
Publication Date
4-2026
Files
Download Full Text (343 KB)
Abstract
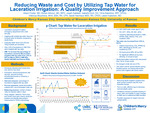
Purpose/Objective: Lacerations requiring closure make up 8 million emergency department (ED) visits annually. Irrigating prior to closure with potable tap water decreases cost and waste without increasing rates of infection compared to sterile fluids. Currently, only 3.5% of lacerations closed in our ED are irrigated with tap water. This project aims to increase the percent age of lacerations closed by ED providers irrigated with tap water from 3.5% to 60% by March 2026 in a freestanding pediatric emergency department across two sites (ED 1, ED 2). Design/Methods: A multidisciplinary team (physicians, nurses, QI consultant, parent advisors) formed in November 2024. Using driver diagram, fishbone, and PICK charts, interventions were identified and implemented in Plan-Do-Study-Act (PDSA) cycles (Table 1). The outcome measure was percentage of lacerations irrigated with tap water. Process measures were the number of sterile fluid bottles ordered for ED 2, order set usage, and rate of irrigation by nurses. The balancing measure was the rate of return visits for infection within 3 days. Fifty randomized charts were reviewed monthly. IRB deemed this study QI, not human subjects research. Results: Of 3,288 eligible encounters, 985 were randomized and included. Tap water irrigation increased from 3.5% to 64.6% (Fig 1). The average number of sterile bottles ordered monthly for ED 2 decreased from 102 to 16, representing a monthly savings of at least $430 and a reduction in plastic waste by at least 9 kg per month, reducing carbon emissions equivalent to 26 miles driven in a gas-powered car. There were no differences in irrigation by nurses or order set usage. There were no return visits for infection. Conclusion/Discussion: Altering the environment by removing sterile irrigation supplies from quick access locations was the most impactful intervention, allowing the team to meet their goal of increased tap water irrigation and decreased cost and waste. Future interventions include patient/family education and a new clinical pathway for lacerations. Limitations include inability to update order sets and limited monitoring of return visits. With the success of this project, the team plans to expand tap water irrigation to urgent care and subspecialist laceration repairs.
Disciplines
Emergency Medicine | Pediatrics
Recommended Citation
Fowler, Alison L.; Akhouri, Rohan; Galdean, Josaih; Dunt, Isabella; Kaberline, Christopher; Stoycheva, Viktoriya MHA, RN, CPN; Nienhaus, Sarah; and Hueschen, Leslie, "Reducing Waste and Cost by Utilizing Tap Water for Laceration Irrigation in the Emergency Department: A Quality Improvement Approach" (2026). Posters. 513.
https://scholarlyexchange.childrensmercy.org/posters/513



Notes
Presented at the 2026 Pediatric Academic Societies (PAS) Annual Meeting; Boston, MA; April 24-27, 2026.