
Publication Date
9-2025
Files
Download Full Text (416 KB)
Abstract
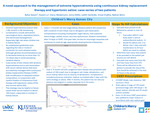
Hypernatremia is defined as a serum sodium greater than 145 mEq/L and is due to either a deficit of free water or excess sodium intake. Extreme hypernatremia (sodium level > 190 mEq/L) is immediately life–threatening with mortality rates > 60%. It is especially challenging to avoid complications, such as permanent neurological injury, respiratory failure, and profound electrolyte derangement, when children are in kidney failure. Established guidelines are lacking for correcting such extreme levels due to a paucity of information in the literature, although general recommendations are to decrease levels by no more than 10-12 mEq/L per day to prevent neurological complications. We report a case series of two infants with extreme hypernatremia due to salt intoxication with anuric kidney failure that were successfully managed with continuous kidney replacement therapy (CKRT) with modification of dialysate sodium composition, in conjunction with careful titration of intravenous fluid therapy. The first case involved a 3-month-old with end stage kidney disease, with home peritoneal dialysis use, presenting with a sodium of 222 mEq/L due to iatrogenic salt intoxication. Complications included multisystem organ failure, subdural hemorrhage, cardiac arrest with subsequent myocardial dysfunction requiring multiple inotropes, respiratory failure, and severe liver dysfunction. Sodium levels normalized over 10 days of “stairstep” CKRT with sodium additives with fine-tuning hypertonic saline and normal saline (See Figure 1). One year later, he has no neurologic sequelae and continues to meet all age-appropriate developmental milestones. The second case was a 9- month-old with congenital heart disease who presented with sodium of 196 mEq/L due to iatrogenic salt intake, severe dehydration, and anuric kidney failure. Complications included pulmonary embolism. Her sodium was corrected after 5 days with the same strategy as above (See Figure 2). At 4-month follow-up, no adverse neurological or cardiac sequelae were noted. Both CKRT prescriptions utilized low clearance of 500 ml/min/1.73m2 and every 12-24 hours CKRT dialysate bags were changed to achieve a sodium reduction of about 10 meq/L per day. In summary, this presents a novel approach to severe hypernatremia in patients with acute or chronic kidney failure through individualized CKRT strategies and judicious fluid therapy.
Disciplines
Nephrology | Pediatrics
Recommended Citation
Barani, Bahar; Lu, Xuexin; Weidemann, Darcy; Vansickle, Judith; Chadha, Vimal; and Beins, Nathan, "A Novel “Stairstep” Approach to the Management of Extreme Hypernatremia Using Continuous Kidney Replacement Therapy and Hypertonic Saline" (2025). Posters. 481.
https://scholarlyexchange.childrensmercy.org/posters/481



Notes
Presented at the 5th International Symposium on Acute Kidney Injury in Children; September 26-28, 2025; Cincinnati, OH.