
These posters have been presented at meetings in Children's Mercy and around the world. They represent research that was done at the time they were created, and may not represent medical knowledge or practice as it exists at the time viewers access these posters.
-
 and Their Association with Subsequent Infections by Kedar Tilak, Neena Kanwar, Rangaraj Selvarangan, and Venkatesh Sampath")
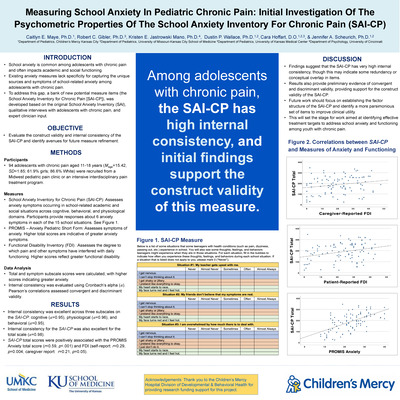
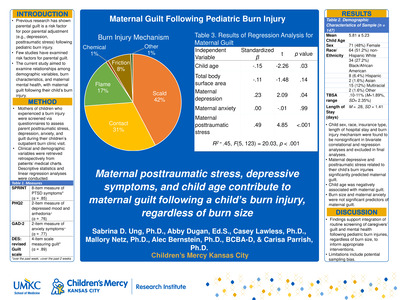
Epidemiology and Microbiology of Admission Surveillance Nasal Swabs in a Level IV Neonatal Intensive Care Unit (NICU) and Their Association with Subsequent Infections
Kedar Tilak, Neena Kanwar, Rangaraj Selvarangan, and Venkatesh Sampath
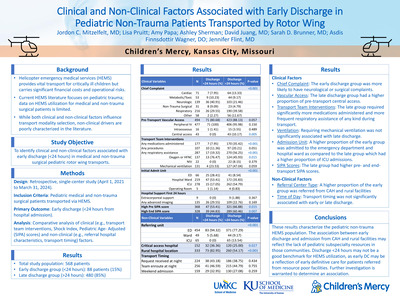
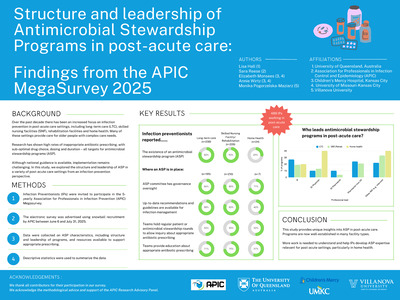
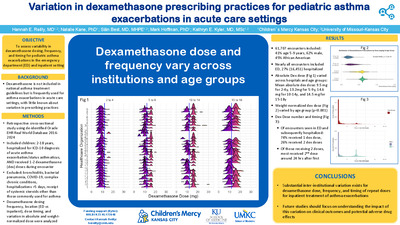
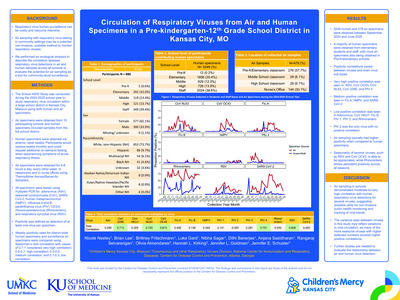
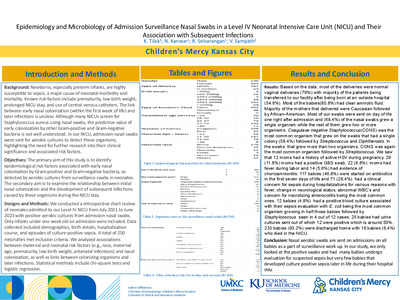
Background Newborns, especially preterm infants, are highly susceptible to sepsis, a major cause of neonatal morbidity and mortality. Known risk factors include prematurity, low birth weight, prolonged NICU stay, and use of central venous catheters. The link between early nasal colonization (within the first week of life) and later infections is unclear. Although many NICUs screen for Staphylococcus aureus using nasal swabs, the predictive value of early colonization by other Gram-positive and Gram-negative bacteria is not well understood. In our NICU, admission nasal swabs were sent for aerobic cultures to detect these organisms, highlighting the need for further research into their clinical significance and associated risk factors. Objectives The primary aim of this study is to identify epidemiological risk factors associated with early nasal colonization by Gram-positive and Gram-negative bacteria, as detected by aerobic cultures from surveillance swabs in neonates. The secondary aim is to examine the relationship between initial nasal colonization and the development of subsequent infections caused by these organisms during the NICU stay. Design/Methods We conducted a retrospective chart review of neonates admitted to our Level IV NICU from July 2021 to June 2023 with positive aerobic cultures from admission nasal swabs. Only infants under one week old on admission were included. Data collected included demographics, birth details, hospitalization course, and episodes of culture-positive sepsis. A total of 250 neonates met inclusion criteria. We are analyzing associations between maternal and neonatal risk factors (e.g., race, maternal age, prematurity, low birth weight, antenatal infections) and nasal colonization, as well as links between colonizing organisms and later infections. Statistical methods include chi-square tests and logistic regression. Results will be available by July 2025.
-

High-Frequency and Conventional Ventilation in Very Low Birth Weight Neonates During Interfacility Transport
Trevor Cabrera, Janelle R. Noel-Macdonnell, and Emily McNellis
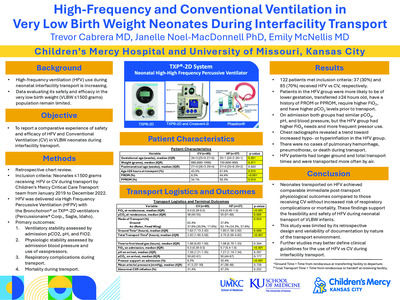
Background: Very low birth weight (VLBW) neonates (≤1500 grams) transported across neonatal facilities often require advanced respiratory support, including high-frequency ventilation (HFV). While HFV use in this setting has increased, data evaluating its safety and efficacy in the VLBW population remain limited. We hypothesized that HFV will provide a safe modality to transport sick VLBW infants. Objectives: To present a comparative experience of safety and efficacy of HFV and CV in VLBW neonates during interfacility transport. Methods: We retrospectively reviewed neonates ≤1500g who received invasive ventilation during interfacility transport by our transport team between January 2019 and December 2022. HFV was delivered using ……, while conventional ventilation (CMV) was delivered via ………Demographic, clinical, transport characteristics, ventilator settings, and respiratory variables were collected. We compared primary outcomes under three categories: (1) ventilatory stability assessed by hypocarbia (pCO2 < 35) or hypercarbia (pCO2 >55) at the end of transport; (2) respiratory complications during transport; and (3) transport mortality. Results: A total of 122 neonates met inclusion criteria; 37 (30%) received HFV and 85 (70%) received CV. Neonates transported on HFV were more likely to have been born at younger gestation, transferred at ≥24 hours old, have a history of PROM or PPROM, require higher FiO2 and have higher pCO2 levels at the transferring facility (Table 1). Upon arrival at the accepting facility, both groups had comparable admission pCO₂, pH, blood pressure, and oxygenation, despite higher FiO₂ and more frequent pressor use in the HFV group. No cases of pulmonary hemorrhage, pneumothorax, or death occurred during transport. HFV patients had longer ground and total transport times. Chest radiographs showed a non-significant trend toward more frequent hypo-/hyperinflation in the HFV group (Table 2). Conclusion: Our retrospective study suggests that both HFV and CV are associated with safe transport and comparable immediate post-transport physiological outcomes in VLBW neonates requiring interfacility transport with invasive ventilation. Despite being more critically ill requiring higher ventilatory support, neonates transported on HFV achieved similar ventilatory stability without increased risk of respiratory complications or mortality. These findings support the feasibility and safety of HFV during neonatal transport of VLBW infants. Future studies will define the clinical parameters that guide preference of HFV vs. CMV for choice of respiratory support. ,
-

Massively Dilated Aorta in a Neonate Leading to Symptomatic Right Heart Compression
Lauren Littell and Peter LaRossa
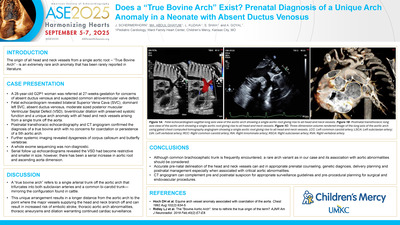
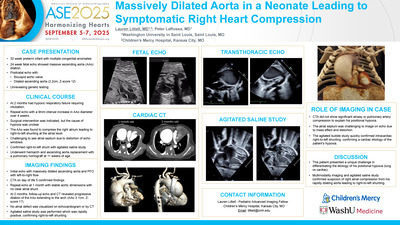
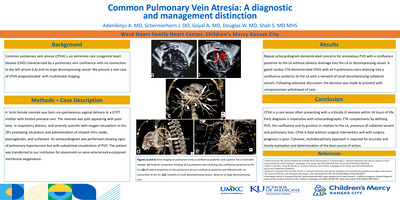
We present a case of a newborn, born at 32 weeks, with prenatally diagnosed massive ascending aorta (AAo) dilatation and multiple congenital anomalies with unrevealing genetic testing. Postnatal echo revealed a bicuspid aortic valve and a dilated AAo (2.2cm, z-score 12). At 2 months of age, he had progressive hypoxic respiratory failure requiring intubation, with frequent positional hypoxia despite adequate ventilation. Repeat echocardiogram showed a 9mm increase in AAo diameter over 4 weeks. Surgical intervention was indicated, but the cause of hypoxia was unclear. The dilated AAo was found to compress the right atrium, causing right-to-left shunting at the atrial level, confirmed by agitated saline study. The patient underwent hemiarch and AAo replacement with a pulmonary homograft at 11 weeks of age. Imaging Findings: Initial echo showed a bicuspid aortic valve, massively dilated AAo (2.2cm, z-score 12), and PFO with left-to-right flow. CTA on day of life 5 confirmed these findings. Repeat echo 1 month later showed stable aortic measurements with no clear atrial-level shunt. At 2 months, a follow up echocardiogram and confirmatory CTA revealed further dilation of the AAo, extending to the arch (3.1cm, z-score 17), with mild anterior tracheal mass effect. No atrial defect was seen, so an echo with agitated saline was performed, which was rapidly positive, confirming right-to-left shunting. Role of Imaging in Patient Care: CTA did not show significant airway or pulmonary artery compression. The atrial septum was challenging to image on echo due to mass effect and distortion. The agitated bubble study quickly confirmed intracardiac right-to-left shunting. Discussion This patient presented a unique challenge in differentiating the etiology of his positional hypoxia (lung vs cardiac). Multimodality imaging and agitated saline study confirmed suspicion right atrial compression from his rapidly dilating aorta, a very unusual finding in the absence of a known genetic disorder, leading to right-to-left shunting across the PFO.
-

No Suspicion for NOCARH: A Cautionary Tale of Anchoring Bias
Nicole DeMarco, Julia Allyson Hays, Bonnie Sullivan, Michael Price, Kimberly A. Horii, and Shannon Haines
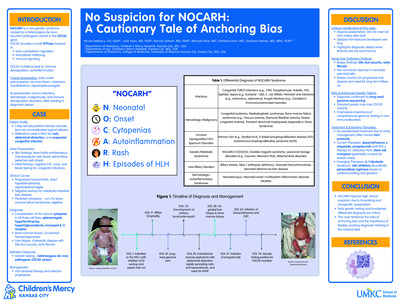
Introduction: Neonatal onset of cytopenia autoinflammation rash and hemophagocytic lymphohistiocytosis syndrome (NOCARH), a subset of hemophagocytic lymphohistiocytosis (HLH), is a rare and life-threatening condition characterized by uncontrolled immune response. It presents a diagnostic challenge in neonates due to the overlap of clinical features with other conditions, particularly congenital infections. We report a case of NOCARH in a late pre-term neonate, highlighting an atypical age group and the diagnostic difficulty of this syndrome. Case Presentation: A 1 day old ex-35 week er neonate presented to a level 4 NICU with chief complaints of pancytopenia,; an extensive petechialmaculopapular rash of on the her extremities, torso, and face ; e, abdominal distention;, hepatomegaly ; abnormal findings on abdominal film ; , and a systolic murmur . Initial symptoms prompted concern for congenital infection s, as well asand necrotizing enterocolitis. Comprehensive infectious disease testing yielded negative results. She was subsequently evaluated for immunodeficiency, liver, and thyroid associatedrelated diseases. Persistent profound pancytopenia, lymphadenopathy, elevated inflammatory markers, episodic rashes, growth failure, worsening cholestasis, and new onset lymphadenopathy episodic rashes at three weeks of age prompted expansion of differential and evaluation for NOCARH despite not fitting clearly into diagnostic criteria . Bone marrow biopsy confirmed the diagnosis with findings of hemophagocytosis without malignancy. Genetic evaluation identified a heterozygous pathogenic CDC42 mutation consistent with NOCARH syndrome. Management: Treatment included the administration of dexamethasone, intravenous immunoglobulin, and emapalumab, a monoclonal antibody targeting IFN-γ. Prophylactic Aantimicrobials were initiated for prophylaxis in the setting of her immunosuppression. Outcomes and Follow-up: The patient demonstrated clinical stabilization with improved resolving cytopenia and reduction in inflammatory markers. Her health ultimately improved , ultimately being able to beenough to discharged home with close follow-up with specialized care and ongoing multidisciplinarymultiple subspecialists , including Gastroenterology and Oncology follow-up. Bone marrow transplantation is planned to achieve long-term disease control. Conclusion: This case highlights the hazards of anchoring bias when evaluation for initial suspected medical condition is inconclusive. Early diagnosis and targeted therapy are critical to improving outcomes in this rare, high-mortality condition. Pediatricians and neonatologists should be aware of the potential for HLH to present in neonates, particularly in association with genetic syndromes like NOCARH. Introduction: Neonatal onset of cytopenia, autoinflammation, rash, and hemophagocytic lymphohistiocytosis syndrome (NOCARH), a subset of hemophagocytic lymphohistiocytosis (HLH), is a rare and life-threatening disorder driven by uncontrolled immune activation. Diagnosis in neonates is challenging because its features overlap significantly with congenital infections and other systemic inflammatory conditions. We present a case of NOCARH in a late preterm neonate, illustrating the diagnostic complexity and importance of early recognition in an atypical age group. Case Presentation: A 1-day-old ex-35-week neonate was admitted to a level IV NICU with pancytopenia, widespread petechiae, abdominal distention, hepatomegaly, and a systolic murmur. The initial differential diagnosis included congenital infections. Broad infectious workup was unrevealing. Over the next three weeks, the infant exhibited persistent cytopenia, lymphadenopathy, elevated inflammatory markers, and recurrent episodic rashes, raising suspicion for HLH/NOCARH despite not fully meeting diagnostic criteria. Bone marrow biopsy revealed hemophagocytosis without malignancy,
-

Pursuit of A Full Night's Sleep
Kennison Adams, Andrew Donaldson, and Brian S. Harvey
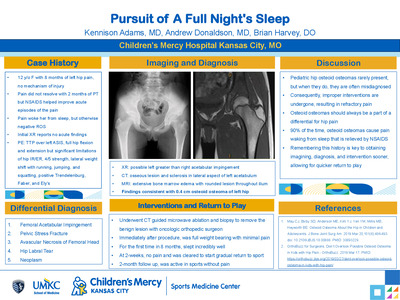
This project was a literature review and reflection upon the importance of having an osteoid osteoma on the differential for adolescent hip pain. The primary objective highlighted key attributes of this pathology and instructed readers to be vigilant in their assessment so that quicker diagnosis, management, and return to sport could occur.
-

Recombinant erythropoietin use for anemia of prematurity: a three year since center experience
Hannah Darland, Krishna Dummula, Chaitali Mahajan, and Vishal Pandey
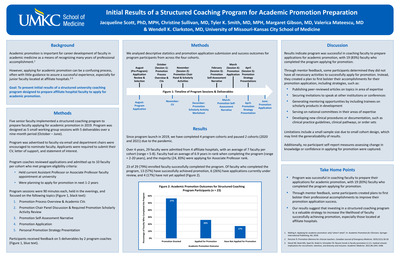
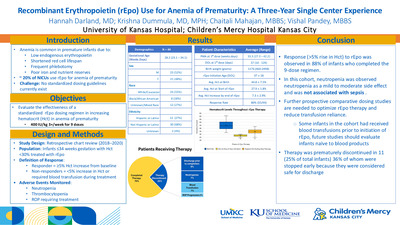
Background: Anemia is a common disorder of prematurity secondary to limited blood volume, excessive blood draws, inadequate nutrition, poor iron reserves, and insufficient endogenous erythropoietin. While many NICUs use recombinant erythropoietin (rEpo) to treat anemia of prematurity, the absence of universal guidelines has led to variability in dosing and schedules. Here we present our experience on the use of rEpo in a level 3 NICU. Our unit protocol uses 400 IU/kg three times a week for a total of 9 doses if hematocrit < 30%. Objectives: The purpose of this study was to evaluate the response to rEpo in infants with anemia of prematurity. Methods: Charts of infants born between 2018 and 2020 with gestation ≤34 weeks who received rEpo for anemia of prematurity were retrospectively reviewed. We defined response to therapy as an increase of hematocrit by 5% from pre-treatment baseline. Infants who did not achieve the therapeutic goal or who received blood transfusions were considered non-responders. Neutropenia, thrombocytopenia, and retinopathy of prematurity (ROP) requiring treatment were treated as adverse events. Results: A total of 44 infants were treated with rEpo during the study period. Clinical characteristics are described in Table I. Average hematocrit at birth was 44.8±7.5 (32.7 to 60.8). Infants were started on rEPO at a median corrected age of 33.3 ±3 weeks and a weight of 1674±622 g. Average DOL was 37±18 at initiation of therapy. Average baseline hematocrit at the start of therapy was 27.9±1.8%. 80% of patients (35/44) responded with increase of hematocrit by >5%, 20% (9/44) did not respond. 75% of infants (33/44) received all 9 doses. 11 patients received between 1-8 doses. Reasons for discontinuation of rEpo were: discharge prior to therapy completion (36%, 4/11), blood transfusion (27%, 3/11), neutropenia (27%, 3/11), and ROP progression (9%, 1/11). Average increase of hematocrit in the responders was 7.3±2.9%. In all, 11.4% of patients (5/44) developed neutropenia- none with ANC< 500 neutrophils/µl. None developed thrombocytopenia but 13.6% (6/44) had thrombocytosis >450,000 platelets/µl. 4.5% (2/44) required treatment for severe ROP, and no deaths occurred. Conclusion: rEpo was efficacious in increasing the hematocrit in the majority (80%) of convalescent preterm infants. Neutropenia observed during the therapy was mild-to-moderate (between 501-1500 neutrophils/µl) and did not result in invasive sepsis. Larger prospective comparative-dosing studies are needed to determine the ideal dose and timing of rEpo therapy in growing preterm infants to prevent late blood transfusions.
-

Severe Thiopurine-Induced Myelosuppression in a Pediatric ALL Patient with the NUDT15 *1/*6 Genotype
Jillian Fry, Keith August, Terrie Flatt DO, and Laura B. Ramsey
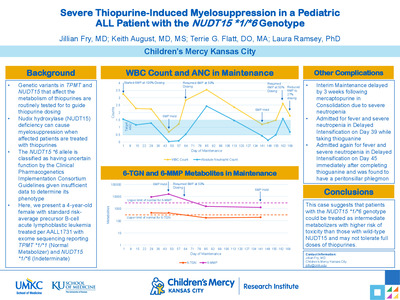
Introduction: Genetic variants in TPMT and NUDT15 that affect the metabolism of mercaptopurine (6MP) are routinely tested for to guide 6MP dosing. Nudix hydroxylase 15 (NUDT15) deficiency can cause myelosuppression when affected patients are treated with 6MP. The NUDT15 *6 allele is classified as having uncertain function by the Clinical Pharmacogenetics Implementation Consortium Guidelines given insufficient data to determine its phenotype. Here, we present the case of a pediatric patient with the NUDT15 *1/*6 genotype experiencing significant mercaptopurine-induced myelosuppression. Case Description: We present a 4-year-old female with standard risk-average precursor B-cell acute lymphoblastic leukemia treated per AALL1731. Exome sequencing reported TPMT *1/*1 (Normal Metabolizer) and NUDT15 *1/*6 (Indeterminate). In Maintenance Cycle 1, 6MP was started at standard dosing of 75 mg/m2/day. On Cycle 1 Day 29, her absolute neutrophil count (ANC) and platelets had decreased but remained within goal range. At that time, 6-thioguanine nucleotides (6-TGN) were at the higher end of normal at 445 pmol/8 x 108 RBC, and 6-methylmercaptopurine (6-MMP) was elevated at 9200 pmol/8 x 108 RBC. On Cycle 1 Day 47, she developed increased bruising and was found to have severe neutropenia with an ANC of 0.03 x 103 mcL and thrombocytopenia with platelets of 5 x 103 mcL. 6-TGN were relatively unchanged at 440 pmol/8 x 108 RBC, but 6-MMP had significantly increased to 16,177 pmol/8 x108 RBC. Given the degree of myelosuppression, 6MP was held. Her ANC and platelets did not recover until Cycle 1 Day 64, at which time 6MP was restarted at 50% of the original dose. She has not required any additional dose changes or disruption in Maintenance Cycle 2. Conclusions: This case suggests that patients with the NUDT15 *1/*6 genotype could be treated as intermediate metabolizers with higher risk of toxicity than those with wild-type NUDT15 and require dose reduction.
-

A Multipronged Approach to Developing & Marketing Asynchronous Resources to Faculty
Heather McNeill; Emilie Keeton, MSOD; Enam Haddad; Myles Chandler; Eric T. Rush; and Jacqueline Hill
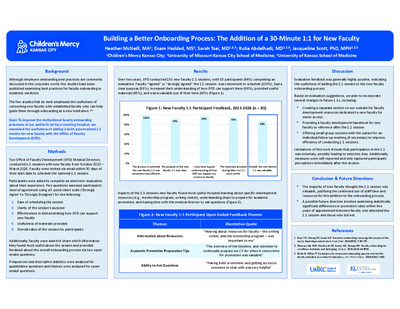
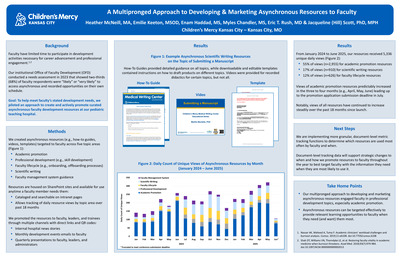
What suggested GFA topic does your submission align with? Organizational Policies, Practices and Procedures Intended/Target Audience Seasoned Faculty and Staff Mid-Career Faculty and Staff New Faculty and Staff Description Faculty have limited time for professional development. We piloted an approach to create and actively promote curated asynchronous professional development resources in five targeted topic areas and recorded resource use over two academic years (July 2023-July 2025). Since July 2023, we had 4,543 unique daily views; more than half (n=2,319) were views of academic promotion resources. Asynchronous resources engaged faculty in professional development topics, especially academic promotion. Additional information: Background: Faculty have limited time for professional development necessary for career advancement. Goal: Pilot an approach to develop and promote asynchronous faculty development resources at our pediatric teaching hospital. Methods: We created resources (e.g., how-to guides, templates, recordings) in topic areas such as academic promotion and professional development. The resources are hosted on SharePoint sites and cataloged on intranet pages, allowing us to track daily resource usage by area. We promoted the resources through targeted communications and presentations and recorded views from July 2023 to July 2025. Outcomes: From July 2023 to December 2024, we had 4,543 unique daily views. More than half (n=2,319) were views of promotion resources. Full data will be available at the conference. Conclusion: Our approach engaged faculty in asynchronous learning on faculty development topics, especially academic promotion. These data will inform changes to our resource catalogs. Learning Objectives After participating in this session, attendees should be able to… 1. Recognize the need for asynchronous resources among faculty 2. Explain how asynchronous resources can engage faculty in professional development 3. Identify opportunities to develop and promote asynchronous resources for faculty
-

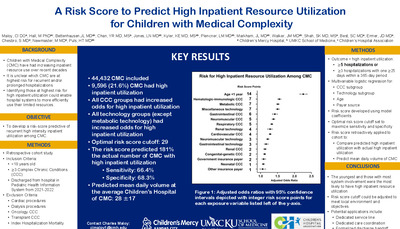
A Risk Score to Predict Recurrent High Intensity Inpatient Resource Utilization for Children with Medical Complexity.
Charles Maloy, Jessica L. Bettenhausen, Y Raymond Chan, Leah Jones, Kathryn Kyler, Laura Plencner, Jessica Markham, Jacqueline Walker, Smit Shah, Sian Best, Jonathan Ermer, Shelby Chesbro, Maria Newmaster M.D., and Henry T. Puls
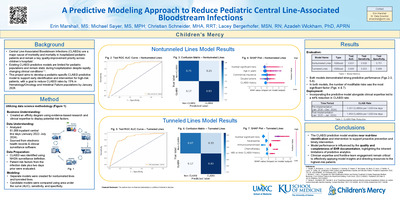
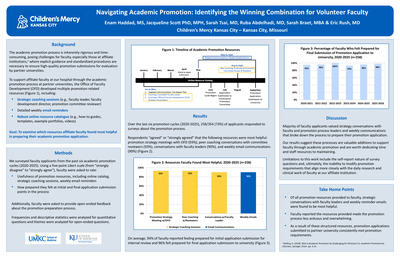
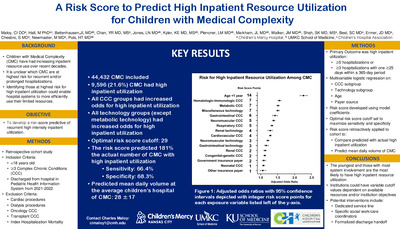
Background Children with medical complexity (CMC) use a greater amount of inpatient resources and stand to benefit from unique care models and coordination. However, hospital resources can be limited, and a better understanding of which CMC are high resource users could improve hospital and staff planning. Objective: To develop a risk score predictive of recurrent high intensity inpatient utilization among CMC. Methods: We conducted a retrospective cohort study of children < 18 years old with ≥3 complex chronic conditions (CCC) discharged from one of 48 children’s hospitals in the Pediatric Health Information System during 2021 and 2022. To reflect CMC typically cared for by a general medical service, children with cardiac procedures, dialysis, oncology, or transplant CCCs, and index hospitalization mortality were excluded. We used multivariable logistic regression to determine factors present on the index hospitalization associated with ≥5 hospitalizations or ≥3 hospitalizations with one lasting ≥25 days within any 365-day period (high inpatient utilization) in 2021-2023. We developed risk scoring system using model coefficients and defined the optimal risk score cutoff to maximize sensitivity and specificity. We then applied the risk score cutoff to children discharged to determine (a) ratio of predicted:actual CMC with recurrent high resource use and (b) the total predicted daily volume on 50th, 75th, and 90th percentile days for each hospital. Results: Of 44,432 included children , 9,596 (21.6%) had high inpatient utilization (Table). Children under 1 year of age had the highest odds of high inpatient utilization (OR 2.26 [95% CI: 2.16, 2.37]) and all CCC and technology groups (except metabolic) met statistical significance (Figure 1). The optimal risk score cutoff was 29 and predicted 17,411 (39.2%) CMC as high inpatient resource utilizers; the predicted:actual ratio of CMC with high inpatient utilization was 1.81. The mean daily census of the 50th, 75th, and 90th percentiles across hospitals was 28 CMC with recurrent high utilization (± 17), 34 (±18), and 39 (±19; Figure2). Conclusions: It is feasible to develop a risk score predictive of recurrent high inpatient utilization among CMC. There is substantial variability in volume of CMC with high utilization between pediatric hospitals. The risk score cutoff values can be modified to suit different applications and institution-specific objectives. These applications could include a dedicated service line or staffing. Alternatively, this could identify patients who would benefit from more formal handoff from inpatient to outpatient providers.
-

A Case of Early Pediatric-Onset Multiple Sclerosis
Mellanie De Guzman and Marcy Vandament
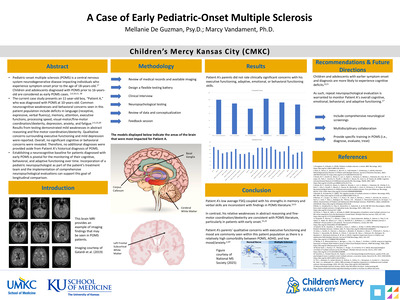
Pediatric-onset multiple sclerosis (POMS) is a central nervous system neurodegenerative disease impacting individuals who experience symptom onset prior to the age of 18-years-old.17 Children and adolescents diagnosed with POMS prior to 16-years-old are considered as early POMS cases. 1,6,10,11, 18 The current case study presents an 11-year-old boy, “Patient A,” who was diagnosed with POMS at 10-years-old. Common neurocognitive weaknesses and behavioral concerns seen in this patient population include deficits in language (receptive, expressive, verbal fluency), memory, attention, executive functions, processing speed, visual-motor/fine-motor coordination/dexterity, depression, anxiety, and fatigue.2-5,15,20 Results from testing demonstrated mild weaknesses in abstract reasoning and fine motor coordination/dexterity. Qualitative concerns surrounding executive functioning and mild depression were reported. Overall, no significant cognitive or behavioral concerns were revealed. Therefore, no additional diagnoses were provided aside from Patient A’s historical diagnosis of POMS. Establishing a neurocognitive baseline for patients diagnosed with early POMS is pivotal for the monitoring of their cognitive, behavioral, and adaptive functioning over time. Incorporation of a pediatric neuropsychologist as part of the patient’s treatment team and the implementation of comprehensive neuropsychological evaluations can support this goal of longitudinal comparison.
-

Scoring Large Muscle Movements in Pediatric Sleep Studies: An Educational Module for Sleep Technologists
Shauna Michelle VanDoren and David G. Ingram
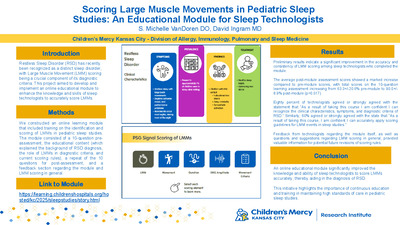
Introduction Restless Sleep Disorder (RSD) has recently been recognized as a distinct sleep disorder, with Large Muscle Movement (LMM) scoring being a crucial component of its diagnostic criteria. This project aimed to develop and implement an online educational module to enhance the knowledge and skills of sleep technologists to accurately score LMMs. Methods We constructed an online learning module that included training on the identification and scoring of LMMs in pediatric sleep studies. The module consisted of a 10-question pre-assessment, the educational content (which explained the background of RSD diagnosis, the role of LMMs in diagnostic criteria, and current scoring rules), a repeat of the 10 questions for post-assessment, and a feedback section regarding the module and LMM scoring in general. Results Preliminary results indicate a significant improvement in the accuracy and consistency of LMM scoring among sleep technologists who completed the module. The average post-module assessment scores showed a marked increase compared to pre-module scores, with total scores on the 10-question learning assessment increasing from 63.3+/-20.6% pre-module to 90.0+/- 8.9% post-module (p=0.017). Eighty percent of technologists agreed or strongly agreed with the statement that “As a result of taking this course I am confident I can recognize the clinical characteristics, symptoms, and diagnostic criteria of RSD.” Similarly, 60% agreed or strongly agreed with the state that “As a result of taking this course, I am confident I can accurately apply scoring guidelines for LMM events in sleep studies.” Feedback from technologists regarding the module itself, as well as questions and suggestions regarding LMM scoring in general, provided valuable information for potential future revisions of scoring rules. Conclusion An online educational module significantly improved the knowledge and ability of sleep technologists to score LMMs accurately, thereby aiding in the diagnosis of RSD. This initiative highlights the importance of continuous education and training in maintaining high standards of care in pediatric sleep studies.
-

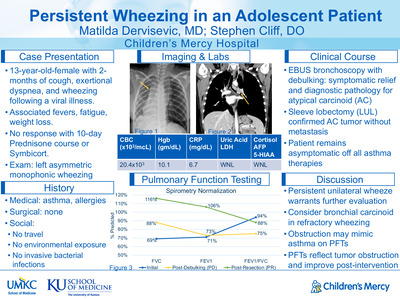
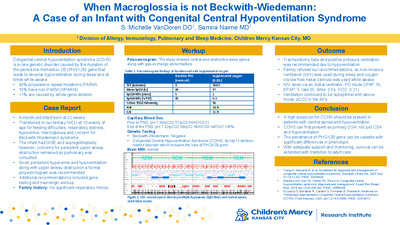
When Macroglossia is not Beckwith-Wiedemann: A Case of an Infant with Congenital Central Hypoventilation Syndrome
Shauna Michelle VanDoren and Samira Naime
Introduction Congenital central hypoventilation syndrome (CCHS) is a rare genetic disorder caused by the mutation of the paired-like homeobox 2B (PHOX2B) gene that leads to alveolar hypoventilation during sleep and at times while awake. The majority of patients with CCHS have polyalanine repeat mutations (PARM) whereas 10% have non-PARM (NPARM). Of those with NPARM, less than 1% are caused by whole gene deletion. NPARM is associated with more severe phenotypes; however, some may have variable penetrance causing variable presentation within families. Report of case(s) Our patient is a 4-month-old infant born at 32 weeks in an outside hospital and transferred to our tertiary NICU at 10 weeks of age due to feeding difficulties, respiratory distress, hypoxemia, macroglossia and concern for Beckwith-Wiedemann syndrome. Upon transfer, she was on 2L of oxygen (FiO2: 0.3) via high flow nasal cannula. During her stay, she was noted to have hypoventilation which was thought to be secondary to upper airway obstruction. Upper airway evaluation by ENT revealed mild laryngomalacia for which supraglottoplasty was performed. Drug induced sleep endoscopy (DISE) revealed macroglossia with posterior displacement of the epiglottis causing obstruction. Due to concerns for obstruction and persistent hypoxemia, she was referred for a polysomnogram (PSG). The study was started on room air, but 1/4L of oxygen via low flow nasal cannula (LFNC) was initiated after 6 minutes due to persistent hypoxemia and hypoventilation. PSG showed an apnea hypopnea index (AHI) of 18/hour, central apnea index (CAI) of 11/hour with persistent nocturnal hypoventilation based on ETCO2, transcutaneous CO2 monitor (TCM) and blood gas (ETCO2 > 50mmHg for 85% of total sleep time (TST), max ETCO2: 62mmHg, TCM>50mmHg for 96% TST, peak TCM: 70mmHg). Given these findings, recommendations were made to obtain PHOX2B gene testing and obtain neurologic workup. Exome sequencing showed deletion of the PHOX2B gene consistent with CCHS. Conclusion A high suspicion for CCHS should be present in patients with central apnea and hypoventilation. Many children with CCHS may be missed due to complex genetic testing and variation in clinical presentation.
-

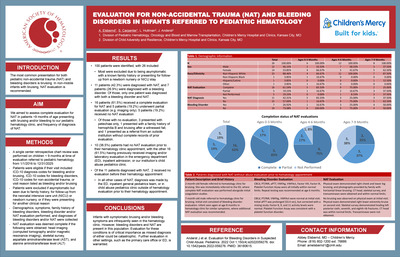
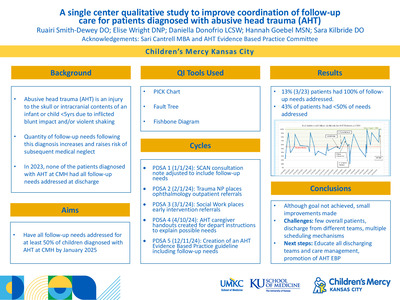
A single center qualitative study to improve coordination of follow-up care for patients diagnosed with Abusive Head Trauma
Ruairi Smith-Dewey, Elise Wright, Daniella Donofrio, Hannah Goebel, and Sara Kilbride
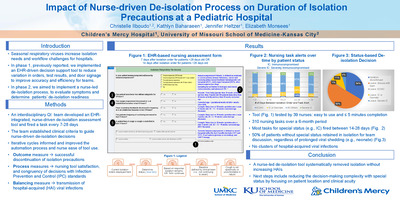
Introduction: Children diagnosed with abusive head trauma (AHT) have subsequent long-term developmental, behavioral, and medical consequences resulting in increased medical system utilization. There were 16 overall potential needs identified, with a single patient having 12. In 2023 at Children’s Mercy Hospital (CMH), 47% (8/17) of patients with AHT had < 50% of follow-up needs addressed at time of discharge. None had 100% of follow-up needs addressed. Needs not being addressed included need not identified or written documentation for need of follow-up without subsequent referral placed/appointment scheduled. Project goal was all follow-up needs to be addressed for at least 50% of children with AHT by January 2025. Methods (include PDSA cycles): Children admitted to CMH from January 2024-December 2024 and diagnosed with AHT by the Safety, Care & Nurturing (SCAN) team were included. Interventions were designed and implemented by a multidisciplinary team to address barriers including variation in scheduling process per specialty, lack of knowledge, and changing caregivers. • PDSA 1 (1/1/24): SCAN added standardized list of potential follow-up needs to documentation. • PDSA 2 (2/1/24): Trauma NP placed ophthalmology outpatient referrals. • PDSA 3 (3/1/24) Social work placed and documented early intervention referrals. Transitioned to SCAN RN responsibility. • PDSA 4 (4/10/24): AHT caregiver handouts with description of all potential follow-up needs added to discharge instructions. • PDSA 5 (12/11/24): AHT Evidence Based Practice guideline created including follow-up needs. Appointments and referrals were tracked by the author. QI tools used included fault tree, fishbone, and PICK Chart. Results: In 2024, 27 children were diagnosed with AHT by SCAN team at CMH. Five children were excluded from the study as 3 died and 2 were transferred to another hospital. The number of patients with < 50% of follow-up needs addressed was reduced from 47% to 43%. All follow-up needs were addressed in 13% (3/23) of patients. Conclusions: While project aims weren’t met, there was progress. Next steps include educating all discharging teams at CMH as there is no single team discharging these patients. Overall, there are few of these patients so standardization of discharge practices is challenging. SCAN created a working group and point person for appointment tracking to ensure follow-up needs established at discharge.
-

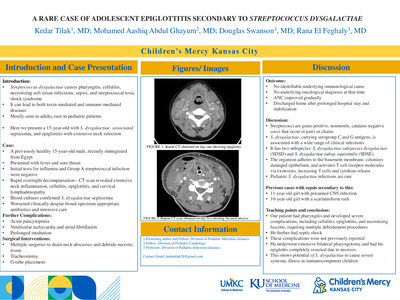
A Rare Case Of Adolescent Epiglottitis Secondary To Streptococcus Dysgalactiae
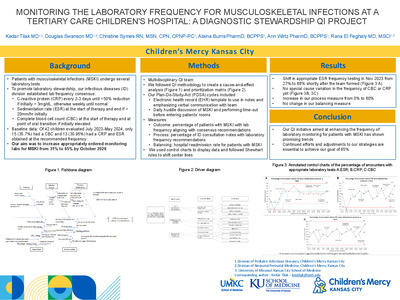
Kedar Tilak, Mohamed Aashiq Abdul Ghayum, Douglas Swanson, and Rana El Feghaly
Streptococcus dysgalactiae causes pharyngitis, cellulitis, necrotizing soft tissue infections, sepsis, and streptococcal toxic shock syndrome • It can lead to both toxin-mediated and immune-mediated diseases • Mostly seen in adults, rare in pediatric patients • Here we present a 15-year-old with S. dysgalactiae- associated septicemia, and epiglottitis with extensive neck infection
-

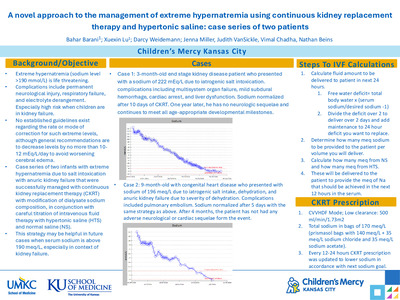
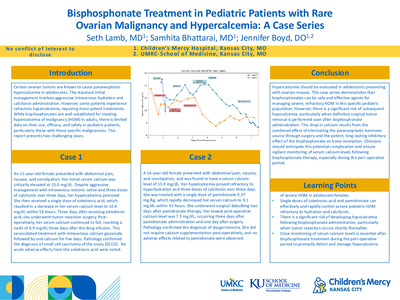
Bisphosphonate Treatment in Pediatric Patients with Rare Ovarian Malignancy and Hypercalcemia: A Case Series
Seth Lamb, Samhita Bhattarai, and Jennifer Boyd
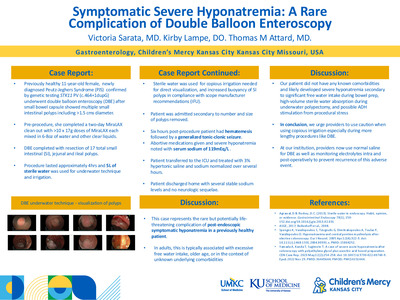
Objective: To describe the presentation, management, and outcomes of severe hypercalcemia in two adolescent females secondary to ovarian malignancy. Methods: The case series includes two adolescent female patients, aged 11 and 16, diagnosed with rare ovarian malignancies and associated hypercalcemia. The 11-year-old female was diagnosed with small cell carcinoma of ovary while the 16-year-old was diagnosed with dysgerminoma. Both patients presented with abdominal pain, nausea and constipation. The 11-year-old received zoledronic acid while the 16-year-old received pamidronate. Serum calcium level, symptoms and adverse effects were monitored before and after both medications. Results: Both patients presented with severe hypercalcemia. The 11-year old presented with serum calcium of 15.0 mg/dL while the 16-year old presented with a serum calcium of 15.9 mg/dL. Both patients were refractory to hyperhydration with isotonic normal saline and 3 or more doses of calcitonin over a span of 3 days. Patients were then given bisphosphonates to decrease severe hypercalcemia. Patient 1 received one dose of zoledronic acid 0.1 Unit/kg while patient 2 received pamidronate. Calcium decreased to 10.4 mg/dl in 56 hours after zoledronic acid administration. Patient also had her tumor resection 3 days after medication administration which further decreased serum calcium to a lowest of 6.9 mg/dl. This was improved after 1 dose of intravenous calcium gluconate. Patient 2 received 1 dose of pamidronate 0.37 mg/kg. Serum calcium decreased to 9.1 mg/dl in 41 hours. Patient had surgical debulking surgery the same day. Lowest post operative calcium level for patient 2 was 7.5 mg/dl 3 days post pamidronate and 1 day post tumor debulking. Diagnosis was confirmed by pathology to be small cell carcinoma of ovary-hypercalcemia type and dysgerminoma respectively for patient 1 and 2. Patient 1 required calcium supplementation for 5 days post-surgery while patient 2 needed no calcium supplementation. No adverse effects noted on both patients. Conclusion: Small cell carcinoma of ovary and dysgerminoma are rare causes of hypercalcemia in adolescents. These cases highlight the importance of recognizing paraneoplastic hypercalcemia, safety, efficacy, and monitoring for hypocalcemia after a single dose of bisphosphonate. Close monitoring is needed if patients plan to undergo tumor resection within the next week as both medications are known to have a long half-life.
-

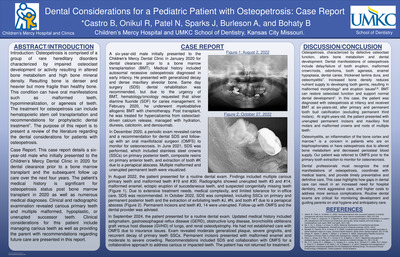
Dental Considerations for a Pediatric Patient with Osteopetrosis: Case Report
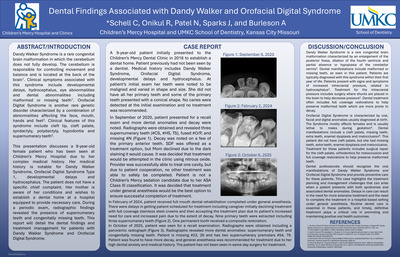
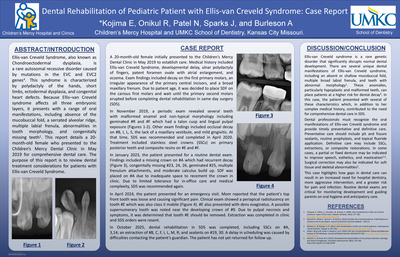
Bethany Castro, Robin Onikul, Neena Patel, Jenna Sparks, Amy Burleson, and Brenda S Bohaty
Introduction: Osteopetrosis is comprised of a group of rare hereditary disorders characterized by impaired osteoclast development or activity resulting in altered bone metabolism and high bone mineral density. Resulting bone is denser and heavier but more fragile than healthy bone. This condition can have oral manifestations such as malformed teeth, hypomineralization, or agenesis of teeth. The treatment for osteopetrosis can include hematopoietic stem cell transplantation and recommendations for prophylactic dental treatment7. The purpose of this report is to present a review of the literature regarding the dental considerations for patients with osteopetrosis. Case Report: This case report details a six-year-old male who initially presented to the Children’s Mercy Dental Clinic in 2020 for dental clearance prior to a bone marrow transplant and the subsequent follow up care over the next four years. The patient’s medical history is significant for osteopetrosis status post bone marrow transplant in 2020 as well as numerous medical diagnoses. Clinical and radiographic examination revealed carious primary teeth and multiple malformed, hypoplastic, or unerupted successor teeth. Clinical considerations for this patient include managing carious teeth as well as providing the parent with recommendations regarding future care are presented in this report.
-

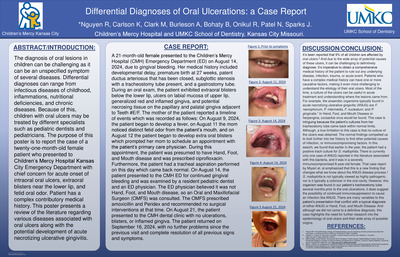
Differential Diagnosis of Oral Ulcerations: a Case Report
Richard Nguyen, Kaitlin Carlson, Meredith Clark, Amy Burleson, Brenda S Bohaty, Robin Onikul, Neena Patel, and Jenna Sparks
The diagnosis of oral lesions in children can be challenging as it can be an unspecified symptom of several diseases. Differential diagnoses can range from infectious diseases of childhood, inflammations, nutritional deficiencies, and chronic diseases. Because of this, children with oral ulcers may be treated by different specialists such as pediatric dentists and pediatricians. The purpose of this poster is to report the case of a twenty-one-month-old female patient who presented to Children’s Mercy Hospital Kansas City Emergency Department with chief concern for acute onset of intraoral oral ulcers, extraoral blisters near the lower lip, and fetid oral odor. Patient has a complex contributory medical history. This poster presents a review of the literature regarding various diseases associated with oral ulcers along with the potential development of acute necrotizing ulcerative gingivitis
-

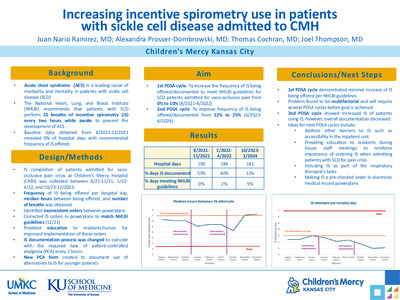
Increasing incentive spirometry use in patients with sickle cell disease admitted to CMH
Juan Nario Ramirez, Alexandra Prosser-Dombrowski, Thomas R. Cochran, and Joel Thompson
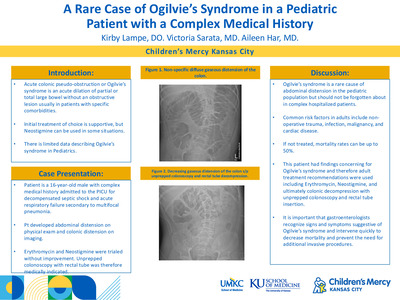
Acute chest syndrome is one of the leading causes of morbidity and mortality in patients with sickle cell disease. The National Heart, Lung, and Blood Institute (NHLBI) recommends that patients with sickle cell disease perform ten breaths of incentive spirometry (IS) every two hours while awake to prevent development of acute chest syndrome. By not meeting these guidelines, patients are more likely to develop this potentially life-threatening acute complication. To increase the use of IS in patients with sickle cell disease admitted to the hospital for vaso-occlusive pain. Patients were identified and IS occurrences were measured via review of electronic medical record. Of those patients admitted with sickle cell vaso-occlusive pain, the frequency that IS was offered or performed each hospital day was recorded. Partial admission and discharge days were excluded. For PDSA cycle 1, all IS orders in Cerner powerplans were updated to reflect current NHLBI recommendations. Additionally, education was provided to residents and nursing staff regarding the importance of the use of IS to prevent severe complications such as acute chest syndrome. Following PDSA cycle 1, a second meeting with stakeholders led to changing IS documentation to coincide with the required task of patient-controlled analgesia (PCA) assessment every two hours. Furthermore, as it is difficult for younger children to use IS appropriately, a new PCA form was created to document the use of alternatives to IS such as pinwheels or bubbles. Data obtained from 10/2023-12/2023 and 10/2024-12/2024 was then reviewed to evaluate the impact of PDSA cycle 2. From 8/2021-11/2021, there were 191 hospital days with patients admitted with sickle cell vaso-occlusive pain, of which 53% had IS documented. When IS was documented, 0% of patients received the recommended frequency of IS and the median hours between IS occurrences was 6.3 hours. From 12/2021-3/2022, 164 hospital days had IS documented 40% of the time with 2% of hospital days meeting the recommended frequency and 5.9 median hours between IS occurrences. From 8/2022-11/2022, 167 hospital days had IS documented 26% of the time with 12% of hospital days meeting the recommended frequency and 3.0 median hours between IS occurrences. From 10/2023 - 12/2023, 181 hospital days had IS documented 12.7% of the time with 9% of hospital days meeting the recommended frequency and 5.6 median hours between IS occurrences. From 10/2024 - 12/2024, 177 hospital days had IS documented 11% of the time with 15.7% of hospital days meeting the recommended frequency and 4.1 hours between IS occurrences. Implementation of uniform IS orders that match NHLBI recommendations resulted in an increase in the provision and frequency of IS used among the studied population. In PDSA cycle 2, implementation of IS documentation along with analgesia assessments resulted in an overall improvement of the median hours between IS occurrences and the number of hospital days with IS given at the recommended frequency, when IS was documented. It is important to note that the overall number of times in which IS was documented decreased compared to the first two cycles, however, the percentage of patients using IS at the recommended frequency continued to improve. For the next PDSA cycle, we will plan to address other potential barriers to IS documentation, such as accessibility to IS in the Hematology/Oncology inpatient unit . Further research will also focus on evaluating the impact of appropriate use of IS on the development of acute chest syndrome in our patient population.
-

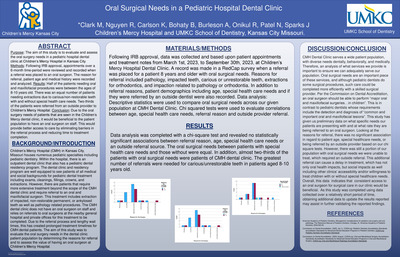
Oral Surgical Needs in a Pediatric Hospital Dental Clinic
Meredith Clark, Richard Nguyen, Kaitlin Carlson, Brenda S Bohaty, Amy Burleson, Robin Onikul, Neena Patel, and Jenna Sparks
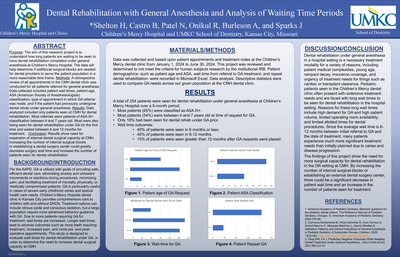
Purpose: The aim of this study is to evaluate and assess the oral surgery needs in a pediatric hospital dental clinic at Children’s Mercy Hospital in Kansas City. Methods: Following IRB approval, appointments over a 6-month time-period were reviewed and recorded when a referral was placed to an oral surgeon. The reason for referral, patient age and medical history were recorded and analyzed. Results: Half of the patients needing oral and maxillofacial procedures were between the ages of 8-10 years old. There was an equal number of patients needing extractions due to carious/non-restorable teeth with and without special health care needs. Two-thirds of the patients were referred from an outside provider to Children’s Mercy Hospital. Conclusion: Due to the oral surgery needs of patients that are seen in the Children’s Mercy dental clinic, it would be beneficial to the patient population to have an oral surgeon on staff. This would provide better access to care by eliminating barriers in the referral process and reducing time to treatment completion.
-

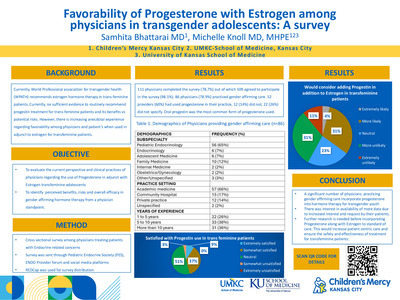
Physician Use of Progesterone in transgender adolescents: A survey
Samhita Bhattarai and Michelle Knoll
Objectives To evaluate the current perspective and clinical practices of physicians regarding the use of synthetic progestins as an adjunct to estrogen therapy in transfeminine adolescents. The survey focuses on perceived benefits, risks and overall efficacy in gender affirming hormone therapy. Methods A cross sectional survey was conducted among physicians who care for transfeminine patients. The survey included questions regarding their specialty, practice setting, age range of patients. Data was also collected regarding their indication for use, perceived benefits (e.g. breast development) and rationale if not using progestins for this purpose. Results Of 110 physicians who participated in the survey, 85 (77.2%) endorsed providing gender affirming care. Of those 85 respondents, 71(83.5%) have used progestins in some way, and 57 (67%) have used them as an adjunct to estrogen. Other uses included for contraception or amenorrhea in transmasculine patients, for suppression of endogenous puberty, and to induce patient requested hormone cycling. The most common form of progesterone used was oral progestin at 80.2% while depo medroxyprogesterone was used 21.1% Majority of the physicians (46/57, 80.7%) responded to being either somewhat satisfied or neutral to use of progestins. Of those who do not use progestins in transfeminine patients, most respondents noted lack of data on efficacy and side effects or lack of recommendations in guidelines. Others noted that it has not been necessary in achieving desired outcomes. Conclusions The survey indicates that while a significant number of physicians who practice gender affirming care incorporate progestins into hormone therapy for transgender youth, there was interest in more data on benefits and side effects on their use in transfeminine patients. Further research is needed to add to the current WPATH guideline to ensure more patient centric care along with ensuring its safety and effectiveness.
-

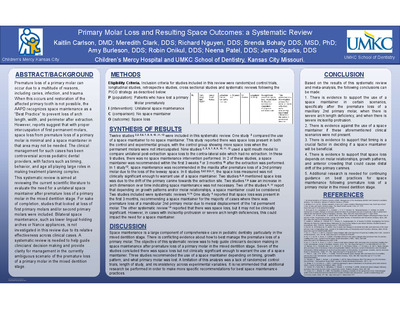
Primary Molar Loss and Resulting Space Outcomes: a Systematic Review
Kaitlin Carlson, Meredith Clark, Richard Nguyen, Brenda S Bohaty, Amy Burleson, Robin Onikul, Neena Patel, and Jenna Sparks
Premature loss of a primary molar can occur due to a multitude of reasons, including caries, infection, and trauma. When this occurs and restoration of the affected primary tooth is not possible, the AAPD recognizes space maintenance as a “Best Practice” to prevent loss of arch length, width, and perimeter after extraction. However, reports suggest that with proper intercuspation of first permanent molars, space loss from premature loss of a primary molar is minimal and a space maintainer in that area may not be needed. The clinical management for such cases has been controversial across pediatric dental providers, with factors such as timing, behavior, and age all playing large roles in making treatment planning complex. This systematic review is aimed at reviewing the current scientific literature to evaluate the need for a unilateral space maintainer after premature loss of a primary molar in the mixed dentition stage. For sake of completion, studies that looked at loss of first primary molars and/or second primary molars were included. Bilateral space maintenance, such as lower lingual holding arches or Nance appliances, is not investigated in this review due to its relative effectiveness across clinical cases. A systematic review is needed to help guide clinicians’ decision making and provide clarity for management in the currently ambiguous scenario of the premature loss of a primary molar in the mixed dentition stage.
-

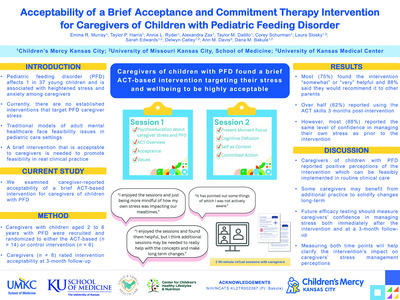
Acceptability of a Brief Acceptance and Commitment Therapy Intervention for Caregivers of Children with Pediatric Feeding Disorder
Emma Murray, Taylor P. Harris, Annie L. Ryder, Alexandra Zax, Taylor M. Datillo, Corey Schurman, Laura Slosky, Sarah T. Edwards, Delwyn Catley, Ann M. Davis, and Dana Bakula
Introduction: Pediatric feeding disorder (PFD) affects 1 in 37 young children and is associated with heightened stress and anxiety among caregivers. Currently, there are no established interventions that target PFD caregiver stress, and traditional models of adult mental healthcare face feasibility issues in pediatric care settings. To address this gap, we developed a brief acceptance and commitment therapy (ACT) intervention (Clinical Trials #NCT06001398). We assessed caregiver-perceived acceptability to inform future efficacy testing. Method: Twenty caregivers participated in a NIMH-funded pilot study of a 2-session ACT intervention for parents of children with PFD. Caregivers with children aged 2 to 6 years with PFD were recruited and randomized to either the active (n = 14) or control intervention (n = 6). Intervention content included psychoeducation, ACT skills training, and application of ACT skills to mealtimes. Caregivers’ rated intervention acceptability at 3-month follow-up. Results: Eight caregivers who received the ACT intervention completed acceptability measures. Most (75%) found it “somewhat” or “very” helpful. 62% reported using the ACT strategies 3 months following intervention completion and 88% said they would recommend this program to other parents. Most (88%) reported the same level of confidence in managing their own stress as prior to the intervention. Descriptively, caregivers enjoyed the sessions (“I enjoyed the sessions and just being more mindful of how my own stress was impact[ing] our mealtimes”). Conclusions: Caregivers found this brief ACT intervention to be highly acceptable. Caregivers reported regular use of the strategies, positive perceptions of the program, and that they would recommend it to others. Interestingly, they did not report feeling that their confidence in managing their stress improved. It is possible that retrospective comparisons about stress management may be difficult to assess, making it critical that we complete rigorous efficacy testing with pre-post measures of stress. Further efficacy testing is needed.
-

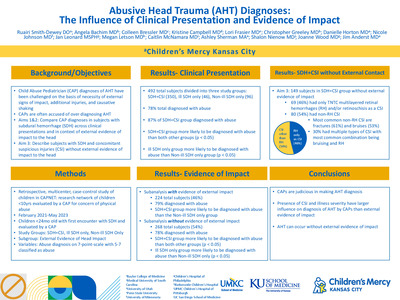
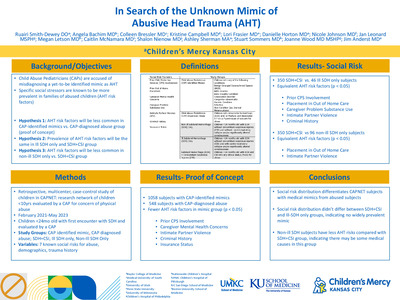
AHT Diagnoses: The Influences of Clinical Presentation and Evidence of Impact
Ruairi Smith-Dewey, Angela Bachim, Colleen Bressler, Kristine Campbell, Lori Frasier, Christopher Greeley, Danielle Horton, Nicole Johnson, Jan Leonard, Megan Letson, Caitlin McNamara, Ashley K. Sherman, Shalon Nienow, Joanne Wood, and James Anderst
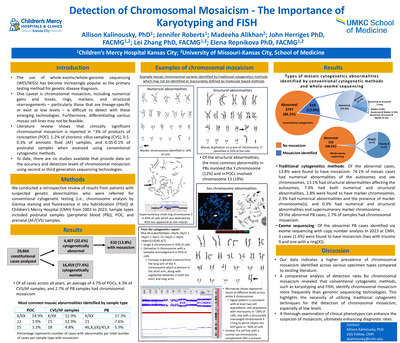
In cases where Child Abuse Pediatricians (CAPs) diagnose abusive head trauma (AHT) in young children, some factors surrounding the diagnosis have been challenged including causative shaking, necessity of external signs of impact, or concomitant suspicious injuries. Evaluation of CAP diagnoses in children with subdural hemorrhage (SDH) can give insight into factors related to the frequency of abusive head trauma (AHT) diagnoses. Additionally, characterization of those with SDH+CSI without evidence of impact may inform controversies around AHT diagnoses. Objective We aim to compare CAP diagnoses in subjects with SDH across clinical presentations and in the context of evidence of head impact. We also aim to describe the subjects with SDH+CSI and no external signs of impact to the head. Design/Methods Retrospective case-control study using Child Abuse Pediatrics Research Network (CAPNET) data from 10 sites over 27 months. Subjects were < 24 months old with SDH and in-person CAP evaluation. Subjects were divided into groups based on study determined criteria: Ill SDH only, Non-ill SDH only, and SDH with CSI. Ill status was categorized by clinical signs of cardio-respiratory collapse and/or significantly altered consciousness. CSIs are injuries highly associated with abuse in the following categories: skin, bones, eyes, and abdomen. CAP diagnosis of abuse was defined as 5-7 on a 7-point scale. Abuse diagnoses were compared across study groups. Head impact signs included bruising to the head, scalp swelling, and skull fractures. Comparisons used unadjusted odds ratios with 95% confidence intervals. Results Of the 492 study subjects, 386 (78%) were diagnosed with AHT. The SDH+CSI subjects were more likely to be diagnosed with abuse than Ill-SDH (OR 2.7, 95% CI 1.3-5.6) and Non-ill SDH (OR 7.2, 95% CI 4.3-12.1). Of the 276 subjects without signs of head impact, 215 (78%) were diagnosed with abuse. In this subgroup, SDH+CSI were more likely to be diagnosed with abuse than Ill-SDH (OR 3.7, 95% CI 1.5-9.2) and Non-ill SDH (10.3, 95% CI 5.0-21.1). Of the 157 subjects with SDH+CSI and no signs of head impact, 88/157 (56%) had non-head/eye related CSIs, including 52/88 (59%) with high specificity fractures and/or multiple fractures, 48/88 (55%) with high specificity bruising. Multiple types of CSIs were in 22/88 (25%). Conclusion(s) Among children with SDH, AHT is more frequently diagnosed in the presence of CSIs, particularly in the absence of external signs of impact. The high prevalence of CSIs in cases with SDH and no external signs of impact indicates that AHT can occur absent external signs of head impact.
-

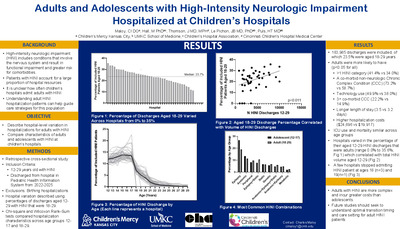
A Risk Score to Predict Recurrent High Intensity Inpatient Resource Utilization for Children with Medical Complexity.
Charles Maloy, Matt Hall, Jessica L. Bettenhausen, YR Chan, Leah Jones, Kathryn Kyler, Laura Plencner, Jessica Markham, Jacqueline Walker, Smit Shah, Sian Best, Jonathan Ermer, Shelby Chesbro, Maria Newmaster, and Hank Puls
Background
Children with medical complexity (CMC) use a greater amount of inpatient resources and stand to benefit from unique care models and coordination. However, hospital resources can be limited, and a better understanding of which CMC are high resource users could improve hospital and staff planning.
Objective:
To develop a risk score predictive of recurrent high intensity inpatient utilization among CMC.
Methods:
We conducted a retrospective cohort study of children < 18 years old with ≥3 complex chronic conditions (CCC) discharged from one of 48 children’s hospitals in the Pediatric Health Information System during 2021 and 2022. To reflect CMC typically cared for by a general medical service, children with cardiac procedures, dialysis, oncology, or transplant CCCs, and index hospitalization mortality were excluded. We used multivariable logistic regression to determine factors present on the index hospitalization associated with ≥5 hospitalizations or ≥3 hospitalizations with one lasting ≥25 days within any 365-day period (high inpatient utilization) in 2021-2023. We developed risk scoring system using model coefficients and defined the optimal risk score cutoff to maximize sensitivity and specificity. We then applied the risk score cutoff to children discharged to determine (a) ratio of predicted:actual CMC with recurrent high resource use and (b) the total predicted daily volume on 50th, 75th, and 90th percentile days for each hospital.
Results:
Of 44,432 included children , 9,596 (21.6%) had high inpatient utilization (Table). Children under 1 year of age had the highest odds of high inpatient utilization (OR 2.26 [95% CI: 2.16, 2.37]) and all CCC and technology groups (except metabolic) met statistical significance (Figure 1). The optimal risk score cutoff was 29 and predicted 17,411 (39.2%) CMC as high inpatient resource utilizers; the predicted: actual ratio of CMC with high inpatient utilization was 1.81. The mean daily census of the 50th, 75th, and 90th percentiles across hospitals was 28 CMC with recurrent high utilization (± 17), 34 (±18), and 39 (±19; Figure2).
Conclusions:
It is feasible to develop a risk score predictive of recurrent high inpatient utilization among CMC. There is substantial variability in volume of CMC with high utilization between pediatric hospitals. The risk score cutoff values can be modified to suit different applications and institution-specific objectives. These applications could include a dedicated service line or staffing. Alternatively, this could identify patients who would benefit from more formal handoff from inpatient to outpatient providers.
-

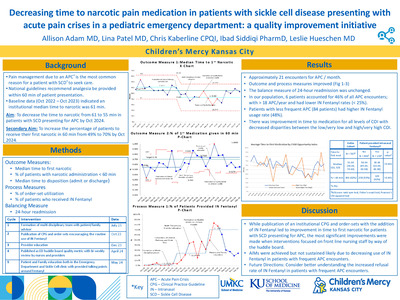
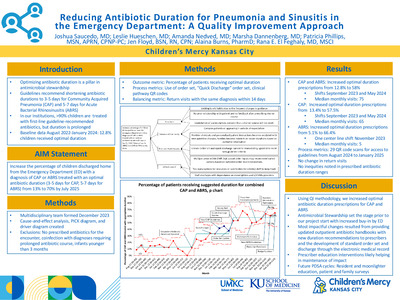
Decreasing time to narcotic pain medication in patients with sickle cell disease presenting with acute pain crises in a pediatric emergency department: a quality improvement initiative
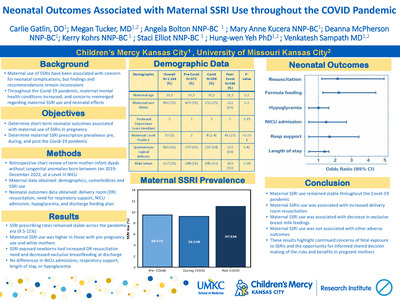
Allison Adam, Lina Patel, Christopher Kaberline, Ibad Siddiqi, and Leslie Hueschen



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}