
These slides have been presented at a meetings in Children's Mercy and around the world. They represent research that was done at the time they were created, and may not represent medical knowledge or practice as it exists at the time viewers access these slide presentations.
-

Parent satisfaction with same day discharge after laparoscopic appendectomy for non perforated appendicitis
Nelimar Cruz-Centeno, James Fraser, Shai Stewart MD, Derek Marlor, Rebecca M. Rentea, Pablo Aguayo, David Juang, Richard J. Hendrickson, Charles L. Snyder, Bhargava Mullapudi, Shawn D. St.Peter, Jason D. Fraser, and Tolulope A. Oyetunji
Background: Same-day discharge (SDD) after laparoscopic appendectomy for acute non-perforated appendicitis is safe, without an increased rate of postoperative complications, emergency department visits, or re-admissions. We aimed to evaluate caregiver satisfaction with this protocol. Materials and Methods: Patients discharged on the day of laparoscopic appendectomy for non-perforated acute appendicitis were identified between January 2022-August 2022. Surveys to evaluate satisfaction with the protocol were distributed to the caregivers via e-mail or text message 96 hours after discharge. Telephone surveys were conducted if there were no responses to the initial online survey. The surveys assessed comfort with SDD, post-operative pain control adequacy, post-operative provider contact, and overall satisfaction. The protocol focused on avoidance of narcotics in the postoperative period and immediate return to a regular diet. Results: A total of 255 cases of non-perforated acute appendicitis underwent SDD. The survey response rate was 50.6% (n=129). Most respondents were Caucasian (69.0%, n=89) and male (51.9%, n=67), with a median age of 12.0 years (IQR 8.9,14.7). The median postoperative length of hospital stay was 3.8 hours (IQR 3.2,4.8). The overall satisfaction rate was 91.5%, with 118 caregivers feeling satisfied with SDD. Most caregivers felt comfortable with the SDD protocol (89.9%, n=116), with 22.5% (n=29) calling a medical provider postoperatively. Approximately nine out of ten caregivers reported that pain was adequately controlled (91.5%, n=118). In contrast, those that were dissatisfied reported issues with pain control and anxiety with SDD after a surgical procedure. Conclusions: Caregiver satisfaction and comfort with same-day discharge following laparoscopic appendectomy is high with appropriate anticipatory guidance and preoperative education.
-

Persistent Pediatric Breast Abscesses Following Initial Treatment at Tertiary and Community Centers
Derek Marlor, Kayla B. Briggs, Shai Stewart MD, Nelimar Cruz-Centeno, Charlene Dekonenko, Tolulope A. Oyetunji, and Jason D. Fraser
Introduction: Our institution previously reported on outcomes of children with untreated and not spontaneously draining breast abscesses. This study aimed to evaluate the outcomes of all patients with breast abscesses who were evaluated at our institution. Methods: Following IRB approval, all patients < 18-years-old with breast abscesses were included. A total of 145 patients treated from January 2008-December 2018 were identified. Patients were divided into 2 groups; Group 1 included patients initially evaluated at our institution and Group 2 included patients who were initially evaluated at referring centers. The primary outcome was disease persistence. Secondary outcomes were antibiotic utilization, number and type of procedures performed, and risk factors for recurrence. Statistical analysis was performed using STATA® 17 with a p-value of <0.05 indicating significance. Results: A total of 145 patients were identified: 111 (76.6%) in Group 1 and 34 (23.4%) in Group 2. Demographics were similar between groups. Of the 111 patients in Group 1, 2 (1.8%)) were treated with observation alone, 58 (52.3%) were treated with antibiotics alone, 26 (23.4%) were treated with aspiration, and 25 (22.5%) were treated with incision and drainage. Of the 34 patients in Group 2, 4 (11.8%) were treated initially with observation, 22 (64.7%) with antibiotics alone, 5 (14.7%) with manual expression, 2 (5.9%) with incision and drainage, and 1 (2.9%) with warm compresses. Patients in Group 1 were more likely to receive needle aspiration (23.4% vs. 0%; p<0.001) or incision and drainage (22.5.% vs. 5.9%; p<0.001) as initial treatment. Compared to Group 2, patients in Group 1 were more likely to be prescribed clindamycin when treated with antibiotics alone (69.9% vs 18.2%; p<0.001). They also had a 12.6% persistent disease rate (n=14). Second treatment in those with persistent disease included aspiration in 50% (n=7), incision and drainage 45.5% (n=5), antibiotics 7.1% (n=1), and manual expression 7.1% (n=1). No patients had persistent disease following second treatment. Patients in Group 2 were more likely to be treated with antibiotics alone (64.7% vs. 52.3%; p<0.001), with trimethoprim/sulfamethoxazole being the most commonly prescribed antibiotic (54.6%). In patients with persistent disease treated at our institution following initial evaluation at a referring center, 50.0% were treated with antibiotics alone, 26.5% with aspiration, 17.7% with incision and drainage, and 5.9% with manual expression. Following treatment at our institution, the rate of persistent disease was similar between groups (12.6% vs 11.8%;). Conclusions: Persistent breast abscesses may be treated with antibiotics alone in community and tertiary care centers. Disease persistence is similar regardless of the initial treatment setting.
-

Clinical features and outcomes in pediatric severe scald burn patients
Ashley Daniel
Introduction/Hypothesis Young children with scald burns experience severe complications compared to older children. A paucity of data exists to support these observations. This study compares clinical features and complications of younger versus older pediatric patients with scald burns at four children’s hospitals participating in the Pediatric Injury Quality Improvement Collaborative (PIQIC). This collaborative includes five pediatric burn centers that utilize research to improve quality of burn care. 485 Methods This is a retrospective cohort study of scald burn patients admitted from 2010 to 2020 to four pediatric hospitals participating in PIQIC. Patients with total body surface area (TBSA) < 15% were excluded. Patients were categorized by age into three groups: toddlers (0–3 years), children (3-10 years), and adolescents (>10 years). The adolescent group was excluded with three patients in this group. Demographics, clinical features and adverse events were compared between age groups. For categorical variables, counts and percentages are reported; P-values were determined by Fisher’s Exact test. Continuous variables are reported using median and inter-quartile range; P-values were determined using the Wilcoxon Rank Sum test. Results Ninety-five patients were identified; 73 (76%) were in the toddler group. Although median burn size was larger in children (24 [21-36] vs 21 [18-30] % TBSA, p<0.001), toddlers had longer median intensive care unit (ICU) LOS (3 [2-16] vs 3 [2-9], p<0.001) and more median mechanical ventilator (MV) days (13 [1-137] vs 5 [2-138], p<0.001) than the child group. There was notable incidence of sepsis, nosocomial infection and abdominal catastrophe in the toddler group. Abdominal catastrophes only occurred in the toddler group, with 5 patients (7%) affected. Mortality was only observed in the child group (n=2, 9%). Conclusions Scald burns are more prevalent in the toddler group compared to the child group. Mortality risk may not be higher in this group, but they encounter longer ICU LOS, higher MV days, and incidence of sepsis, nosocomial infection, and abdominal catastrophe. This is one of the largest reports of abdominal catastrophe in this patient population to our knowledge. Continued investigation will help better understand this patient population.
-

Pediatric In-Hospital Cardiac Arrests: We Have More to Learn About Patient Demographics and Outcomes
Nathan LaVoy, John Cowden, Jenna Miller, Asdis Finnsdottir Wagner, Shekinah Hensley, and Stephen Pfeiffer
Introduction: Prior pediatric studies show an association between patient demographics and mortality after in-hospital cardiac arrests (IHCA). To our knowledge, this has not been assessed in pediatric intensive care units (PICU). This study aims to evaluate the impact of demographics and code characteristics on outcomes after IHCA in a quaternary referral PICU. Methods: A single center retrospective review of PICU IHCA events from 2010-2021 was performed. Patient demographics included age, gender, race/ethnicity, and language. Primary diagnosis was defined as cardiac or non-cardiac. The use of ECMO, CRRT, or defibrillation were included as code characteristics. The primary outcome was survival to hospital discharge. Adjusted odds of mortality (aOR) were obtained using PRISM III scores to adjust for illness severity. Data obtained via Virtual Pediatric System© and chart review. Results: 377 patients (median age 11 months) had 520 PICU IHCA events. 59.4% identified as White, 16.2% Black, 8.3% Hispanic, and 1.5% Asian. Overall survival was 49%. Adjusting for disease severity, there was no difference in survival rates between females (43.3%) vs. males (54%) [aOR 1.26(p=0.278)] or racial/ethnic groups: Hispanic 39.5% [aOR 1.75(p=0.214)], Asian 25.0% [aOR 4.74(p=0.063)], Black 51.2% [aOR 1.13(p=0.664) vs. White 51.1%. Language had no impact on survival: Spanish 36.8% vs. English 49.3% [aOR 1.08(p=0.912)]. Cardiac diagnosis survival was 54.5% vs. non-cardiac 42.2% [aOR 0.75(p=0.166)]. Although different, survival rates were not statistically significant in patients requiring ECMO (Black 33.3% [OR 1.70(p=0.485), Asian 0% [OR 1.99(p=0.302)] vs. White 45.9%), CRRT (Hispanic 20% [OR 1.49(p=0.999)], Asian 0% [OR: 1.34(p=0.819)] vs. White 27.3%), or defibrillation (Asian 0% vs. White 39.1% [OR 0.60(p=0.999)]). Conclusion: Controlling for illness severity, there were no statistically significant outcome differences based on demographics after IHCA in the PICU. This is inconsistent with previously published data on outcomes following IHCA. While this single center study did not assess CPR performance or post-arrest care, it provides framework for future analysis of IHCA in the PICU and identifying risk factors for mortality in this specific patient population.
-

Steven Johnson Syndrome/Toxic Epidermal Necrolysis Management in the Pediatric Population: The Surgeon’s Perspective
Shai Stewart MD, James Fraser, Ladonna Kearse, and Pablo Aguayo
Introduction
Stevens–Johnson Syndrome and Toxic Epidermal Necrolysis are rare, life-threatening cutaneous reactions resulting in epidermal detachment that is likened to partial thickness burns. There are sparse data with regards to wound management in the pediatric literature. We aimed to explore the current practices of pediatric-only burn centers in the Pediatric Injury Quality Improvement Collaborative to lay the framework for a standardized approach to wound care.
Methods
A 36-item survey was administered to pediatric surgeons at participating centers of the consortium. No patient specific data was collected.
Results
Surveys were completed from 4 out of the 5 institutions. The admitting service differed amongst all centers with patients being admitted to the burn team, critical care, general pediatrics, and infectious disease. The burn team primarily managed wounds (n=4) with one institution partnering with dermatology. Complete debridement occurred at one institution, gentle cleansing at two, and no debridement at one institution. Burn consults are obtained at least within 24 hours for all but one institution, where the threshold is TBSA >10%. Most dressing changes are performed daily (n=3) by the burn nurses (n=4). Enteral feeding is initiated within 24 hours universally. All institutions use antibiotic ointment and occlusive gauze as a primary dressing.
Conclusion
SJS/TEN is a rare but serious disease process in children with variations in practices and limited data on best management protocols. Further details into specific management protocols and outcomes may provide insight into best practice guidelines.
-

Get SMART: Implementation of Updated Asthma Guidelines for Pediatric Hospitalists
Alexander Hogan, Kathryn Kyler, and Claire Seguin
Prescription of Single Maintenance And Reliever Therapy (SMART) for moderate and severe persistent asthma is the most important and actionable improvement in the National Heart Lung Blood Institute (NHLBI) asthma guidelines for pediatric hospitalists. SMART is the use of a single inhaled corticosteroid/long acting beta agonist inhaler both as a daily preventive inhaler and as-needed for asthma symptoms. As hospitalists, we treat patients with poorly controlled asthma who will benefit from SMART asthma action plans. Despite ample evidence supporting use of SMART, implementation of such large changes in practice is challenging. Implementation science and quality improvement principles can be used to anticipate barriers and plan effective frameworks for increasing use of new guidelines in practice. Through work at our own institutions, we have identified common barriers to implementing the new SMART guidance. While no single solution is likely to lead to widespread uptake, multi-pronged efforts can support adoption of this practice change. In this session, we will review the new NHLBI asthma guidelines relevant to pediatric hospitalists, focusing on when and how to use SMART for our patients with asthma. Using historical experience in implementation of other care guidelines, we will discuss implementation barriers that have been described and may apply to SMART. We will share the experience with SMART at our own institutions and tools used for inter-disciplinary guideline dissemination and SMART implementation. Our goal is to aid attendees in creating organized changes in local practice. Attendees will receive an actionable toolkit to bolster efforts in implementation of SMART at their institutions. This toolkit will include quality improvement and implementation tools useful for targeting institution-specific barriers and tracking progress of SMART use.
-

Financial Outcomes by Severity Across Children's Hospitals
Jonathan Hartley, Jessica L. Bettenhausen, Matt Hall, David C. Synhorst, Jessica L. Markham, and James Gay
Background: Hospitalizations represent a significant driver of healthcare costs for children. Little is known about how payor type and the severity of children cared for on the general pediatric inpatient floor impact a hospital’s financial outcomes. Objective: The primary objective of this study is to compare financial outcomes of pediatric hospitalizations to the general floor across patient severity quartiles. Secondary objectives included financial outcomes stratified by payor type across severity quartiles. Methods: Retrospective cohort study included children aged 0-18 years discharged during calendar year 2019 from hospitals that reported clinical information to the Pediatric Health Information System database and financial data to the Revenue Management Program (Children’s Hospital Association, CHA). We excluded newborns, surgical and OB admissions, children requiring PICU or NICU, and transfers in and out. We calculated the ratio of reimbursements to costs (CCR; CCR <1.0 represents a financial liability to hospitals) and compared the CCR across severity quartiles and by payor type. Severity was determined using the Hospitalization Resource Intensity Score for Kids (H-Risk). Results: This study included 287,658 children within fourteen children’s hospitals. Patients were divided among four quartiles of H-Risk with quartile one being the least severe and quartile four the most. The majority of patients were in quartile one (55.5%) and had a public payor (54.4%). As severity increased the number of children with chronic complex conditions increased (CCC; 19.5% with 1 or greater CCC for quartile one and 88.5% for quartile four) and length of stay increased (a geometric mean of 1.8 days for quartile one and 11.3 days for quartile four). Overall, the CCR was 1.1 across all payors and severity levels representing a slight financial gain. Among private payors the CCR varied from 1.5 to 1.7 across severity quartiles. The median net financial gain ranged from $2,496 in quartile one to $37,257 in quartile four. Among public payors the CCR varied from 0.7 to 0.8 across severity quartiles. The median net financial loss ranged from $1,893 in quartile one to $22,513 in quartile four. Conclusions: Not unexpectedly, the financial gains and losses were higher for patients in higher severity quartiles. However, the net gain or loss varied substantially by payor. Utilizing the CCR in conjunction with the patient severity and payor mix may inform payment models and hospital operations, such as staffing models and patient placement, to ensure financial solvency.
-

Implementation of Longitudinal Learning Curricula Results in Improved ITE Scores and ABP Certifying Examination Pass Rates
Angela Etzenhouser, Emily Killough, and Danielle Reed
OBJECTIVE: To improve In-Training Examination (ITE) Scores and American Board of Pediatrics (ABP) Certifying Examination pass rates, our program implemented two longitudinal learning curricula; the objective of this study was to evaluate the effectiveness of these curricula. BACKGROUND: In 2018, we developed the “ITE Study Plan” which requires participation for residents whose ITE score falls below the national average. Residents develop a study plan that incorporates a minimum of 10 PREP questions per week along with any additional learning modalities they wish to utilize. Progress and compliance with the study plan is monitored monthly by an Associate Program Director. In 2019, the program implemented the Structured Independent Learner Curriculum (SILC), based on the work of Dr. Kris Rooney at Lehigh Valley Reilly Children’s Hospital. The SILC curriculum is required for all residents in the program and consists of earning “credits” for completing various board-relevant learning objectives each month. For lighter rotations, 6 credits per month are required. For more time-intensive months, 3 credits per month are required. Residents obtain credits for required learning such as conference attendance, online modules, and presentation of Morning Report. Additional credits can be earned according to the resident’s learning preferences and include online questions, articles, and podcasts. METHODS: In-Training Exam scores, ABP Certifying Exam scores, and ABP pass rates were tracked over a five-year period. Program scores were compared with the mean scores of all programs published with the ITE and ABP score reports. RESULTS: Since implementation of these two measures, our program has seen increased compliance with conference attendance and rotation requirements, a 330% increase in completed PREP questions, and an incremental rise in ITE scores above national means for both second- and third-year residents. ITE scores for interns remained stable over the study period. The program also saw an increase in ABP Certifying Examination pass rates, including in 2021 when nationally ABP pass rates were significantly lower. CONCLUSION: Implementation of longitudinal learning curricula improves both In-Training Examination Scores and American Board of Pediatrics Certifying Examination pass rates while reinforcing habits of life-long learning.
-

Assessing and Addressing Barriers to Fertility Preservation in Pediatric and Adolescent Patients at Risk for Infertility
Emily Burnett, Tennille Hilyard, and Julie Strickland
Fertility consultation is a recognized standard that should be offered to pediatric patients with fertility threatening diagnoses or undergoing fertility threatening therapy. The primary objective of this study is to determine how patients who did proceed with fertility preservation differ from those who declined the procedure. This study aims to assess barriers that may contribute to the underutilization of fertility preservation procedures after a formal consultation is completed.
-

Examining Diagnostic Variability Among Pediatric Subspecialists in Case Examples of Infant Head Injury
Angela Doswell, Emily Killough, James Anderst, Timothy Zinkus, and Ashley Sherman
Background: Clinical presentation, imaging, and ophthalmologic findings are important factors in distinguishing between noninflicted and abusive head trauma (AHT) in infants. However, little is known about agreement between pediatric subspecialists regarding diagnosis and timing of AHT in infants. Hypothesis/Objects: The primary outcome was differences in rates of AHT diagnosis among different types of pediatric subspecialists using case examples of infant head injury. The secondary outcome was qualitative trends in clinical reasoning related to injury timing. Methods: Four case examples of infant head injury were developed into an online survey. Cases were categorized as: (1) “bilateral mixed density subdural hemorrhages (SDHs)”; (2) “hyperdense right/interhemispheric SDH”; (3) “bilateral SDHs with membranes”; and (4) “hyperdense right SDH”. Each case assessed diagnosis regarding infant head injury, likelihood of AHT diagnosis, and timing of head injury given clinical presentation, laboratory, neuroradiology, and ophthalmologic findings. Participants evaluated at least 1 possible case of AHT during their career and identified as being a part of 1 (or more) of the following 5 pediatric subspecialties: Child Abuse Pediatrics (CAP), Pediatric Emergency Medicine (PEM), Pediatric Critical Care (PCC), Neurosurgery (NS) and Pediatric Hospital Medicine (PHM). The response selected by most CAPs was the reference and compared across subspecialties using Chi-square or Fisher’s exact tests. Bonferroni corrections were used to determine statistical significance. Qualitative responses were coded individually, with more frequent responses being grouped into such categories as clinical presentation (i.e., symptoms, labs, or other information provided in clinical vignette), neuroimaging findings (i.e., SDH characteristics) and ophthalmologic findings (i.e., presence and/or type or retinal hemorrhages). Results/Conclusion: A total of 288 participants completed at least 1 case. Roughly 26.7% of participants were CAPs, and 64% of participants reported evaluating at least 26 cases of possible AHT during their careers. For case 1, 100% of CAPs diagnosed AHT with no significant difference detected across subspecialties (100% PEM, 83.3% PCC, 100% NS, and 97.1% PHM diagnosed AHT). For case 2, 57.9% of CAPs did not diagnose AHT, but significantly fewer PHM (34.9%, p=0.0061), PEM (28.0%, p<0.0001) and NS participants (24.0%, p=0.0033) did not diagnose AHT. For case 3, 72.2% of CAPs diagnosed AHT with no significant difference detected across subspecialties (73.6% PEM, 66.7% PCC, 80.8% NS, and 84.1% PHM diagnosed AHT). For case 4, 39.4% of CAPs reported uncertainty with AHT diagnosis, with no significant difference detected across subspecialties (34.8% PEM, 50.0% PCC, 42.3% NS, and 34.3% PHM reported uncertainty with AHT diagnosis). In case 1, most participants reported neuroimaging findings as most helpful with injury timing. In cases 2 through 4, most participants reported clinical presentation as most helpful with injury timing. Statistically significant diagnostic variability across pediatric subspecialties was detected in only 1 case example of infant head injury; however, variability persisted across the 3 remaining cases. Further research and/or education regarding the determination of AHT diagnosis and timing of infant head injuries is warranted to aid in the medical decision-making process and decrease diagnostic variability.
-

Financial Outcomes by Severity Across Children's Hospitals
Jonathan Hartley, Jessica L. Bettenhausen, Matt Hall, James Gay, David C. Synhorst, and Jessica L. Markham
Background: Hospitalizations represent a significant driver of healthcare costs for children. Little is known about how payor type and the severity of children cared for on the pediatric medical inpatient floor impact a hospital’s financial outcomes. Objective: The primary objective of this study is to compare financial outcomes of pediatric hospitalizations to the medical inpatient floor across patient severity quartiles. Secondary objectives included financial outcomes stratified by payor type across severity quartiles. Methods: Retrospective cohort study included children aged 0-18 years discharged during calendar year 2019 from hospitals that reported clinical information to the Pediatric Health Information System database and financial data to the Revenue Management Program (Children’s Hospital Association, CHA). We excluded newborns, surgical and OB admissions, children requiring PICU or NICU, and transfers in and out. We calculated the ratio of reimbursements to costs (CCR; CCR <1.0 represents a financial liability to hospitals) and compared the CCR across severity quartiles and by payor type. A net margin median was calculated as median reimbursement minus median costs. Severity was determined using the Hospitalization Resource Intensity Score for Kids (H-Risk). Results: This study included 163,656 children within 14 children’s hospitals. Patients were divided equally among four quartiles of H-Risk with quartile 1 being the least severe and quartile 4 the most. The majority of patients had a public payor (54.4%). As severity increased the number of children with chronic complex conditions increased (CCC; 6.8% with 1 or greater CCC for quartile 1 and 78.7% for quartile 4) and length of stay increased (a geometric mean of 1.4 days for quartile 1 and 3 days for quartile 4). Overall, the CCR was 1.1 across all payors and severity levels representing a slight positive margin. Among private payors the CCR varied from 1.6 to 1.7 across severity quartiles which resulted in a median net positive margin $2,544 in quartile 1 and $7,855 in quartile 4. Among public payors the CCR varied from 0.7 to 0.8 across severity quartiles which resulted in a median net negative margin of ($1,404) in quartile 1 and ($905) in quartile 4. Conclusions: Net financial outcomes varied substantially by payor. Utilizing the CCR in conjunction with the patient severity may inform payment models and hospital operations, such as staffing models and patient placement, to ensure financial solvency.
-

Improving Antibiotic Durations for Skin and Soft Tissue Infections in Pediatric Urgent Care Clinics
Megan Hamner, Amanda Nedved, Holly Austin, Donna Wyly, Alaina N. Burns, Brian Lee, and Rana El Feghaly
Background: Skin and soft tissue infections (SSTIs) are the second most common diagnosis leading to pediatric antibiotic prescriptions in the outpatient setting after respiratory diagnoses. However, most antibiotic stewardship programs have mainly focused on respiratory diagnoses. Children seen in the ambulatory setting for SSTIs often receive >7 days of antibiotics, although current society guidelines recommend 5-7 days for most diagnoses. Objective: To increase the percentage of patients receiving 5-7 days of oral antibiotics for SSTIs from 58% to 75% by December 31st, 2021, in pediatric urgent care clinics (UCCs). Design/Methods: We formed a multidisciplinary team in April 2020. We completed cause-and-effect analyses and developed a driver diagram (Figure 1). Plan-Do-Study-Act (PDSA) cycle 1 provided an update on current guidelines for UCC providers. PDSA cycle 2 modified the electronic health record to display antimicrobial order sentences from shortest to longest duration. PDSA cycle 3 provided project outcome and balancing measure updates to UCC providers at regular intervals. We created a monthly report of patients 90 days and older seen in UCCs with a final diagnosis of SSTIs including impetigo, abscesses, cellulitis, erysipelas, folliculitis, paronychia, and animal bites. Our outcome measure is the percentage of patients receiving 5-7 days of oral antibiotics for SSTIs. Process measure is the percentage of prescriptions selected from a folder. Balancing measure is the number of patients returning for SSTI within 14 days of their visit. Results are displayed using an annotated control chart. Results: The percentage of patients receiving 5-7 days of oral antibiotics during the baseline period (June 2019-June 2020) was 58%. After project initiation in April 2020, this increased to 68%, and consistently increased following PDSA cycles to a sustainable rate of >80% (Figure 2). A total of 1,971 UCC visits were included in the analysis. Process measure revealed less than 10% of providers utilize prescription folders. There was no change in balancing measure numbers. Conclusion: Prior to our project, only 58% of children seen in pediatric UCCs for SSTIs received the recommended antibiotic duration. By addressing primary drivers uncovered through QI methodology, we surpassed our goal of 75%. Additional PDSA cycles are planned along with expansion to other departments. This work will allow us to expand antibiotic stewardship efforts to other infectious diagnoses as well.
Presented at 2022 PAS Conference; Denver, CO; April 2022.
-

Outpatient Emergency Preparedness
Mary Haywood
It is commonly believed that medical emergencies do not present to general pediatric offices. However, it has been estimated that 0.9-42 emergencies per office site/year occur. The most common presentations are respiratory in nature. However, children can also present with dehydration, seizure, psychiatric or behavioral complaints. Despite this, most offices are not prepared to handle these presentations for various reasons. Multiple studies have showed that preparedness in inpatient settings is improved with education, implementation, or protocols and deliberate practice with mock codes. However, there have been few studies in the outpatient setting. One study utilized simulation as a tool to improve preparedness in an outpatient setting. This study hopes to improve outpatient preparedness as well as identify latent safety threats in the outpatient setting by utilizing rapid cycle simulation in clinics around the Kansas City area.
-

Parental Teach Back in the ED setting for Non-English Speaking Families
Rohan Akhouri
90 million Americans have low health literacy1.in Missouri 35% of adults have prose literacy at or below basic skill level2. Literacy, more specifically health literacy, is a modifiable social determinant of health that has a large impact on patient care and outcome. Poor health literacy in adults is associated with a higher number of ED visits and worse health outcomes3,4. Teach back is a method used in multiple pediatric and adult settings, shown to improve patient outcomes and comfort with discharge instructions5. There is limited data regarding teach back in non-English speaking patients and its efficacy with this group of patients. Our long-term goal is to address disparity in discharge education for non-English speaking patients in the Emergency Department with the use of the teach back method. Our central hypothesis is that using the “Teach Back” method with non-English speaking patients will improve patient medication compliance, and reduce return to ED. To test our central hypothesis and attain the overall objective, we will pursue the following specific aims: Aim 1. Use teach back with non-English speaking patients for discharge instructions. Our working hypothesis is that using teach back for non-English speaking patients will improve patient understanding of discharge instructions and reduce ED return times. We will complete surveys post-discharge with families via phone Aim 2. Measure patient compliance with medications after discharge. Our central hypothesis is that using teach back in the ED setting at discharge will improve patient medication compliance.
-
 by Angela Doswell, James Anderst, Joel Tieder, Henry T. Puls, and BRUE Research and Quality Improvement Network")
Rates of Physical Abuse Screening and Detection in Infants with Brief Resolved Unexplained Events (BRUEs)
Angela Doswell, James Anderst, Joel Tieder, Henry T. Puls, and BRUE Research and Quality Improvement Network
Background: “Apparent Life-Threatening Events” (ALTEs) have been associated with child physical abuse (CPA). In 2016, “Brief Resolved Unexplained Event” (BRUE) and the development of its clinical guidelines and risk-stratification replaced ALTE. However, it is unknown if there is a similar association between BRUEs and CPA. Hypothesis/Objectives: To determine the rate of CPA in infants presenting with a BRUE, examine differences between infants with and without CPA, and to examine rates of diagnostic testing used to detect CPA. Methods: This study was part of the BRUE Research and Quality Improvement Network, composed of 15 hospitals. Subjects were infants presenting with BRUE in emergency department or inpatient settings. Subjects were followed from BRUE presentation through the first year of life for possible diagnosis of CPA at either initial BRUE or subsequent presentations. The primary outcome was CPA diagnosis at either initial BRUE or subsequent presentations. CPA was the only maltreatment type identified. The secondary outcomes were minor evidence of trauma and diagnostic testing used to detect CPA (head imaging, skeletal survey, and/or liver transaminases) at initial BRUE presentation. Chi-square tests assessed for differences. Results/Conclusion: Of the 2036 infants presenting with a BRUE, 7 (0.3%) were diagnosed with CPA, 5 of whom had findings consistent with abusive head trauma (AHT). Only 1 infant was diagnosed with CPA (cutaneous injury) at initial BRUE presentation (<0.1%). For the remaining cases, 1 infant was diagnosed with AHT within 3 days, 1 with AHT and cutaneous injury within 31-60 days, 1 with abusive fractures within 31-60 days and 3 with AHT more than 60 days after initial BRUE presentation. Infants diagnosed with CPA were more likely to be White (85.7% vs. 48.3%, p<0.05), to exhibit color change (100% vs. 51.1%, p=0.01) and have minor evidence of trauma (14.3% vs. 0.3%, p<0.001) at initial BRUE presentation. There was no difference between CPA diagnosis and BRUE risk stratification. There were 7 (0.3%) infants with minor evidence of trauma: 1 was diagnosed with CPA, 3 were iatrogenic, 1 birth-related and 2 multiple yet nonspecific minor traumas. Of all infants, only 6.2% underwent head imaging, 7% skeletal survey, and 12.1% liver transaminases. Skeletal survey was more likely to be performed if there was minor evidence of trauma (42.9 vs. 6.9%, P <0.001) or a concerning social history (13.9% vs. 5.9%, p <0.05). Head imaging was more often performed if infants had minor evidence of trauma (71.4% vs. 6.0%; p< 0.001), family history of sudden unexplained death (10.2% vs. 6.3%; p= 0.047) or concerning social history (22.8% vs. 5.4%; p< 0.001). There was a lower rate of CPA in infants at initial BRUE presentation (<0.1%) than in infants with ALTE, although testing rates at initial BRUE presentation were also low. Minor evidence of trauma and other clinical features appeared to raise suspicion and initiate diagnostic testing to detect CPA. Further research is warranted to systematically identify and diagnose infants with BRUE at increased risk for CPA.
-

Spending on Public Benefit Programs and Exposure to Adverse Childhood Experiences
Megan Collins, Matt Hall, P J. Chung, Jessica L. Markham, Jessica L. Bettenhausen, L M. Plencer, Molly Krager, Kathyrn Kyler, D Bard, Kayla R. Heller, Roxana Guggenmous, Jordan Keys, and Henry T. Puls
Background: Adverse childhood experiences (ACEs) have been shown to be associated with poor health outcomes, and children living in poverty are more likely to experience ACEs. Our objective was to estimate the association between spending on benefit programs and cumulative exposure to ACEs among children. Methods: This cross-sectional study examined state and federal spending, at the state-level, on 5 categories of public benefit programs: cash, housing, and in-kind assistance; housing infrastructure; childcare assistance; refundable Earned Income Tax Credit; and Medical Assistance Programs (e.g., Medicaid). The primary exposure was median annual spending per person living below the federal poverty limit across 2010-2017 Federal fiscal years (i.e., one observation per state). The primary outcome was state-level percentage of children aged <18 years having ever been exposed to>≥ 4 ACEs, as reported in 2016-2017 National Survey of Children’s Health. Pearson correlations estimated unadjusted correlations. Linear regression models estimated associations after adjustment for states’ racial and ethnic demographics. A sub-analysis including only children 0-8 years of age was conducted to more closely focus on children who could have been first exposed to ACEs in the 2010-2017 Federal fiscal years. Results: Among the 51 states, a median of 6.3% of children (IQR: 5.2, 7.6) had exposure to ≥4 ACEs. Spending varied between states and was correlated with the percent of children with ≥ 4 ACEs (r= -0.41 [95% CI: -0.62, -0.15, p= 0.003]; Figure 1). Total spending on all benefit categories combined was associated with lower exposure to ≥ 4 ACEs (β coefficient= -0.11 [95% CI: -0.18, -0.04]; p= 0.005). This association suggests that for each additional $1000 spent per person living in poverty, there was an associated -0.7% point difference, or 496,379 fewer children accumulating ≥4 ACEs nationally. Increased spending in each individual benefit category was also associated with decreased reported ACEs exposure (Table 1, Figure 2; all p <0.05). Among children 0-8 years, greater average annual total spending as well as spending on cash, housing, and in-kind assistance; childcare assistance; and Medical Assistance Programs remained significantly associated with decreased reported ACEs exposure (Table 1). Conclusions: Average annual spending on benefit programs was associated with less cumulative exposure to ACEs. Investments in public benefit programs not only decrease childhood poverty but may also have broad positive effects on near- and long-term child well-being beyond the programs’ stated objectives.
-

Assessing Early Use and Complications of Gastrostomy Blended Feeds
James Fraser, Shai Stewart MD, Kristen L. Sayers, Amy L. Pierce, Beth A. Orrick, Kayla B. Briggs, Wendy Jo Svetanoff, Tolulope A. Oyetunji MD MPH, Shawn D. St Peter, and Richard J. Hendrickson
-

Implementation of a Transition Readiness Assessment and Transition Discussion Documentation in a Type 1 Diabetes Clinic
Sonalee Ravi
Background/Objective: Our institution utilizes a general transition readiness assessment to facilitate transition discussions. Patients rate six areas of knowledge, eight skills, and confidence in ability to transfer care successfully prior to age 22, then select a goal for their next visit. Discussions are documented in the medical record. Our aim was to implement this assessment with a 20% documentation rate after six months.
Methods: In March 2021, we trained providers and diabetes educators about the need for transition planning, the differences between transition planning and transfer, and the need for documentation. We added three diabetes-specific questions related to insulin adjustments, sexual function/pregnancy, and diabetes emergencies to the assessment tool. In April 2021, the transition assessment was implemented in clinic visits and all patients aged 17-years and older were asked to complete the assessment prior to their clinic visit. In June 2021, emails were jointly sent to providers and educators the Friday prior to visit indicating patients who needed transition assessments. Monthly data were pulled from the medical record that indicated percentage of eligible patients who had a documented discussion.
Results: Our clinic improved transition assessment documentation from 4.81% to 43.75% after six months. Conclusions: Our clinic successfully increased awareness and use of a general transition readiness assessment to guide transition planning. Future directions include utilizing clinic nurses to provide in-clinic reminders. We will also expand the assessment to younger ages to identify knowledge gaps and provide targeted education videos to improve self-management of diabetes and complete transfer of care.
-

Reimagining Bioethics Curricula: Centering Antiracism, Diversity, Equity, and Inclusion
Shika Kalevor, Marie-Laura Allirajah, Isabella Hernandez, and Phoebe Ozuah
As bioethicists, we engage with social, political, and health care systems that all center on relationality. Part of our responsibility in occupying space within these systems is recognizing where bias, power, and privilege lie, and how our positionality can either contribute to or take away from progress toward a morally conscious society. Bioethicists have the opportunity to remediate preventable harms and address issues of equity, justice, diversity, and oppression. We can also address these issues as core to our growing knowledge base. From our own experiences as bioethics students from multidisciplinary backgrounds, we know that these topics are not sufficiently addressed within academia or they are considered peripheral subjects. Educational institutions can play a role in instituting systemic change, intentional anti-racist practices, and more inclusive frameworks that confront the systems of oppression which contribute to health inequity.Many institutions of higher education released statements committing to address racism and white supremacy in the wake of the pandemic and racial reckoning of 2020. An academic curriculum that reflects these commitments as core to burgeoning bioethicists is a method of action against historical injustice that informs health disparity in care, outcomes, and experiences of the most marginalized.Our purpose is to examine what is included and what is excluded as core learning across three Master of Bioethics programs in the United States. In doing so, we aim to encourage institutions to begin a conversation about the creation of curricula that reflect our priorities as a field moving forward in this new landscape.
-

Umbilical Access in Laparoscopic Surgery in Infants less than 3 months: Single Institution Retrospective Review
James Fraser, Kayla B. Briggs, Wendy Jo Svetanoff, Rebecca M. Rentea, Pablo Aguayo, David Juang, Jason D. Fraser, Charles L. Snyder, Richard J. Hendrickson, Shawn D. St Peter, and Tolulope A. Oyetunji
PURPOSE: Umbilical access in laparoscopic surgery has been cited as a potential factor for increased complications in low birth weight infants and those less than three months old. Previous series noted a self-reported complication rate of 10.6% among 329 pediatric surgeons via anonymous survey, citing carbon dioxide (CO2) embolism as the most common complication. We report four-year outcomes with blunt transumbilical laparoscopic access to examine the safety of this technique. METHODS: Following IRB approval, a retrospective database of patients less than three months of age who underwent laparoscopic pyloromyotomy or inguinal hernia repair from 2016-2019 at a tertiary care academic center was reviewed. Operative reports, anesthesia records, post-operative documentation, and postoperative telephone calls were reviewed for complications related to umbilical access. Complications included bowel injury, bleeding umbilical vessels, umbilical vein cannulation, CO2 embolism, umbilical surgical site infection (SSI), umbilical hernia requiring repair, and death. RESULTS: Three hundred sixty-five patients met criteria for analysis (Table 1); 246 laparoscopic pyloromyotomy and 119 laparoscopic inguinal hernia repairs. Median age at operation was 5.9 weeks [4.3,8.8] and median weight was 3.9 kg [3.4,4.6]. Median operative time was 20 minutes [15,28]. Nine complications occurred for a total complication rate of 2.5%; 5 umbilical SSIs (1.4%), 1 bowel injury upon entry requiring laparoscopic repair (0.2%), 1 umbilical hernia requiring repair at 22 days after surgery (0.2%), and 2 cases of severe hypotension and bradycardia upon insufflation that resolved with exsufflation (0.5%). There were no intraoperative mortalities and no signs or symptoms of CO2 embolism. CONCLUSIONS: In this series umbilical access in laparoscopic surgery in neonates less than three months of age and less than 5kg was safe, with minimal complications.
-

Congenital Abnormalities of the Lower Airways and Lungs
Christopher M. Oermann
Goals and Objectives. Participants will be able to: Describe the 5 stages of fetal lung development. Summarize the prenatal identification and management of congenital abnormalities of the lower airways and lung (CALAL). Explain the classification of CALAL. Compare the clinical characteristics, pathology, and management of common CALAL. Discuss the long-term prognosis of CALAL.
-

HPV Cancer Free: Adolescent Vaccination
Sharon Humiston
Objectives:
1. Explain why HPV vaccine is important enough to be routinely recommended for young people (i.e., HPV cancer prevention).
2. Give an HPV vaccination recommendation that is effective and succinct using the same way, same day approach to the introduction of HPV vaccine.
3. Answer the most frequently asked questions about HPV vaccine accurately and succinctly.
-

Getting Back on Track with Cancer Prevention and Adolescent Immunizations
Sharon Humiston
Objectives:
1.Explain why HPV vaccine is important enough to be routinely recommended for young people (i.e., HPV cancer prevention).
2. Give an HPV vaccination recommendation that is effective and succinct using the same way, same day approach to the introduction of HPV vaccine.
3. Answer the most frequently asked questions about HPV vaccine accurately and succinctly.
-

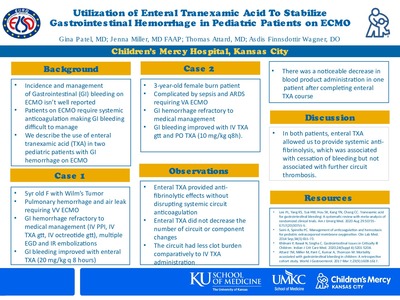
Utilization of Enteral Tranexamic Acid To Stabilize Gastrointestinal Hemorrhage in Pediatric Patients on ECMO
Gina Patel, Jenna Miller, Thomas M. Attard, and Asdis Finnsdottir Wagner
Background:
Incidence and management of Gastrointestinal (GI) bleeding on ECMO isn’t well reported Patients on ECMO require systemic anticoagulation making GI bleeding difficult to manage We describe the use of enteral tranexamic acid (TXA) in two pediatric patients with GI hemorrhage on ECMO




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}