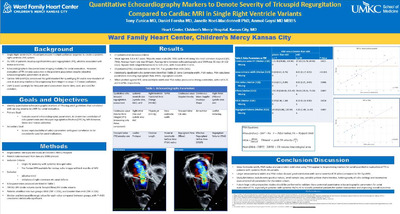
Quantitative Echocardiography Markers to Denote Severity of Tricuspid Regurgitation Compared to Cardiac MRI in Single Right Ventricle Variants
Tony Zunica, Daniel Forsha, Janelle Noel-Macdonnell, and Anmol Goyal
Background: Single right ventricle and Hypoplastic Left Heart Syndrome (HLHS) are congenital heart diseases that require multiple palliative surgeries to create a single right ventricular system. 25-30% of these patients develop significant tricuspid regurgitation (TR), which is associated with worse outcomes among all stages of palliation. Echocardiography remains the cornerstone imaging modality for serial evaluation in these patients. However, estimating tricuspid regurgitation is highly subjective in the pediatric population, necessitating need for reliable and reproducible quantitative echocardiography markers. Currently, cardiac magnetic resonance (CMR) is considered the gold standard for quantification of tricuspid regurgitation with good accuracy and reproducibility. Objectives/Goal: Our primary aim was to identify quantitative markers of determining TR severity using echocardiography that correlated with CMR between the final two palliative stages. Methods/Design: This was a single-center, retrospective study performed at Children’s Mercy Hospital. Inclusion criteria included patients with single systemic right ventricle with a systemic tricuspid valve who have undergone an echocardiogram within 6 months of their CMR. All other congenital heart diseases were excluded. Patient characteristics included age, sex, body surface area, diagnosis, heart rate with echocardiography and CMR and time between echocardiography and CMR. Multiple echocardiographic variables were recorded including but not limited to Nyquist limit, TR continuous wave doppler density, shape and volume time integral (VTI), vena contract width, jet number, proximal isovelocity surface (PISA) radius, leaflet morphology and right ventricular functional indices. Tricuspid valve regurgitation fraction (TRF) by CMR was recorded and categorized as mild (≤15%) or greater than mild (>15%). Each quantitative echocardiographic variable was correlated with the two groups as estimated by CMR. P value < 0.05 was considered statistically significant. Results: 27 patients met inclusion criteria. Mean age was 3.8 ± 0.7 years. Majority were male (20, 74%) with HLHS being the most common diagnosis (21, 78%). Average heart rate was 89 bpm. Average time between echocardiography and CMR was 31 days (0-112 days). Nyquist limit ranged between 42 to 123 cm/s, with mean of 82.4 cm/s. 20 patients (74%) were characterized as mild based on CMR TRF. Vena contracta width (0.61-0.76 for greater than mild vs 0.17-0.35 for mild, p< 0.001), TR continuous wave VTI (76.8-143.9 for greater than mild vs 15.7-69.3 for mild, p = 0.021) and PISA radius (0.51-0.89 for greater than mild vs 0.21-0.40 for mild, p = 0.006) were statistically significantly higher in the greater than mild category. Calculated indices such as effective regurgitation orifice area and regurgitation volume were statistically significantly higher in greater than mild category (p=0.016 and 0.007, respectively). Conclusions: Although sample size is small, our study highlights echocardiographic markers such as vena contracta width, PISA radius, and associated calculated indices that can potentially be used to better estimate severity of TR in HLHS variants. Future large-scale studies are needed to further evaluate this correlation, which may lead to more objective methods of estimating TR using echocardiography, leading to improved management decisions and outcomes.
-
 by Abbey Elsbernd, N Grills, J Antoon, Kathryn Kyler, L Orth, T Savage, M Hall, Jennifer Goldman, and Shannon Carpenter")
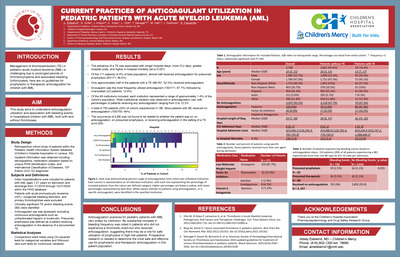
Current practices of anticoagulant utilization in pediatric patients with acute myeloid leukemia (AML)
Abbey Elsbernd, N Grills, J Antoon, Kathryn Kyler, L Orth, T Savage, M Hall, Jennifer Goldman, and Shannon Carpenter
-
 and bleeding disorders in infants referred to pediatric hematology by Abbey Elsbernd, Lyndsey Hultman, and James Anderst")
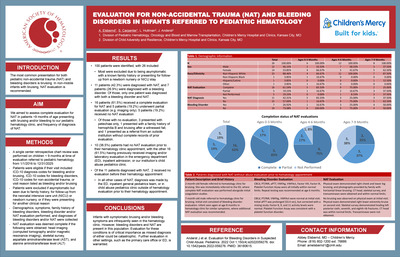
Evaluation for non-accidental trauma (NAT) and bleeding disorders in infants referred to pediatric hematology
Abbey Elsbernd, Lyndsey Hultman, and James Anderst
-

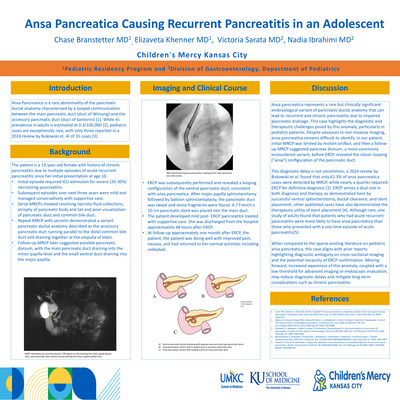
A Case Report: Ansa Pancreatica as a Cause of Recurrent Pancreatitis
Chase Branstetter, Elizaveta Khenner, Victoria Sarata, and Nadia Ibrahimi
-

A Rare Case of Ogilvie’s Syndrome in a Pediatric Patient with a Complex Medical History
Kirby Lampe, Victoria Sarata, and Aileen Har
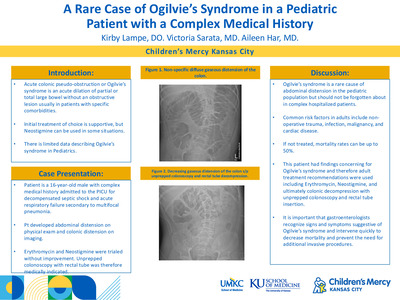
Acute colonic pseudo-obstruction (ACPO) or Ogilvie’s syndrome is an acute dilatation of the small or large bowel without an obstructive lesion. Symptoms include abdominal distension, nausea and vomiting, constipation and occasional dyspnea. The disorder most commonly involves the cecum and right colon and is most frequently seen in male patients above the age of 60 (1). It is rare for Ogilvie’s to occur in the pediatric population though some infrequent instances have been reported. Here, we report a case of a patient with significant abdominal distension and gaseous distension seen on x-ray, which was diagnosed and treated as Ogilvie’s syndrome. He was unresponsive to conservative and medical management and ultimately required endoscopic decompression.
-

Intravenous sotalol in pediatric cardiac intensive care patients compared to other antiarrhythmics: insights from a multicenter database
Rohit S. Loomba, Emily R. Backes, Juan Farias Torres, Alejandro Borquez, Lindsey Malloy-Walton, and Saul Flores
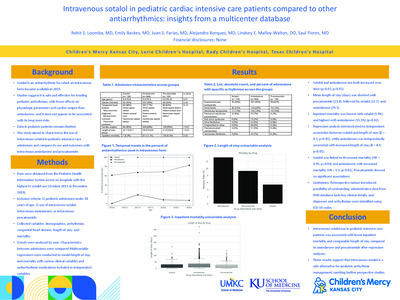
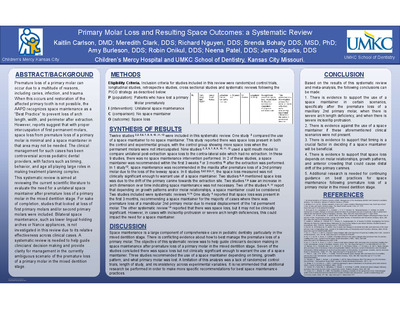
Background: Sotalol is an antiarrhythmic for which an intravenous (IV) form became available in 2015. Studies suggest it is safe and effective for treating pediatric arrhythmias, with fewer effects on physiologic parameters and cardiac output than amiodarone, and it does not appear to be associated with its long-term risks. However, data in pediatric patients remains limited. This study aimed to characterize the use of intravenous sotalol in pediatric intensive care admissions and compare its use and outcomes with intravenous amiodarone and procainamide. Methods: Data were drawn from the Pediatric Health Information System across six hospitals with the highest IV sotalol use (October 2015 to December 2019). Included were admissions of pediatric patients who received intravenous sotalol, amiodarone, or procainamide. Collected variables included demographics, arrhythmias, congenital heart disease, length of stay, and mortality. Trends were analyzed by year. Multivariable regressions were conducted to model length of stay and mortality with various clinical variables and antiarrhythmic medications included as independent variables. Results: Of 927 admissions, 128 (14%) received sotalol, 660 (71%) amiodarone, and 139 (15%) procainamide. Cardiac surgery was least common in the sotalol group (p< 0.01). Sotalol and amiodarone use both increased over time (p=0.03 and p< 0.01) (Figure 1). Supraventricular tachycardia was the most common arrhythmia (Table 1). Mean length of stay (days) was shortest with procainamide (21.8), followed by sotalol (22.7), and amiodarone (29.5) (Figure 2). Inpatient mortality was lowest with sotalol (5.4%) and highest with amiodarone (13.1%) (p=0.02) (Figure 3). Regression analysis demonstrated no independent association between sotalol and length of stay (β = -0.2, p=0.83), while amiodarone was independently associated with increased length of stay (β = 8.4, p< 0.01). Sotalol was linked to decreased mortality (OR = 0.95, p=0.04) and amiodarone with increased mortality (OR = 1.1, p< 0.01). Procainamide showed no significant associations. Conclusion: Intravenous sotalol use in pediatric intensive care patients was associated with lower inpatient mortality and comparable length of stay compared to amiodarone and procainamide after regression analyses. These results support that intravenous sotalol is a safe alternative for pediatric arrhythmia management, meriting further prospective studies.
-

Juvenile Polyp and Lymphoid Hyperplasia “Leads” to Intussusception
Rasheed Ansari, Kirby Lampe, and Ding-You Li
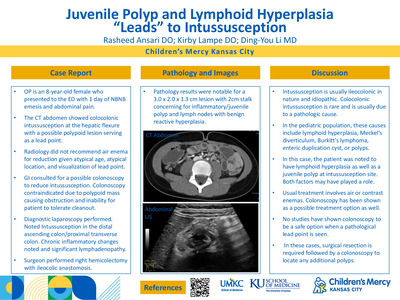
OP is an 8-year-old female who presented to the ED with 1 day of NBNB emesis and abdominal pain. • The CT abdomen showed colocolonic intussusception at the hepatic flexure with a possible polypoid lesion serving as a lead point. • Radiology did not recommend air enema for reduction given atypical age, atypical location, and visualization of lead point. • GI consulted for a possible colonoscopy to reduce intussusception. Colonoscopy contraindicated due to polypoid mass causing obstruction and inability for patient to tolerate cleanout. • Diagnostic laparoscopy performed. Noted Intussusception in the distal ascending colon/proximal transverse colon. Chronic inflammatory changes noted and significant lymphadenopathy. • Surgeon performed right hemicolectomy with ileocolic anastomosis. OP is an 8-year-old female who presented to the ED with 1 day of NBNB emesis and abdominal pain. • The CT abdomen showed colocolonic intussusception at the hepatic flexure with a possible polypoid lesion serving as a lead point. • Radiology did not recommend air enema for reduction given atypical age, atypical location, and visualization of lead point. • GI consulted for a possible colonoscopy to reduce intussusception. Colonoscopy contraindicated due to polypoid mass causing obstruction and inability for patient to tolerate cleanout. • Diagnostic laparoscopy performed. Noted Intussusception in the distal ascending colon/proximal transverse colon. Chronic inflammatory changes noted and significant lymphadenopathy. • Surgeon performed right hemicolectomy with ileocolic anastomosis.
-

Refractory Benign Esophageal Strictures Complicated by Esophageal Perforation and Treated with Serial Dilations and Stent Placement in a Pediatric Patient
Kirby Lampe, Victoria Sarata, and Nadia Ibrahimi
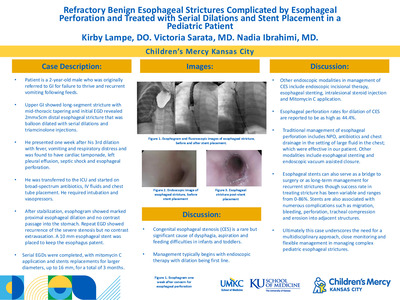
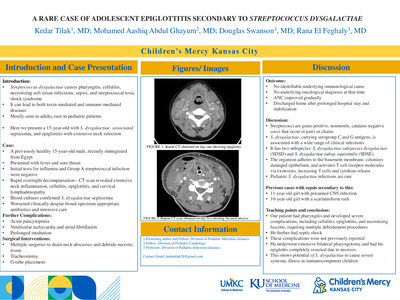
Patient is a 2-year-old male who was originally referred to GI for failure to thrive and recurrent vomiting following feeds. Upper GI showed long-segment stricture with mid-thoracic tapering and initial EGD revealed 2mmx5cm distal esophageal stricture that was balloon dilated with serial dilations and triamcinolone injections. He presented one week after his 3rd dilation with fever, vomiting and respiratory distress and was found to have cardiac tamponade, left pleural effusion, septic shock and esophageal perforation. He was transferred to the ICU and started on broad-spectrum antibiotics, IV fluids and chest tube placement. He required intubation and vasopressors. After stabilization, esophogram showed marked proximal esophageal dilation and no contrast passage into the stomach. Repeat EGD showed recurrence of the severe stenosis but no contrast extravasation. A 10 mm esophageal stent was placed to keep the esophagus patent. Serial EGDs were completed, with mitomycin C application and stents replacements for larger diameters, up to 16 mm, for a total of 3 months. Congenital esophageal stenosis (CES) is a rare but significant cause of dysphagia, aspiration and feeding difficulties in infants and toddlers. Management typically begins with endoscopic therapy with dilation being first line. Other endoscopic modalities in management of CES include endoscopic incisional therapy, esophageal stenting, intralesional steroid injection and Mitomycin C application. Esophageal perforation rates for dilation of CES are reported to be as high as 44.4%. Traditional management of esophageal perforation includes NPO, antibiotics and chest drainage in the setting of large fluid in the chest; which were effective in our patient. Other modalities include esophageal stenting and endoscopic vacuum assisted closure. Esophageal stents can also serve as a bridge to surgery or as long-term management for recurrent strictures though success rate in treating stricture has been variable and ranges from 0-86%. Stents are also associated with numerous complications such as migration, bleeding, perforation, tracheal compression and erosion into adjacent structures. Ultimately this case underscores the need for a multidisciplinary approach, close monitoring and flexible management in managing complex pediatric esophageal strictures.
-

Symptomatic Severe Hyponatremia: A Rare Complication of Double Balloon Enteroscopy
Victoria Sarata, Kirby Lampe, and Thomas M. Attard
Previously healthy 11-year-old female, newly diagnosed Peutz-Jeghers Syndrome (PJS) confirmed by genetic testing STK11 PV (c.464+1dupG) underwent double balloon enteroscopy (DBE) after small bowel capsule showed multiple small intestinal polyps including >1.5 cms diameter. Pre-procedure, she completed a two-day MiraLAX clean out with >10 x 17g doses of MiraLAX each mixed in 6-8oz of water and other clear liquids. DBE completed with resection of 17 total small intestinal (SI), jejunal and ileal polyps. Procedure lasted approximately 4hrs and 5L of sterile water was used for underwater technique and irrigation.Sterile water was used for copious irrigation needed for direct visualization, and increased buoyancy of SI polyps in compliance with scope manufacturer recommendations (IFU). Patient was admitted secondary to number and size of polyps removed. Six hours post-procedure patient had hematemesis followed by a generalized tonic-clonic seizure. Abortive medications given and severe hyponatremia noted with serum sodium of 119mEq/L . Patient transferred to the ICU and treated with 3% hypertonic saline and sodium normalized over several hours. Patient discharged home with several stable sodium levels and no neurologic sequelae. This case represents the rare but potentially life- threatening complication of post-endoscopic symptomatic hyponatremia in a previously healthy patient. In adults, this is typically associated with excessive free water intake, older age, or in the context of unknown underlying comorbidities.
-

The Use of Omalizumab For Idiopathic Isolated Angioedema In A Pediatric Patient
Manali Shah and Thao Le
Introduction Angioedema manifests as localized, asymmetric, nonpruritic cutaneous and/or mucosal swelling. The two main clinical forms are histaminergic and bradykinin mediated angioedema. Histaminergic is more common and presents with hives, and responds to antihistamines, steroids, and epinephrine. Bradykinin mediated angioedema lacks hives and does not respond to these therapies. Ten percent of patients with recurrent angioedema have isolated angioedema without urticaria. Case Description A previously healthy 8-year-old male presented initially to the ED evaluation of isolated lip swelling and no other systemic symptoms. There was no exposure to new foods, medications, or illness symptoms. He received anti-histamines and steroids with improvement in his symptoms and referred to Allergy clinic for further evaluation. Lab evaluation with CBCD, BMP, LFTs, inflammatory markers, thyroid studies, ANA, hereditary angioedema, and tryptase were within normal limits. He continued to have recurrent episodes of swelling despite high dose second-generation antihistamines and H2 antagonist. He was started on omalizumab for idiopathic isolated angioedema, with resolution of his symptoms after the second dose. He has been able to stop all anti-histamines without recurrence of symptoms. Discussion This case highlights the off-label use of omalizumab for idiopathic isolated angioedema and demonstrates improvement in symptom control. Isolated angioedema in the absence of urticaria is rare but still warrants a thorough evaluation as management may differ. Isolated angioedema can be difficult to treat as it may not respond to standard therapy. Omalizumab may be effective for these patients and can be considered as a treatment option for recurrent idiopathic isolated angioedema.
-

Unclear Source of Gastrointestinal Bleeding: Utilizing Small Bowel Capsule to Detect an Enteric Duplication Cyst
Victoria Sarata, Kirby Lampe, and Kathryn Clarkston
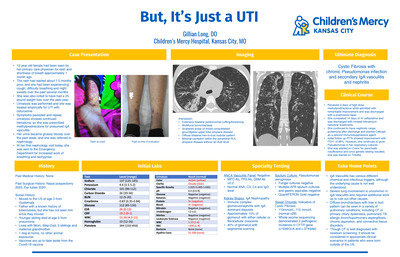
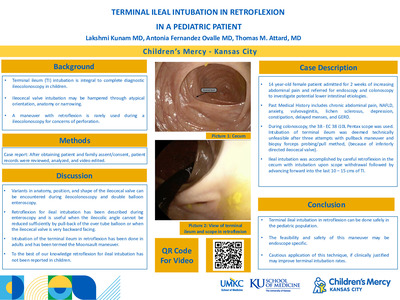
Introduction Enteric duplication cysts (EDCs) are rare congenital malformation formed during embryonic development of the gastrointestinal tract. Symptoms may include vomiting, abdominal distension, palpable abdominal mass, or bleeding but may vary based on location of the lesion [1]. We present a case of a 9-year-old-male with presented with recurrent rectal bleeding and had abnormalities on small bowel capsule which were diagnosed as enteric duplication cyst on exploratory laparoscopy. Case This is a 9 year old male with a history of persistent iron deficiency anemia, gallstones s/p cholecystectomy and recurrent hematochezia. Patient was initially admitted for recurrent red bloody stools and fatigue. His hemoglobin on admission was 8.1. Fecal calprotectin was elevated to 927. Meckel’s scan negative. Esophagogastroduodenoscopy and colonoscopy completed which showed mild superficial chronic gastritis but were otherwise normal. Small bowel capsule was initiated and normal but was not completed. He was discharged home on high dose proton pump inhibitor (PPI) and iron supplement. Hemoglobin on discharge was 8.4 He had follow up with GI about 1 month after this admission. He was doing well with no recurrent bloody stools. Hemoglobin was 12.7. PPI was decreased to once daily. About one month after clinic visit, he was re-admitted for recurrent bloody stools and fatigue. Hemoglobin on admission was 8.7. During this admission, magnetic resonance enterography (MRE) was negative. Nuclear medicine gastrointestinal blood loss imaging was negative with no active bleeding. EGD and colonoscopy repeated and visually normal. No biopsies obtained. Repeat small bowel capsule placed. Hemoglobin on discharge 10.3. Small bowel capsule now showing an area of narrowing, mucosal disruption, and ulceration concerning for a short-segment stricture. There is erythema/mucosal disruption without active bleeding in the distal 1/3 of the small bowel. There is a double lumen appearance with surface ulceration potentially concerning for a Meckel’s diverticulum. There are scattered areas of erythema in the distal small bowel. Dilated lacteals noted in the distal 2/3 of the small bowel. Double balloon enteroscopy vs surgery consult was recommended for further evaluation of these findings. He was again admitted about 1 month later for melena. Hemoglobin 9.6. Exploratory laparoscopy completed and visualized a large conglomeration of hypervascular bowel with small bowel coming in and out of it and adherence to the mesentery proximal to terminal ileum. This was identified as enteric duplication cyst. Patient tolerated the procedure and recovered well. Pathology identified it as benign enteric cystic lesion with mucosal ulceration consistent with an enteric duplication cyst. There was focal presence of oxyntic type gastric mucosa. At surgery follow up visit, he was doing well with stable hemoglobin. Discussion EDCs are congenital malformations of the GI tract that may cause a variety of abdominal symptoms including pain, vomiting, or bleeding. They are typically found in the distal ileum with an incidence of 4500-12500 but may occur anywhere along the GI tract [2]. EDC must have epithelial lining containing the mucosa of the GI tract, an envelope of smooth muscle and an attachment to the GI tract [1]. Most EDCs are diagnosed prenatally but if undetected, they can gradually increase in size and cause worsening obstruction, bleeding or ulceration. Ultrasound is the imaging technique of choice and will show the presence of a cyst with a “double-wall” or “muscular rim” sign. Advanced imaging such as computed tomography (CT) or magnetic resonance can also be used but these are less preferred given cost, radiation exposure or need for sedation. In a study by Okur et al., (2014), out of 32 pediatric cases of EDCs described, 28 were diagnosed with ultrasound and CT was performed in 21 patients [2]. In our case, MRE did not show evidence of an EDC.
-

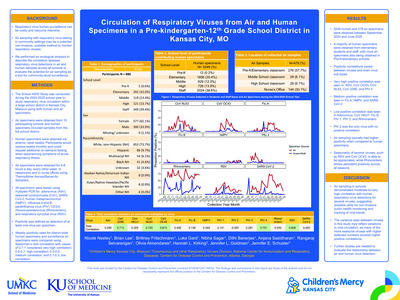
Circulation of Respiratory Viruses from Air and Human Specimens in a Pre-kindergarten-12th Grade School District in Kansas City, MO
Nicole Neeley, Brian Lee, Brittney Fritschmann, Luke Gard, Nibha Sagar, Dithi Banerjee, Anjana Sasidharan, Rangaraj Selvarangan, Olivia Almendares, Hannah L. Kirking, Jennifer Goldman, and Jennifer E. Schuster
Background: Air sampling with respiratory virus testing in community settings may be a potential non-invasive, scalable method to monitor respiratory viruses. We performed an ecological analysis to describe the correlation between respiratory virus detections in air and human samples across all schools to evaluate the potential for air sampling as a tool for community-level surveillance. Methods: Knowledge of Infectious Diseases in Schools (School KIDS) is a voluntary respiratory virus surveillance program in a pre-kindergarten-12th grade public school district in Kansas City, MO. In 10 schools, students and staff collected anterior nasal swabs while at school, with optional on-demand swabbing when experiencing acute respiratory illness. Simultaneously, air samples were collected biweekly using AerosolSense samplers (ThermoFisher Scientific) in 2-4 (total n=32) locations (e.g., classrooms and nurse’s office) per school for 6-8 hours during school. All specimens were tested by multiplex PCR for adenovirus, human metapneumovirus (hMPV), influenza (Flu) A and B, parainfluenza viruses (PIV) 1-4, respiratory syncytial virus (RSV), rhinovirus/enterovirus (RV/EV), SARS-CoV-2, and seasonal coronaviruses ([sCoV] OC43, HKU1, NL63, 229E). Positivity was defined as detection of ≥1 virus. District-wide weekly virus positivity rates from human and air samples were compared using Spearman’s rank correlation. Results: During September 18, 2024–March 31, 2025, 839 participants (Table) submitted 3851 specimens, with 970 (25.2%) testing positive. Of 353 air samples, 312 (88.4%) were positive. Air sample positivity was higher than human specimen positivity in all 22 weeks when both human and air samples were collected (Figure). Strong positive correlations were observed for RSV (0.87), sCoV OC43 (0.87), PIV-4 (0.73); moderate for sCoV NL63 (0.61), Flu A (0.58), and SARS-CoV-2 (0.53); and weak for hMPV (0.29) and RV/EV (0.12). Conclusion: Air sampling in schools demonstrated moderate-to-strong correlation with human respiratory virus detections for several viruses, suggesting possible utility for non-invasive public health monitoring. Further studies are needed to evaluate the relationship between air and human virus detection.
-

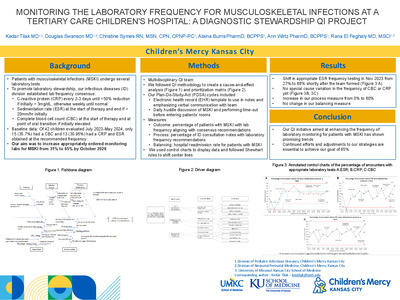
Monitoring The Laboratory Frequency For Musculoskeletal Infections At A Tertiary Care Children's Hospital: A Diagnostic Stewardship Qi Project
Kedar Tilak, Douglas Swanson, Christine Symes, Alaina N. Burns, Ann L. Wirtz, and Rana El Feghaly
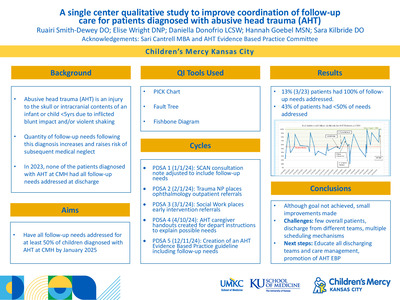
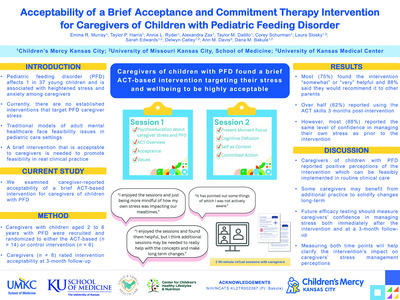
Patients with musculoskeletal infections (MSKI) undergo several laboratory tests. To promote laboratory stewardship, our Infectious diseases (ID) division recommended the following frequencies for labs: 1) C-reactive protein (CRP) every 2-3 days until >50% reduction while >3mg/dL, otherwise weekly until normal, 2) Sedimentation rate (ESR) at the start of therapy and end if > 20mm/hr initially, 3) Complete blood cell count (CBC) at the start of therapy and when transitioning to oral therapy if WBC is initially elevated. Baseline data showed that of 42 children evaluated between July 2023-May 2024, only 15 (35.7%) had a CBC and 13 (30.95%) had a CRP and ESR obtained at the recommended frequency. Our aim was to increase appropriately ordered monitoring labs to 65% by October 2025. Methods We formed a quality improvement team (QI) of ID specialists (fellow, advanced practice provider, pharmacists, physician) and consulted with orthopedics and hospital medicine physicians. We followed QI methodology to create a cause-and-effect analysis (Figure 1) and prioritization matrix (Figure 2). Our Plan-Do-Study-Act (PDSA) cycles included: 1) An electronic health record (EHR) template to use in notes and emphasizing verbal communication with team; 2) Daily huddle discussion of MSKI and performing time-out before entering patients’ rooms. Our outcome measures were the percentage of patients with MSKI having laboratory frequency in accordance with our consensus, our process measure was the percentage of time the laboratory frequency is recommended in the ID consultation note, and our balancing measure was hospital readmission rate for patients with MSKI. We used control charts to display data and followed Shewhart rules to shift center lines. Results We saw a shift in appropriate ESR frequency testing in November 2023 from 27% to 68% shortly after the team formed (Figure 3 A). We have not observed a shift in the frequency of CBC or CRP (Figure 3B, 3C). We saw an increase in our process measure from 0% to 60%. We saw no change in our balancing measure. Conclusion Our QI initiative aimed at enhancing the frequency of laboratory monitoring for patients with MSKI has shown promising trends. Continued efforts and adjustments to our strategies are essential to achieve our goal of 65% by October 2025.
-

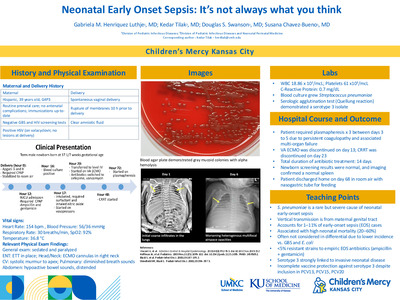
Neonatal Early-Onset Sepsis: It’s Not Always What You Think
Gabriela M. Henriquez, Kedar Tilak, Douglas Swanson, and Susana Chavez-Bueno
-

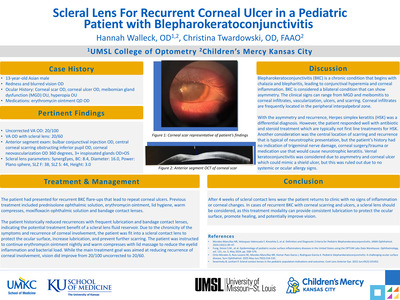
Scleral Lens For Recurrent Corneal Ulcer in a Pediatric Patient with Blepharokeratoconjunctivitis
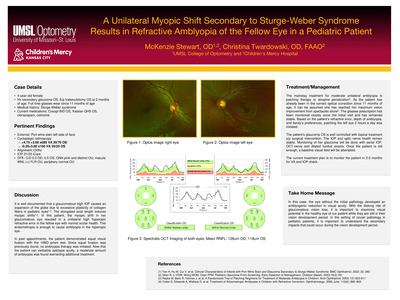
Hannah Walleck and Christina Twardowski
-

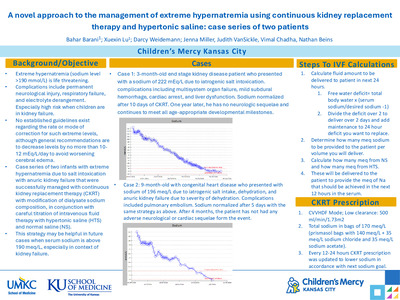
A Novel “Stairstep” Approach to the Management of Extreme Hypernatremia Using Continuous Kidney Replacement Therapy and Hypertonic Saline
Bahar Barani, Xuexin Lu, Darcy Weidemann, Judith Vansickle, Vimal Chadha, and Nathan Beins
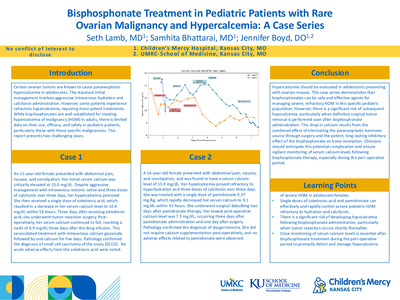
Hypernatremia is defined as a serum sodium greater than 145 mEq/L and is due to either a deficit of free water or excess sodium intake. Extreme hypernatremia (sodium level > 190 mEq/L) is immediately life–threatening with mortality rates > 60%. It is especially challenging to avoid complications, such as permanent neurological injury, respiratory failure, and profound electrolyte derangement, when children are in kidney failure. Established guidelines are lacking for correcting such extreme levels due to a paucity of information in the literature, although general recommendations are to decrease levels by no more than 10-12 mEq/L per day to prevent neurological complications. We report a case series of two infants with extreme hypernatremia due to salt intoxication with anuric kidney failure that were successfully managed with continuous kidney replacement therapy (CKRT) with modification of dialysate sodium composition, in conjunction with careful titration of intravenous fluid therapy. The first case involved a 3-month-old with end stage kidney disease, with home peritoneal dialysis use, presenting with a sodium of 222 mEq/L due to iatrogenic salt intoxication. Complications included multisystem organ failure, subdural hemorrhage, cardiac arrest with subsequent myocardial dysfunction requiring multiple inotropes, respiratory failure, and severe liver dysfunction. Sodium levels normalized over 10 days of “stairstep” CKRT with sodium additives with fine-tuning hypertonic saline and normal saline (See Figure 1). One year later, he has no neurologic sequelae and continues to meet all age-appropriate developmental milestones. The second case was a 9- month-old with congenital heart disease who presented with sodium of 196 mEq/L due to iatrogenic salt intake, severe dehydration, and anuric kidney failure. Complications included pulmonary embolism. Her sodium was corrected after 5 days with the same strategy as above (See Figure 2). At 4-month follow-up, no adverse neurological or cardiac sequelae were noted. Both CKRT prescriptions utilized low clearance of 500 ml/min/1.73m2 and every 12-24 hours CKRT dialysate bags were changed to achieve a sodium reduction of about 10 meq/L per day. In summary, this presents a novel approach to severe hypernatremia in patients with acute or chronic kidney failure through individualized CKRT strategies and judicious fluid therapy.
-

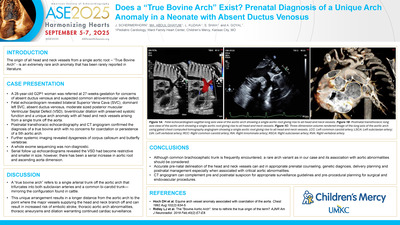
Does a “True Bovine Arch” Exist? Prenatal Diagnosis of a Unique Arch Anomaly in a Neonate with Absent Ductus Venosus
Jenna Schermerhorn, Mohamed Aashiq Abdul Ghayum, Laura Kuzava, Sanket Shah, and Anmol Goyal
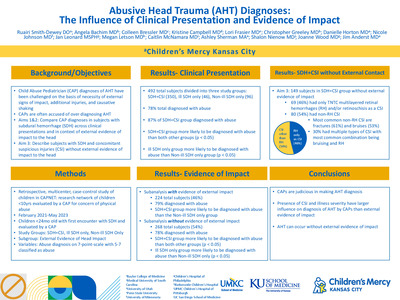
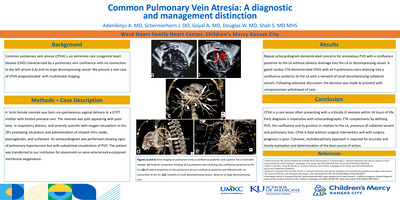
Introduction: The origin of all head and neck vessels from a single aortic root – “True Bovine Arch” - is an extremely rare arch anomaly that has been rarely reported in literature. Clinical Presentation: A 28-year-old G2P1 woman was referred at 27-weeks-gestation for concerns of absent ductus venosus and suspected common atrioventricular valve defect. Fetal echocardiogram revealed bilateral Superior Vena Cava (SVC), dominant left SVC, absent ductus venosus, moderate sized posterior muscular Ventricular Septal Defect (VSD), biventricular dilation with preserved systolic function and a unique arch anomaly with all head and neck vessels arising from a single trunk off the aorta. Postnatal transthoracic echocardiography and CT angiogram confirmed the diagnosis of a true bovine arch with no concerns for coarctation or persistence of a 5th aortic arch. Further systemic imaging revealed dysgenesis of corpus callosum and butterfly vertebrae. A whole exome sequencing was non-diagnostic. Serial follow up echocardiograms revealed the VSD had become restrictive and smaller in size, however, there has been a serial increase in aortic root and ascending aorta dimension. Imaging Findings: Figure 1a shows a sagittal view of the aortic arch with unique branching pattern of all head and neck vessels arising from a single aortic root. Figure 1b and 1c shows post-natal confirmation of the unique aortic arch anomaly via TTE and CTA respectively. Role of Imaging in Patient Care: Accurate prenatal identification of cardiac and aortic arch anomalies is paramount for prenatal counseling, genetic diagnosis, delivery planning and postnatal management. CTA can complement pre and postnatal suspicion for appropriate surgical and endovascular procedural planning. Discussion: The origin of all head and neck vessels from a single aortic root is an extremely rare arch anomaly that has been seldom reported in literature with no documented prenatal identification. A “true bovine arch” refers to a single arterial trunk off the aortic arch that trifurcates into both subclavian arteries and a common bi-carotid trunk—mirroring the configuration found in cattle. Although a common brachiocephalic trunk is considered a normal variant, it has been shown to have a higher likelihood of developing ascending aortic aneurysm and embolic cerebrovascular accidents, a possibility even more likely to happen in our patient with unique arch branching. This could be secondary to hemodynamic variations and sheer stress from an altered angle of branching of the great vessels making identification of these variations vital for risk assessment prior to procedures. Accurate pre-natal delineation of the head and neck vessels can aid in appropriate prenatal counseling, genetic diagnosis, delivery planning and postnatal management especially when associated with critical aortic abnormalities. CT angiogram can complement pre and postnatal suspicion for appropriate surveillance guidelines and pre-procedural planning for surgical and endovascular procedures.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}