
-

Respiratory Viral Infections in School KIDS
Sydnie Petty, Amanda Hayes, Anjana Sasidharan, Dithi Banerjee, Rangaraj Selvarangan, Jennifer Goldman, and Jennifer E. Schuster
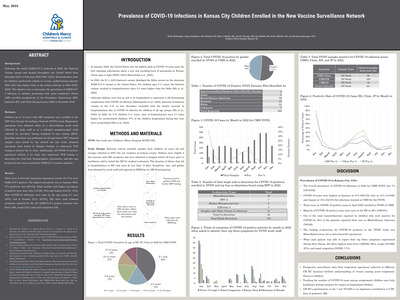
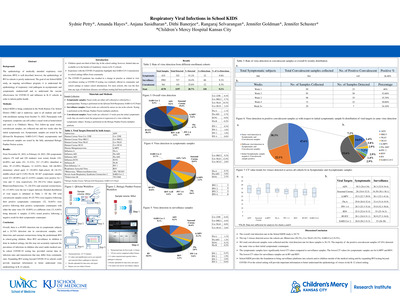
Background: The epidemiology of medically attended respiratory viral infections (RVI) is well described, however, the epidemiology of RVI in schools is poorly understood. The goal of our School KIDS study, an ongoing surveillance program, is to understand the epidemiology of respiratory viral pathogens in asymptomatic and symptomatic students/staff and to understand the vaccine effectiveness for COVID-19 and influenza in K-12 schools in order to inform public health.
Methods: School KIDS is being conducted in the North Kansas City School District (NKC) and is underway; open to all students and staff, with enrollment starting from October 31, 2022. Participants with respiratory symptoms can self-collect a nasal swab at home/school and send it to Children's Mercy. Two follow-up nasal swabs, convalescent samples, are collected one and two weeks after the initial symptomatic test. Symptomatic samples are tested by the QIAstat-Dx Respiratory SARS-CoV-2 Panel; asymptomatic and convalescent samples are tested by the fully automated Hologic Panther Fusion system.
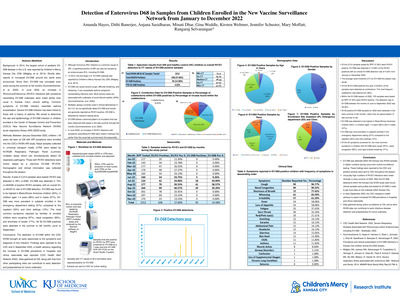
Results: From November 01, 2022, to February 24, 2023, 298 symptomatic subjects (70 staff and 228 students) were tested; female (191, 64.09%) and males (93, 31.21%). 213 (71.48%) identified as white, 39 (13.09%) Hispanic, 12 (4.03%) black. 140 (46.98%) elementary school aged, 31 (10.40%) high-school, 48 (16.1%) middle-school and 9 (3.0%) Pre-K. Of 467 symptomatic samples tested 233 (49.89%) and 23 (4.93%) samples were positive for 1 virus and >1 virus respectively; 234 (50.11%) where negative. Rhinovirus/Enterovirus, 73, (28.52%) and seasonal coronaviruses, 63, (13.49%) were the top 2 targets detected. Detailed distribution of viral targets is tabulated in Table 1. Of the 190 total convalescent samples tested, 49 (25.79%) were negative following their positive symptomatic counterpart; (32, 16.84%) were positive following their positive symptomatic counterparts with either the same virus (19, 10.00%) or a different virus (13, 6.84%) being detected. 6 samples (3.16%) tested positive following a negative result for their symptomatic counterpart.
Conclusion: Overall, there is a 49.89% detection rate in symptomatic subjects and a 24.74% detection rate in convalescent samples, with rhinovirus and seasonal coronaviruses being the predominant RVI in school-going children. Most RVI surveillance in children is done in medical settings, but this may not accurately represent the prevalence of infections in children who aren't under medical care. In-school COVID-19 testing has provided current data on infection rates and transmission that may differ from community rates. Expanding RVI testing beyond COVID-19 in schools could provide important information to better understand virus epidemiology in K-12 schools.
-

Right ventricular dysfunction is common among pediatric patients with acute respiratory distress syndrome on venovenous ecmo
Cara Holton, Sanket Shah, and Jenna Miller
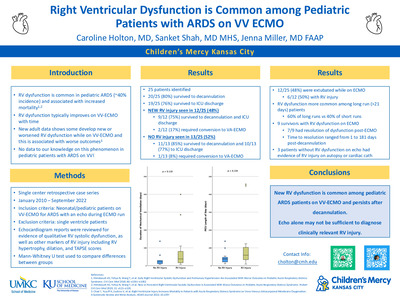
Intro: The presence of right ventricular (RV) dysfunction is common among pediatric and adult patients with acute respiratory distress syndrome (ARDS) and is associated with increased mortality. Typically, RV dysfunction that is secondary to ARDS improves with cannulation to venovenous (VV) extracorporeal membrane oxygenation (ECMO). However, some adult patients develop new RV dysfunction on ECMO that is associated with worse outcomes. No published studies have evaluated the incidence and outcomes of RV dysfunction among pediatric patients on VV ECMO for ARDS.
Methods: A single center retrospective case series was conducted from January 2010 to September 2022. 25 neonatal and pediatric patients cannulated on VV ECMO for ARDS with an echocardiogram performed during their ECMO run were included. Single ventricle patients were excluded. Echocardiogram reports were reviewed for evidence of qualitative systolic dysfunction.
Results: The majority (23/25, 92%) of patients were cannulated using a dual lumen cannula. Overall, 20/25 (80%) survived to decannulation and 19/25 (76%) survived to ICU discharge. About half (12/25, 48%) had echo evidence of new RV dysfunction during their ECMO run. Of the patients without RV dysfunction, 11/13 (85%) survived to decannulation and 10/13 (77%) survived to ICU discharge. Survival to decannulation and ICU discharge was slightly lower among those with RV dysfunction (9/12, 75%). Despite the high incidence of RV dysfunction, only 3 patients required conversion from VV to VA - 2 due to pulmonary hypertensive crisis with associated RV dysfunction and 1 due to cannula thrombus.
Patients with RV dysfunction had a trend towards longer ECMO run, duration of mechanical ventilation, ICU length of stay and hospital length of stay. RV dysfunction was more common in patients with ECMO runs greater than 21 days (6/10, 60%) compared to those with shorter runs (6/15, 40%). The majority of survivors with RV dysfunction continued to have abnormal echos following decannulation and time to resolution on echo varied from 1 to 181 days after decannulation. Of note, autopsy results, cardiac cath findings and post-ICU deaths in several patients demonstrated failure to diagnose clinically relevant RV injury by echo alone.
Conclusion: New RV dysfunction is common among pediatric patients on VV ECMO for ARDS and is associated with worse outcomes. As VV ECMO becomes increasingly more common it is prudent for providers to evaluate for RV dysfunction as a potential complication and early prognostic imaging marker, especially among patients on ECMO for extended periods of time.
-

SARS-CoV-2 Envelope Protein Tolerizes Macrophage Response to Secondary Inflammatory Stimuli
Stephen Pierce, Rebecca McLennan, Santosh Khanal, Heather Menden, Venkatesh Sampath, and Todd Bradley
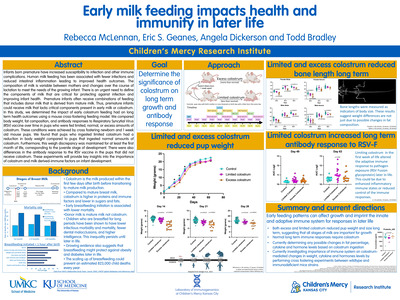
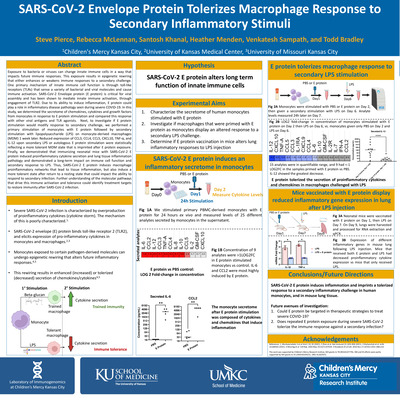
Exposure to bacteria or viruses can change innate immune cells in a way that impacts future immune responses. This exposure results in epigenetic rewiring that either enhances or weakens immune responses to a secondary challenge. One primary mechanism of innate immune cell function is through toll-like receptors (TLRs) that sense a variety of bacterial and viral molecules and cause immune activation. SARS-CoV-2 Envelope protein (E protein) is critical for viral assembly and has been shown to mediate innate immune activation, through engagement of TLR2. Due to its ability to induce inflammation, E protein could play a role in inflammatory disease pathology seen during severe COVID-19. In this study, we determined the secretome of chemokines, cytokines and growth factors from monocytes in response to E protein stimulation and compared this response with other viral antigens and TLR agonists. Next, to investigate if E protein stimulation would modify response to secondary challenge, we performed a primary stimulation of monocytes with E protein followed by secondary stimulation with lipopolysaccharide (LPS) on monocyte-derived macrophages (MDM) 1 week later. Reduced expression of CCL3, CCL4, CCL5, CXCL10 TNF-A, and IL-12 upon secondary LPS or autologous E protein stimulation were statistically reflecting a more tolerant MDM state that is imprinted after E protein exposure. Finally, we demonstrated that immunizing neonatal mice with SARS-CoV-2 E protein induced proinflammatory cytokine secretion and lung tissue inflammation pathology and demonstrated a long-term impact on immune cell function and secondary response to LPS. Thus, SARS-CoV-2 E protein induces macrophage proinflammatory networks that lead to tissue inflammation, but also induce a more tolerant state after return to a resting state that could impact the ability to respond to secondary infection. Further understanding of the molecular pathways that drive this immune activation and tolerance could identify treatment targets to restore immunity after SARS-CoV-2 infection.
-

Shared in Rare: Engaging Stakeholders to Develop a Shared ELSI Research Agenda Across Rare Diseases
Courtney D. Berrios, Jeremy R. Garrett, Linda Jones, Nancy Petersen, Meghan Strenk, and Rare Voices Advisory Group
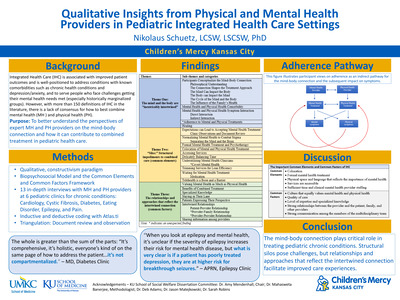
Research on individual rare diseases presents challenges such as small sample sizes and limited funding sources, while research efforts spanning across rare diseases present difficulty in applying outcome measures to conditions with variable manifestations. Common experiences in rare disease (extended diagnostic odyssey, chronic conditions, need for advocacy, and challenges finding and managing multi-specialty care) create shared ethical, legal, and social issues (ELSI). Shared in Rare is a stakeholder engagement project to leverage the shared experiences of patients and families impacted by rare disease to develop an ELSI research agenda that is both applicable across rare diseases and guided by patient and family priorities.
A stakeholder group, Rare Voices (RV), is collaborating with ELSI and community engaged researchers to complete the project. RV includes 4 teens and 12 parents of children impacted by rare disease and 6 clinicians/researchers. This project team is working together to conduct listening sessions with diverse parents, caregivers, and teens in the rare disease community that will inform development of the ELSI research agenda.
Early engagement with RV members revealed anticipated challenges including identifying research topics across all rare diseases, communication across diverse stakeholders, moving from qualitative listening session data to research questions, and addressing stakeholder feelings about traumatic experiences surfaced by the project work. This input informed modifications to the project plan including participatory RV training in qualitative research utilizing interviews with RV parent members and collaborative development of research questions emerging from those interviews. Frequent small group work has been incorporated to facilitate communication and engagement. A trauma workgroup was formed and completed training to integrate trauma sensitive practices into all project activities.
This incorporation of stakeholder input has built a highly collaborative and engaged project team working equitably to reach the project aims. 17/22 (77%) of RV members are directly involved in the listening sessions as part of teams developing recruitment materials, drafting the discussion guide, and moderating listening sessions. The team’s actions to address anticipated challenges inform future stakeholder engagement and the collaboration in every aspect of this project poised the listening sessions to capture the voice of the rare disease community, facilitating identification of research needs that will inform a patient and family-centered ELSI research agenda to improve care for rare diseases.
-

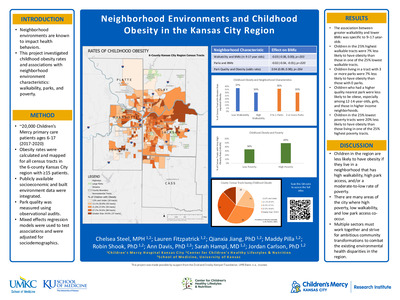
Socioeconomic factors and PICU interventions in high mortality risk asthmatics
Hanh Ho, Paul N. Bauer, and Jade B. Tam-Williams
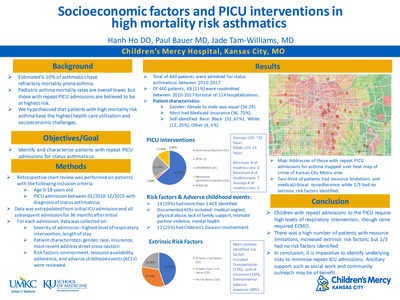
Background: Asthma mortality rates are overall lower in children, but studies estimate 5-10% of asthmatics have refractory mortality prone asthma. Asthmatics with repeat pediatric intensive care unit (PICU) admissions are believed to be at high mortality risk with increased health care utilization and socio-economic challenges.
Objectives/Goal: We aim to identify patients with repeat PICU admissions for status asthmaticus and characterize the levels of interventions and socio-economic status.
Methods: A retrospective chart review was done on patients with the following inclusion criteria: age 0-18, PICU admission between January 2010 to December 2015, and a diagnosis of status asthmaticus on admission. Data was extrapolated from initial ICU admission at any given year, and all subsequent admissions, at least 36 months from date of initial admission. Highest level of respiratory intervention, length of stay, gender, race, insurance, and risk factors (e.g. environment, resource availability, adherence, adverse childhood events) were reviewed.
Results: 440 patients were admitted for asthma to the PICU between 2010-2017. Of those 440, 48 (11%) were readmitted between 2010-2017 for a total of 114 hospitalizations. Interventions for each admission were: 72 (63%) continuous albuterol, 3 (2%) HFNC, 25 (22%) CPAP/BIPAP, 14 (12%) mechanical ventilation/intubation and 0% ECMO. The average stay was ~32 hours (range: 20 min to 204 hours). The ratio of female to male was equal (24:24, 50%). 32 (67%) were Black, 12 (25%) were White, 1 was American Indian and 3 were Other. Most had Medicaid insurance (36, 75%). 32 patients had at least 1 risk factor; 22 had >1 risk factors; 16 patients had none identified. 7 (15%) identified transportation limitation, 6 (13%) had lack of insurance. 19% reported environmental tobacco smoke. ACEs were reviewed; 14 (30%) reported one or more ACE (medical neglect, physical abuse, lack of family support, intimate partner violence, mental health); 12 (25%) had Children’s Division involvement.
Conclusion: Children with repeat admissions to the PICU require higher levels of respiratory interventions. Within this group, 2/3 had resource limitations and medical/clinical nonadherence while 1/3 had intrinsic factors that may have contributed to repeat admissions to PICU. It is significant that 1/3 of these children had experienced at least 1ACE and ¼ had Children’s Division involvement. Therefore, in this cohort, it is imperative to identify underlying risks, including social work involvement and outreach to improve asthma care.
-

State Spending on Public Benefit Programs and the Differential Impact on Child Maltreatment by Race and Ethnicity
Henry T. Puls, Matthew Hall, Reiko Boyd, and Paul J. Chung
Background:
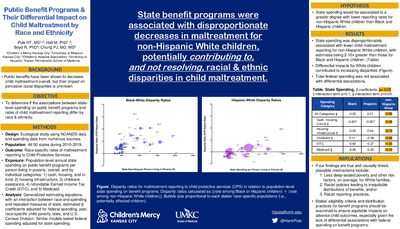
State spending on programs with the capacity to mitigate poverty have been shown to reduce child maltreatment overall. However, given pervasive racial/ethnic disparities across child maltreatment outcomes, it remains unclear if current spending and policies have different effects on child maltreatment by race/ethnicity.
Objective:
To determine if associations between state-level spending on public benefit programs and rates of child maltreatment reporting differ by race and ethnicity. We hypothesized that inverse associations between spending and maltreatment would be greater for non-Hispanic White children than for non-Hispanic Black or Hispanic children.
Design/Methods:
This was an ecological study of all U.S. states during Federal fiscal years 2010-2019. The primary exposure was states’ total annual spending per person living below the Federal poverty limit on local, state, and federal benefit programs, which was the sum of 1) cash, housing, and in-kind assistance, 2) housing infrastructure, 3) childcare assistance, 4) refundable Earned Income Tax Credit, and 5) Medical Assistance Programs. The outcome was race/ethnicity-specific rates of maltreatment reporting to Child Protective Services. Generalized estimating equations, with an interaction between race and spending and repeated measures of states, estimated β coefficients and 95% confidence intervals (CI) after adjustment for federal spending, year, and race/ethnicity-specific child poverty rates.
Results:
There were 493 state-year observations after exclusions for missing maltreatment data. The relationship between total spending and maltreatment reporting differed significantly by race/ethnicity (p= 0.029). There was an inverse association between total state spending and maltreatment reporting for non-Hispanic White children (β= -0.043 [CI -0.0782, -0.0076]) but not for non-Hispanic Black or Hispanic children. Likewise, inverse associations were significant for only non-Hispanic White children with respect to spending on housing infrastructure, childcare assistance, Earned Income Tax Credit, and Medical Assistance Programs (Table).
Conclusions:
Public benefits may be disproportionately received by or effective in preventing maltreatment for non-Hispanic White children, potentially perpetuating racial/ethnic disparities in child maltreatment. Benefit programs’ eligibility criteria and distribution strategies should be carefully examined to ensure equitable impacts mitigating adverse child outcomes.
-

Stem Like T Cells in Anti-cancer Immunosurveillance Against Therapy-resistant Pediatric Cancer
Fang Tao, Sara McElroy, Jacqelyn Nemechek, Irina Pushel, Santosh Khanal, John Szarejko, Todd Bradley, Douglas Myers, and John M. Perry
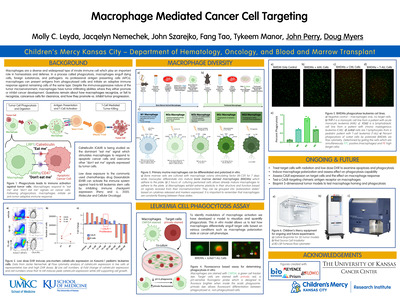
Leukemia is the most commonly diagnosed pediatric cancer. Acute lymphoblastic leukemia (ALL) has an 85% 5-year-survival rate; yet 20% of patients experience relapse driven by therapy-resistant cells and do not survive long-term. The Wnt/β-catenin and PI3K/Akt signalling pathways interact to confer resistance to cancer therapies. We previously found low dose doxorubicin (DXR) specifically target therapy-resistant leukemic stem cells (LSCs) by inhibiting immune check point genes on LSCs in a T-cell acute lymphoblastic leukemia (T-ALL) mouse model. However, the cellular and molecular mechanisms of how low DXR functions to achieve this anti-cancer immunity are not well understood. Wnt signaling was shown to arrest effector cell differentiation and generate memory stem cells, which preserves anti-tumor potential. As DXR inhibits the cooperative interaction of Akt and β-catenin, we hypothesized that low DXR facilitates immune reactivation against resistant LSCs by regulating stem-like T cells. In this study, we investigated multiple populations of CD8+ T cells, especially the stem-cell like T cells in T-ALL. We found low dose doxorubicin increased the naïve T cell and stem-like T cell pool. Moreover, our flow cytometry and single-cell sequencing analysis of LSCs and blast cells revealed upregulation of stem-like T cell gene signature after low DXR treatment, but not after conventional chemotherapy. Further functional analysis of the CD8 T cells reactive to leukemia is ongoing by in vitro culture. Meanwhile, we characterized T cells in patients with minimal residual disease (MRD). We found that MRD negative patients were presented with more naïve T cells, and enhanced polyfunctionality in their T cells. These cells may ultimately be pharmacologically stimulated by low DXR while genetically engineered to express chimeric antigen receptors, allowing application of adoptive immunotherapy based on the tumor-specific stem-like T cells and preventing relapse in patients treated with immunotherapy.
-

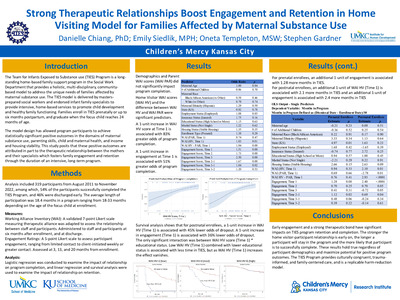
Strong Therapeutic Relationships Boost Engagement and Retention in Home Visiting Model for Families Affected by Maternal Substance Use
Danielle Chiang, Emily Siedlik, Oneta Templeton, and Stephen Gardner
The Team for Infants Exposed to Substance use (TIES) Program is a home-based family support program in the Social Work Department that provides a holistic, multi-disciplinary, community-based model to address the unique needs of families affected by maternal substance use. The TIES model, now in its 30th year, is delivered by masters-prepared social workers along with endorsed infant family specialists to provide intensive, home-based services to promote child development and healthy family functioning. The design of the two-role model addresses gaps and challenges identified in other home visiting programs, including poor participant engagement and retention. The model design has allowed program participants to achieve statistically significant positive outcomes in the domains of maternal substance use, parenting skills, child and maternal health, and income and housing stability. This study posits that these positive outcomes are attributed in part to the therapeutic relationship between the mothers and their specialists which fosters family engagement and retention through the duration of an intensive, long-term program.
Data were collected from 2012 to September 2022 from 235 participants, among which, 67% of the participants successfully completed the TIES Program, and 33% were discharged early. The average length of participation was 19.8 months in a program ranging from 18-33 months depending on the age of the focus child at enrollment. The Working Alliance Inventory (WAI), a validated scale measuring therapeutic alliance, was adapted to assess the relationship between staff and participants. The scale was administered to staff and participants once six months after enrollment, and once at discharge. Logistic regression was conducted to examine the impact of relationship on program completion, and linear regression was conducted to examine the impact of relationship on length of program participation.
Preliminary results indicated that a 1 unit increase in relationship leads to 2.2 times greater odds of program completion. In addition, each 1-point increase in relationship leads to 1.63-1.65 more months of program participation. The upcoming full analysis will examine the moderating effects of participants’ demographics and virtual visits. These initial results showed that the therapeutic relationship has a significant impact on program engagement and retention. The stronger the relationship is, the longer a participant will stay in the program. The results speak to the importance of building relationship and bonding with participants early on for better program outcomes.
-

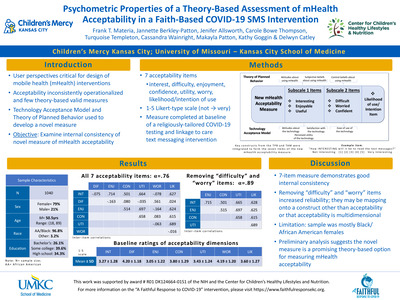
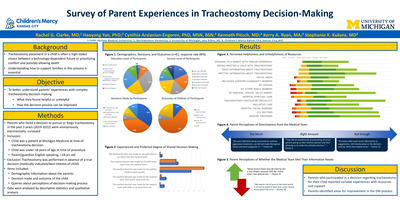
Survey of Parental Experiences in Tracheostomy Decision-Making
Rachel G. Clarke, Haoyang Yan, Cynthia Arslanian-Engoren, Kenneth Pituch, Kerry A. Ryan, and Stephanie Kukora
Background
Tracheostomy placement in a child is often a high-stakes choice between a technology-dependent future or prioritizing comfort and possibly allowing death. Understanding how to support families in this process is essential.
Objective
We surveyed parents who faced a decision regarding tracheostomy for their child to better understand their experiences with complex tracheostomy decision-making (DM).
Design/Methods
Children for whom a tracheostomy was considered from 2019-2022 at a single quaternary center were identified using medical record term search. Cases where tracheostomy was ethically obligated (best interest of child) were excluded. Participants were electronically surveyed. Queries included perceptions of their child’s tracheostomy DM process and outcome, suggestions to improve DM (free-text response), Illness Cognition Questionnaire (ICQ), and demographics. Survey items were refined by content and decision-science experts. Data were analyzed by descriptive statistics, two-sample t test or fisher’s exact test as appropriate, and qualitative analysis.
Results
There were 61 completed surveys (response rate 49%). Demographic data shown in Table 1. 66% of parents reported pressure to decide quickly, though reported time for DM varied. 26% did not feel they were offered a choice, despite exclusion of patients for whom tracheostomy was obligated. 25% reported mismatch between how the decision was made with the medical team and how they thought it ought to have been made. Parents’ experience with and perceived helpfulness of resources are shown in Figure 1. Though most parents found the medical team helpful, 10% reported their intensive care physicians were unhelpful. 31% reported not experiencing palliative care. None of the parents who watched video-information (64%), received written information (85%), or met or saw a child with a tracheostomy (41%) found these experiences unhelpful. 71% of parents with living children reported life after tracheostomy DM better than expected, with a non-distressed level of helplessness (M=10.49, SD=2.97) and high acceptance of their child’s illness (M=20.55, SD=3.16) (subscale range:6–24) on ICQ scale. Perception of pressure, choice, helpfulness, and ICQ scores did not differ by the decision made.
Free-text responses described aspects of the DM process parents found helpful (n=53 responses) or unhelpful (n=50). Major themes and exemplary quotes in Table 2.
Conclusion
Parents who participated in a decision regarding tracheostomy for their child reported variable experiences with resources and support. Parents identified areas for improvement in the DM process.
-

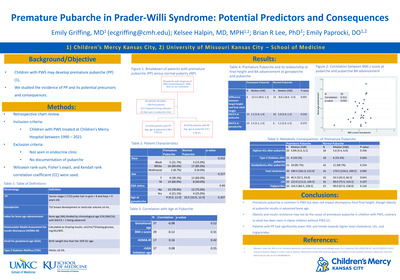
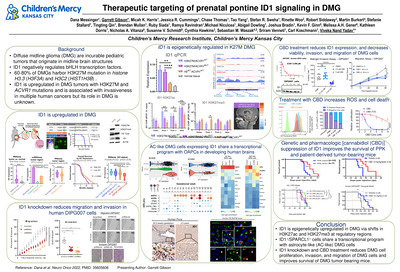
Therapeutic targeting of prenatal pontine ID1 signaling in DMG
Dana Messinger, Garrett Gibson, Micah K. Harris, Jessica R. Cummings, Chase Thomas, Tao Yang, Stefan R. Sweha, Rinette Woo, Robert Siddaway, Martin Burkert, Stefanie Stallard, Tingting Qin, Brendan Mullan, Ruby Siada, Ramya Ravindran, Michael Niculcea, Abigail Dowling, Joshua Bradin, Kevin F. Ginn, Melissa A H Gener, Kathleen Dorris, Nicholas A. Vitanza, Susanne V. Schmidt, Cynthia Hawkins, Sebastian M. Waszak, Sriram Venneti, and Viveka Nand Yadav
Diffuse intrinsic pontine glioma (DIPG) is a highly aggressive brain tumor with rare survival beyond two years. This poor prognosis is largely due to the tumor's highly infiltrative and invasive nature. Nearly 80% of DMGs harbor K27M mutation in the genes encoding histones H3.1 (H3F3A) or H3.3 (HISTIH3B) variants, often with concurrent mutation in ACVR1. Inhibitor of DNA-binding (ID) proteins are key transcriptional regulators of genes involved in lineage commitment and associated with invasiveness and poor clinical outcomes in multiple human cancer. Prior work showed that recurrent K27M and ACVR1 mutations increase ID1 expression in cultured astrocytes, but this has not been confirmed in human tumors or therapeutically targeted. We developed an in-utero electroporation (IUE) murine H3K27M-driven tumor model, which demonstrates increased ID1 expression in H3K27M- and ACVR1-mutated tumor cells. Exome and transcriptome sequencing analysis of multi-focal DMG tumors (n=52) and normal brain tissue revealed that increased ID1 expression is associated with H3K27M/ACVR1-mutation, brainstem location, and correlates with poor survival in patients. ChIP sequencing for H3K27ac and H3K27me3 in multiple DMG tumors (n=5) revealed that ID1 gene is epigenetically active, which matches the epigenetic state of murine prenatal hindbrain cells. Higher ID1-expressing astrocyte-like DIPG cells share a similar transcriptional program with ID1+/SPARCL1+ positive oligo/astrocyte-precursor (OAPC) cells from the developing human brain and demonstrates upregulation of gene sets involved with regulation of cell. Both genetic and pharmacologic [cannabidiol (CBD)] suppression of ID1 results in decreased DIPG cell invasion/migration in vitro and invasion/tumor growth in multiple in vivo models. Mechanistically, CBD reduces proliferation through reactive oxygen species production. Further, DIPG patients treated off-trial with CBD (n=15) showed reduced ID1 expression and improved overall survival. In summary, ID1 is upregulated in DIPG through K27M mediated epigenetic reactivation of a developmental OAPC transcriptional state, and ID1-driven invasiveness of DIPG is therapeutically targetable with CBD.
-

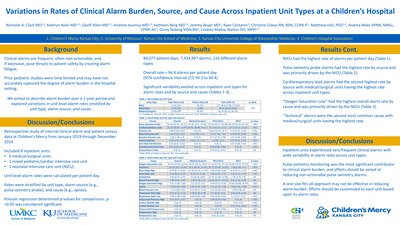
Variations in Rates of Clinical Alarm Burden, Source, and Cause Across Inpatient Unit Types at a Children’s Hospital
Nicholas Clark, Kathyrn Kyler, Geoffrey L. Allen, Andrew Ausmus, Kathleen Berg, Jeremy Beyer, Ryan Centanni, Christine Claeys, Matthew Hall, Andrea Miles, Ginny Nyberg, and Lindsey Malloy-Walton
Introduction: Clinical alarms are frequent, often non-actionable, and, if excessive, pose threats to patient safety by creating alarm fatigue. Prior pediatric studies were limited and may have not accurately captured the degree of alarm burden in the hospital setting. We aimed to describe alarm burden over a 1-year period and explored variations in alarm rates stratified by unit type, alarm source, and cause.
Methods: We conducted a retrospective study of internal clinical alarm and patient census data at Children’s Mercy from January 2019 through December 2019, including 8 inpatient units: 6 medical/surgical (M/S), 1 pediatric intensive care unit (PICU), and 1 neonatal intensive care unit (NICU). Alarm rates per patient day were calculated. Rates were stratified by unit type, alarm source (e.g., pulse oximetry probe), and cause (e.g., apnea). Poisson regression determined p-values for comparisons.
Results: There were 84,077 patient days and 7,934,997 alarms included. Overall rate of 94.4 alarms per patient day (95% confidence interval [CI] 94.3 to 94.4; Table 1). Significant differences in overall alarm rates existed across inpatient unit types (117.5 NICU vs 90.7 PICU vs 81.3 M/S; p<.001). Pulse oximetry probe alarms had highest rate by source (54.4; 95%CI 54.3 to 54.4) followed by cardiorespiratory leads (31.0; 95%CI 31.0 to 31.1). There was significant variation in alarm rates by source across unit types. PICU had lowest rate of pulse oximetry probe alarms (92.6 NICU vs 33.3 PICU vs 37.6 M/S; p<.001), while NICU had lowest rate of cardiorespiratory lead alarms (16.2 NICU vs 31.4 PICU vs 40.1 M/S; p<.001). Similarly, alarms stratified by cause displayed significant variation across unit types with low oxygen saturation alarms having highest overall rate (43.4; 95%CI 43.3 to 43.4) followed by technical alarms (16.3; 95%CI 16.3 to 16.4). Intensive care units had higher rates of low oxygenation alarms compared to M/S (79.6 NICU vs 27.1 PICU vs 26.3 M/S; p<.001), but lower rates of technical alarms (3.4 NICU vs 15.8 PICU vs 24.5 M/S; p<.001).
Conclusions: Our inpatient units experienced very frequent clinical alarms with wide variability in alarm rates across unit types. By studying alarm rates over a full year, our work builds upon existing literature showing that alarms arising from pulse oximetry monitoring are the most significant contributor to clinical alarm burden at children’s hospitals, but that unit type may play a role in alarm burden. Efforts should be aimed at reducing non-actionable pulse oximetry alarms.
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}